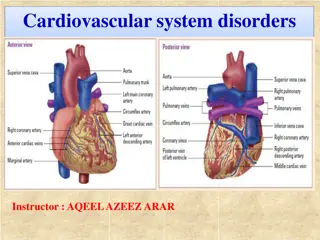
Coronary Revascularization: Anatomy vs. Physiology

Coronary Revascularization:
Anatomy vs. Physiology
S. Elissa Altin, MD
Assistant Professor
Yale University
VA Connecticut
Disclosures
I have no disclosures.
Learning Objectives
•
Prevalence of angina in women
•
Prevalence of non-obstructive disease in women
•
Anatomy vs. physiology for lesion assessment
•
FFR
•
iFR
•
Microvascular disease measures in women
Angina Prevalence in Women
•
Angina is more prevalent among
women
than men (pooled random-
effects sex ratio of 1.20 [95% CI 1.14
to 1.28], P<0.0001).
•
Among Americans, ratio was 1.40
[95% CI 1.28 to 1.52], with non-
whites>whites
Hemingway et al.
Circulation
2008;117:1526
Stable Angina Portends Worse Outcomes,
Regardless of Anatomy in Men and Women
Jesperson et al.
EHJ
2012.
Learning Objectives
•
Prevalence of angina in women
•
Prevalence of non-obstructive disease in women
•
Anatomy vs. physiology for lesion assessment
•
FFR
•
iFR
•
Microvascular disease measures in women
38% obstructive
coronary
artery
disease
% of total patients
N=397,954
N=149,739
0
20
40
60
80
100
120
Pre-Coronary Angiography
Post-Coronary Angiography
Better Diagnostic Methods Are Needed To Stratify
Patients For Coronary Angiography
National Cath Lab Data Registry:
•
62% of patients undergoing elective cardiac
catheterization do not have obstructive CAD
•
Majority of patients (84%) received noninvasive
diagnostic tests
prior to referral to
catheterization
Low yield at invasive angiography is a
diagnostic challenge
Patel MR et al.
Patel MR et al.
N Engl J Med
N Engl J Med
2010;362:886-95.
2010;362:886-95.
Significant CAD by Sex and Ethnicity in Stable Angina
Shaw et al.
Circulation
2008 ;117:1787
•
Women have
significantly less
obstructive CAD
independent of
ethnicity
9
In ACS Non-Obstructive CAD is more Common in Women
•
Up to 20% of ACS patients
referred for angiography have
no significant CAD
•
Of these
~60% are women and
40% are men
Bugiardini et al. JAMA 2005;293:477-484
Daly et al. Circulation 2006;113:490-498
Learning Objectives
•
Prevalence of angina in women
•
Prevalence of non-obstructive disease in women
•
Anatomy vs. physiology for lesion assessment
•
FFR
•
iFR
•
Microvascular disease measures in women
Accuracy of Visual Assessment
PVA, Physician visual assessment; QCA, quantitative coronary angiography
20% overestimation
of
lesion severity by
physician visual
assessment compared
to quantitative
angiography
Zhang et al.
JAMA Internal Medicine
2018.
Anatomy vs. Physiology Based Outcomes
Johnson et al.
Circ: Cardiovasc Imaging
2013.
Learning Objectives
•
Prevalence of angina in women
•
Prevalence of non-obstructive disease in women
•
Anatomy vs. physiology for lesion assessment
•
FFR
•
iFR
•
Microvascular disease measures in women
Women have higher FFR for given degree of
stenosis than men (LAD)
Kang et al.
JACC CI
2013.
•
No sex difference in anatomic
stenosis severity
•
Women have higher FFR
values at maximum
hyperemia compared with
male patients with the same
degree of LAD stenosis
FAME: Women have higher FFR values for the
same degree of stenosis
Kim et al.
JACC CI
2012.
FFR-Guided PCI Equally Beneficial in Men and Women
Kim et al.
JACC CI
2012.
Learning Objectives
•
Prevalence of angina in women
•
Prevalence of non-obstructive disease in women
•
Anatomy vs. physiology for lesion assessment
•
FFR
•
iFR
•
Microvascular disease measures in women
DEFINE-FLAIR Sub-study
Kim et al.
JACC CI
2019.
•
FFR-guided strategy was associated
with a higher rate of revascularization
than iFR-guided strategy in men
, but
not in women.
•
No sex differences in outcomes
for
FFR vs iFR guided interventions
Learning Objectives
•
Prevalence of angina in women
•
Prevalence of non-obstructive disease in women
•
Anatomy vs. physiology for lesion assessment
•
FFR
•
iFR
•
Microvascular disease measures in women
IMR similar between men and women, CFR
lower (but due to increased resting flow)
Kobayashi et al.
JACC CI
2015.
Morrow et al.
BMJ Case Report
2019.
Is Microvascular Dysfunction the Underlying Cause of
Angina in Women without Obstructive CAD?
1.
Confirms that CFR is lower
in women than men
2.
BUT…Microvascular
function (IMR) is the same
for men and women.
3.
CFR is lower due to shorter
resting transit time (OR
higher coronary flow at rest)
in women
K
e
y
F
i
n
d
i
n
g
s
•
IMR is a direct hyperemic
measure; eliminates variability of
resting vascular tone
•
Resting transit time subject to
substantial variation due to
resting hemodynamics (BP, HR,
contractility, coronary pathology)
Kobayashi et al.
JACC CI
2015.
