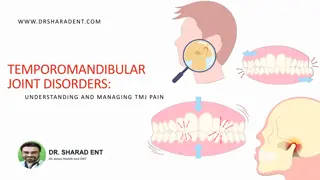
Comprehensive Approach to TMJ Pathology Diagnosis and Orthopedic Treatment

Understanding the prevalence, structure, and classification of TMJ dysfunction is vital in the diagnosis and orthopedic treatment of patients. Anamnesis, symptoms evaluation, and etiology of disc displacement play crucial roles in identifying the underlying issues. This comprehensive guide sheds light on the complexities of TMJ disorders, emphasizing the importance of proper evaluation and treatment strategies for optimal patient outcomes.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Diagnosis and orthopedic treatment of patients with TMJ pathology .
Prevalence of TMJ dysfunction: Articular disorders - 19% Muscle disorders - 23% A combination of muscle and joint disorders - 31% Have no signs of dysfunction - 31% The frequency of violations increases from 15 to 45 years. Ratio of men and women from 1/3 to 1/9.
The structure of the temporomandibular joint Ligaments of the temporomandibular joint View from the medial side. 1- lateral ligament (temporomandibular joint); 2- capsule of the temporomandibular joint; 3- wedge-mandibular ligament; 4 - awl-mandibular ligament; 5- aperture of lower jaw; 6- zygomatic arch; 7-wedge sinus; 8 - pituitary fossa (Turkish saddle).
DIAGNOSTICS OF TISSUE DISEASES Anamnesis 1. Symptoms at the moment: Pain, stiffness and tension in the muscles and joints; Impaired mobility of joints; Sensitivity or pain in the teeth, the intensity of pain reactions; The onset and duration of symptoms;
2. Previous Symptoms 3. Previous dental history. 4. Data on grinding or squeezing teeth
Classification. Articular problems: 1. Disc offset: With the restoration of position; Without restoring the situation. 2. Disk compression: The problem of the ligamentous apparatus of the joint; Muscular problems. 3. Combination of displacement and compression.
Etiology of disc displacement: Injury of the joint, leading to a sharp displacement of the joint head back;Loss of incisive path; Prosthetics without the principle of "freedom in centric" (when modeling a prosthesis, a dental technician should give 1 mm of freedom of the incisal and fang path); Anomalies of occlusion with forced position of the lower jaw (offset to the side).
2 types of displacement of the joint disc: With the restoration of position Without restoring the situation
The clinical picture of the displacement of the articular disc with the restoration of the position: Clicking when opening and closing the mouth at the same stage (reciprocal click may not be heard without a stethoscope); Shift of the lower jaw to the sore side, after clicking, the lower jaw is centered; Pain syndrome is not characteristic; Limitation of the volume of movements is not observed; Deformation of the disc in 31% of cases.
Without restoring the situation Acute stage: Severe pain with lower jaw movement Noticeable restriction of mouth opening There are no noises in the joint, but they can be in the anamnesis Straight line of deflection of the mandible to the sore side Limiting the movements of the lower jaw in a healthy way Chronic stage No noise, but they can be. Anamnesis Easy restriction of opening the mouth with a shift of the lower jaw to the sore side Limiting the movements of the lower jaw in a healthy way Deformation of the disc in 77% of cases
Treatment: Pain relief - diclofenac, ibuprofen (50 mg 2 r./d. After eating 5-10 days); Nimesulite, nise, nimelite (100 mg 2 r./d.After eating) Manufacturing of a reponning tire (when the disc is displaced with position restoration). Wear 10-15 days 24 hours a day (do not take off food for a while); Brush your teeth with your mouth open. Helps in 20-30% of cases. If for two weeks the kappa did not help (two reasons: clicking away from occlusion, shifting the disc without restoring the position), then plastics of the ligaments or removal of the disc are necessary.
Classification of TMJ diseases in children and adolescents (MMSI; NN Kasparov): 1.Primary-bone injuries and joint diseases. 1.1. Congenital pathology of the TMJ. 1.2. Inflammatory diseases of articular ends of bones and their outcomes. Osteoarthritis; Secondary deforming osteoarthritis; Bone ankylosis; neoarthritis. 2. Functional-distension diseases of the TMJ and their outcomes. 2.1. Youthful dysfunction of the TMJ Habitual dislocation; Painful dysfunction syndrome. 2.2. Inflammatory and inflammatory-degenerative primary cartilaginous diseases of the TMJ, developed as a consequence of joint dysfunction Arthritis (acute, chronic); Deforming juvenile arthrosis.
Dysfunction of the temporomandibular joint is a violation of joint mobility, in the form of restriction or increase in motion, lateral displacement, clicks in the joint, pain in the muscles and nerves of the face. If the dysfunction continues for a long time, the articular cartilage prematurely wears out, and in these cases we often see arthrosis or arthritis. Often this disorder is considered a trigeminal neuralgia, and treated for a long time and ineffectively. Osteoarthritis of the temporomandibular joint develops usually as a result of prolonged dysfunction, trauma or inflammation. The articular disc, cartilage becomes thinned and tearing, hence the pain and limitation of mobility in the joint. The diagnosis is not difficult to establish during examination and x- ray photographs. A full-scale treatment, as a rule, helps to relieve pain and improve mobility.
Inflammation of the temporomandibular joint (arthritis) occurs with arthrosis, after trauma and with such serious rheumatic diseases as rheumatoid arthritis, Bechterew's disease, gout, articular psoriasis, reactive arthritis, systemic lupus erythematosus. For proper treatment, it is necessary to find the cause of inflammation accurately, and we do this with the help of modern laboratory studies. Immobilization (contracture) of the temporomandibular joint after trauma or inflammation. Trism - a spasm of the muscles of the jaws, with difficulty opening the mouth. This is a consequence of pain in the area of the teeth or the temporomandibular joint, against the background of the depleted state of the nervous system.
