Comprehensive Guide to Polycystic Ovarian Syndrome in Adults and Adolescents
Managing polycystic ovarian syndrome (PCOS) requires a thorough understanding of its presentation, diagnosis, and management. This guide outlines the initial presentation in primary care, relevant examinations, diagnostic criteria, and management strategies for PCOS in both adults and adolescents. From screening to follow-up care, this resource covers essential considerations for healthcare professionals treating individuals with PCOS.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
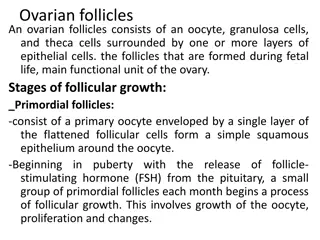
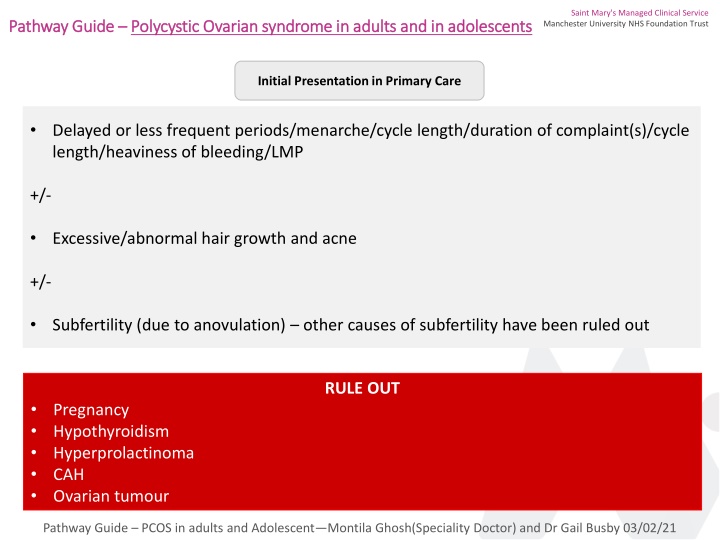
Saint Mary's Managed Clinical Service Manchester University NHS Foundation Trust Pathway Guide Pathway Guide Polycystic Ovarian syndrome in adults and in adolescents Polycystic Ovarian syndrome in adults and in adolescents Initial Presentation in Primary Care Delayed or less frequent periods/menarche/cycle length/duration of complaint(s)/cycle length/heaviness of bleeding/LMP +/- Excessive/abnormal hair growth and acne +/- Subfertility (due to anovulation) other causes of subfertility have been ruled out RULE OUT Pregnancy Hypothyroidism Hyperprolactinoma CAH Ovarian tumour Pathway Guide PCOS in adults and Adolescent Montila Ghosh(Speciality Doctor) and Dr Gail Busby 03/02/21
Saint Mary's Managed Clinical Service Manchester University NHS Foundation Trust Relevant examination for history related to anovulation and hyperandrogenism Please check BMI BP Acanthosis nigricans Hirsutism and acne Investigations FSH, LH, E2, androstenidione, DHEAS, TFT, PRL, 17-OH progesterone, Free androgen index (day 2 or 5 of spontaneous period Oral glucose tolerance test USS for PCOS (not adolescents) and exclude ovarian mass (testosterone producing tumour Diagnostic criteria for PCOS Two out of three :- 1) 2) Anovulation/ oligomenorrhea Clinical and/or biochemical evidence of hyperandrogenism hirsutism/acne/raised testosterone/ androstenedione/DHEAS and FAI Polycystic ovaries - >10cc and more than 12 follicles of 2-9mm 3) and o CAH/Hperprolactinemia/hypothyroidism/ovarian tumour have been excluded Pathway Guide PCOS in adults and Adolescent Montila Ghosh(Speciality Doctor) and Dr Gail Busby 03/02/21
Saint Mary's Managed Clinical Service Manchester University NHS Foundation Trust Management of Polycystic Ovarian Syndrome Management in Primary Care For Irregular Periods General Measures:- o If BMI (>25), to encourage 5-10% weight loss and referral to dietician for advice. This in itself can start to regularise period and also increase chance of spontaneous conception Screening an management of mental health condition is essential Counselling for long term consequence of PCOS like Metabolic syndrome, Type 2 diabetes, Cardiovascular complications, sleep apnoea, Endometrial hperplasia and cancer o o Wants contraception: Does NOT want contraception: Ensure at least 4 periods per year withdrawal bleed with 5 days NET 5mg tds or Provera 10mg BD after 12 weeks of amenorrhea after ruling out pregnancy Any CHC/Mirena/Implant/Depot as per UKMEC and patient choice Pathway Guide PCOS in adults and Adolescent Montila Ghosh(Speciality Doctor) and Dr Gail Busby 03/02/21
Saint Mary's Managed Clinical Service Manchester University NHS Foundation Trust Management of Polycystic Ovarian Syndrome Referral to Secondary Care: Management of irregular bleeding in confirmed PCOS with persistence of anovulation o Cyclical CHC 1st choice If CHC contraindicated or not tolerated Provera 10mg BD cyclically (3weeks on/1 week off) o Metformin Pathway Guide PCOS in adults and Adolescent Montila Ghosh(Speciality Doctor) and Dr Gail Busby 03/02/21
Saint Mary's Managed Clinical Service Manchester University NHS Foundation Trust Management of Polycystic Ovarian Syndrome Refer to secondary care: Refer to secondary care If subfertility (trying for pregnancy for 1 years) - Refer to Saint Mary s Reproductive Medicine unit Hyperandrogenic features a) Hirsuitism and acne and male pattern baldness May need treatment with ovulation induction agents/surgery i) ii) iii) CHC Metformin Spironolactone Refer to Endocrinology if new diagnosis of CAH increased 17-OH b) Only acne and no hyperandrogenism refer to dermatologist Or Hyperprolactinemia c) Unresponsive hirsutism ? Genetic i) ii) iii) iv) Eflornithin cream Electrolysis Laser therapy Reassurance and support Ovarian Mass 2WW referral Pathway Guide PCOS in adults and Adolescent Montila Ghosh(Speciality Doctor) and Dr Gail Busby 03/02/21
Saint Mary's Managed Clinical Service Manchester University NHS Foundation Trust National Guidance ESRE 2018 NICE 2018 RCOG Referral Proforma 2WW where appropriate Patient Information NHS website Pathway Guide PCOS in adults and Adolescent Montila Ghosh(Speciality Doctor) and Dr Gail Busby 03/02/21