Resting Transit Time and Coronary Flow:
Predictors
•
Short transit time=higher
coronary flow
•
Predictors of shorter
transit time at rest
•
Female sex
(p=0.006)
•
HTN (p=0.02)
•
Smaller vessels (NS)
Adverse prognosis of abnormal CFR likely multifactorial:
Atherosclerosis
: Early macrovascular disease
Microvascular Dysfunction
Non-Atherosclerosis:
HTN, diastolic dysfunction,
compounded by other risk factors common to women
including insulin resistance, metabolic syndrome,
diabetes
This content discusses the prevalence of angina in women compared to men, the importance of stable angina in predicting outcomes, the need for better diagnostic methods for coronary angiography, and the differences in obstructive CAD by sex and ethnicity in stable angina cases. It highlights the challenges and considerations in evaluating and managing coronary artery disease, particularly in women.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Coronary Revascularization: Anatomy vs. Physiology S. Elissa Altin, MD Assistant Professor Yale University VA Connecticut
Disclosures I have no disclosures.
Learning Objectives Prevalence of angina in women Prevalence of non-obstructive disease in women Anatomy vs. physiology for lesion assessment FFR iFR Microvascular disease measures in women
Angina Prevalence in Women Angina is more prevalent among women than men (pooled random- effects sex ratio of 1.20 [95% CI 1.14 to 1.28], P<0.0001). Among Americans, ratio was 1.40 [95% CI 1.28 to 1.52], with non- whites>whites Hemingway et al. Circulation 2008;117:1526
Stable Angina Portends Worse Outcomes, Regardless of Anatomy in Men and Women Jesperson et al. EHJ 2012.
Learning Objectives Prevalence of angina in women Prevalence of non-obstructive disease in women Anatomy vs. physiology for lesion assessment FFR iFR Microvascular disease measures in women
Better Diagnostic Methods Are Needed To Stratify Patients For Coronary Angiography The New England Journal of Medicine National Cath Lab Data Registry: 120 62% of patients undergoing elective cardiac catheterization do not have obstructive CAD 100 % of total patients 80 Majority of patients (84%) received noninvasive diagnostic testsprior to referral to catheterization 38% obstructive coronary artery disease 60 40 Low yield at invasive angiography is a diagnostic challenge 20 0 Pre-Coronary Angiography Post-Coronary Angiography N=397,954 N=149,739 Patel MR et al. N Engl J Med 2010;362:886-95.
Significant CAD by Sex and Ethnicity in Stable Angina Women have significantly less obstructive CAD independent of ethnicity Shaw et al. Circulation 2008 ;117:1787
In ACS Non-Obstructive CAD is more Common in Women Up to 20% of ACS patients referred for angiography have no significant CAD Of these ~60% are women and 40% are men Bugiardini et al. JAMA 2005;293:477-484 Daly et al. Circulation 2006;113:490-498 9
Learning Objectives Prevalence of angina in women Prevalence of non-obstructive disease in women Anatomy vs. physiology for lesion assessment FFR iFR Microvascular disease measures in women
Accuracy of Visual Assessment 20% overestimation of lesion severity by physician visual assessment compared to quantitative angiography PVA, Physician visual assessment; QCA, quantitative coronary angiography Zhang et al. JAMA Internal Medicine 2018.
Anatomy vs. Physiology Based Outcomes Johnson et al. Circ: Cardiovasc Imaging 2013.
Learning Objectives Prevalence of angina in women Prevalence of non-obstructive disease in women Anatomy vs. physiology for lesion assessment FFR iFR Microvascular disease measures in women
Women have higher FFR for given degree of stenosis than men (LAD) No sex difference in anatomic stenosis severity Women have higher FFR values at maximum hyperemia compared with male patients with the same degree of LAD stenosis Kang et al. JACC CI 2013.
FAME: Women have higher FFR values for the same degree of stenosis Kim et al. JACC CI 2012.
FFR-Guided PCI Equally Beneficial in Men and Women Kim et al. JACC CI 2012.
Learning Objectives Prevalence of angina in women Prevalence of non-obstructive disease in women Anatomy vs. physiology for lesion assessment FFR iFR Microvascular disease measures in women
DEFINE-FLAIR Sub-study FFR-guided strategy was associated with a higher rate of revascularization than iFR-guided strategy in men, but not in women. No sex differences in outcomes for FFR vs iFR guided interventions Kim et al. JACC CI 2019.
Learning Objectives Prevalence of angina in women Prevalence of non-obstructive disease in women Anatomy vs. physiology for lesion assessment FFR iFR Microvascular disease measures in women
IMR similar between men and women, CFR lower (but due to increased resting flow) Kobayashi et al. JACC CI 2015. Morrow et al. BMJ Case Report 2019.
Is Microvascular Dysfunction the Underlying Cause of Angina in Women without Obstructive CAD? Key Findings Kobayashi et al. JACC CI 2015. 1. Confirms that CFR is lower in women than men 2. BUT Microvascular function (IMR) is the same for men and women. 3. CFR is lower due to shorter resting transit time (OR higher coronary flow at rest) in women 157 patients (70% women), with angina and non-obstructive (<50%) CAD. Baseline intracoronary CFR, IMR, FFR. Coronary flow based on thermodilution (Mean transit time) Tmn=inverse correlate of absolute flow at rest and hyperemia IMR is a direct hyperemic measure; eliminates variability of resting vascular tone Resting transit time subject to substantial variation due to resting hemodynamics (BP, HR, contractility, coronary pathology)
Resting Transit Time and Coronary Flow: Predictors Short transit time=higher coronary flow Predictors of shorter transit time at rest Female sex (p=0.006) HTN (p=0.02) Smaller vessels (NS) Adverse prognosis of abnormal CFR likely multifactorial: Atherosclerosis: Early macrovascular disease Microvascular Dysfunction Non-Atherosclerosis: HTN, diastolic dysfunction, compounded by other risk factors common to women including insulin resistance, metabolic syndrome, diabetes