Etiology of primary-bone inflammatory diseases of the TMJ Hematogenous osteomyelitis of the condylar process of the lower jaw; Birth trauma of the TMJ; Intra- and extra-articular fractures of the condylar process of the lower jaw; Acute traumatic arthritis of the TMJ; Odontogenic osteomyelitis of the lower jaw with transition to condylar process; Acute purulent otitis media; Osteomyelitis of the temporal bone (otogenous), mastoiditis.
Articular Symptoms 1. Crunch, clicks, pain while moving the jaw; 2. With a slow wide opening of the mouth, the jaw performs C- or S-shaped movements; 3. Failure to open your mouth smoothly; 4. Swelling and pain in the joint region (between the cheek and the auricle; 5. Insufficient or asymmetrical opening of the mouth; 6. Noise in the ear; 7. Increased wear of teeth.
Muscle Symptoms 1.Pain points in the muscles of the face (they are often taken for pain of the trigeminal nerve); 2. Fatigue when chewing; 3. Chewing on one side with a full set of teeth; 4. Pain when chewing; 5. Insufficient or asymmetrical opening of the mouth; 6. Increased wear of teeth.
What can be expressed dysfunction of the TMJ? Inside the joints there are no nerve endings, so if their work is disturbed, the pain rarely appears in the joint region, they irradiate to other areas. In addition to pain, the development of dysfunction of the TMJ is a strain in the muscles of the head and neck, the appearance of seals, the so-called "trigger points", painful when pressed. These muscles include: Chewing muscles Temporalis muscle Hyoid muscle Neck muscles Pterygoid muscle Sternum-subclavian-mastoid muscle Trapezius muscle of back
Possible causes of arthritis 1. Aggression of one's own immunity with respect to joint tissues. This is possible with autoimmune rheumatic diseases such as Reactive arthritis, Rheumatoid arthritis, Bechterew's disease (ankylosing spondylitis), Psoriatic arthritis (articular psoriasis), Systemic lupus erythematosus (SLE), Rheumatism.
2. Exchange violations. Of the inflammatory diseases of the joints most often gout, when the body produces an excess of uric acid and its crystals are deposited in the joints. Overload of the joint with its prolonged mechanical damage, microfractures of the meniscus, cartilage and ligaments. The reasons for a long load (walking, running, sports) with flat feet, arthrosis. Infectious inflammation. Often inflammation in the joint is associated with venereal infections, for example, chlamydia, gonorrhea. ureaplasma, mycoplasma,
Inflammation of the joints can be acute, then the joint swells, it can become hot to the touch, possibly redness of the skin around the joint. A pain arises necessarily. Body temperature may increase. Chronic, flaccid inflammation of the joints may not be accompanied by swelling, it is rare to see redness of the skin. An important symptom of inflammation is the combination of pain and stiffness, especially after a long stay of the joint in immobility, for example, in the morning, after a night's sleep, or after a long sitting.
Often associated with venereal, urological and gynecological infections, for example, chlamydia, ureaplasma, gonorrhea. inflammation in the joint is mycoplasma,
Osteoarthritis - inflammation of the joint, which developed as a result of damage or inflammation of the articular ends of bones and the spread of the inflammatory focus to the elements of the joint.
Displacement of the joints The displacement articular heads distally may also occur with the maximum closure of the teeth. of the or upwards interlacey
Clicks in the joints The clicking sounds at the opening and closing movements of the lower jaw, as well as with its lateral movements, symptoms of the mandibular dysfunction. are characteristic
Pathological changes in the joint (change in shape and degeneration) Osteoarthritis of the joint Leads to flattening, erasure and erosion of the joint, perforation of the disc, as well as to wear and erosion of the articular surfaces of the temporal bone. Prolonged existence of occlusal disharmony, displacement of joints and non- functional loads can lead to injury of joint tissues, changes in their shape or development of arthrosis.
The crepitation Crepitation sometimes appears in the joint with the opening, closing and eccentric movements of the lower jaw. These sounds testify to intra- articular pathology. is a "crunchy" sound that
Dislocation (subluxation) of joints Dislocation or subluxation may occur if the opening of the lower jaw is too strong, for example during yawning.
Chronic arthritis on the background of habitual dislocation: Clinical symptoms: Dull pain in the joint area, Asymptom of a crunch, Dysfunction of chewing muscles (pain, stiffness), Painful dysfunction syndrome. Diagnostic X-ray signs: Increasing narrowing of the joint space, Thinning and destruction of the subchondral bone closure plate, Foci of destruction in the subchondral bone of the head.
Primary-bone injuries and diseases of the TMJ. The congenital pathology of the TMJ is one of the symptoms of congenital syndromes (Robin syndrome, Franceschetti syndrome, Gill arches syndrome 1 and 2, Goldenhar syndrome), accompanied by a violation of the growth of the lower jaw. There is underdevelopment of the head n / h, condylar process, mandibular fossa of the temporal bone, articular tubercle. Clinical symptoms: Is revealed at the birth of a child, Underdevelopment of longitudinal dimensions of lower jaw on the side of developmental defect Movements are free, Concomitant malformations of the mouth slit, ear, neck. Diagnostic X-ray signs: Awide articular cleft up to the complete absence of articulation of the surfaces, Hypoplasia of the condylar process, articular tubercle and fossa of the temporal bone.
Ankylosis of the TMJ. There are two forms of ankylosis of the TMJ: bone and fibrous. However, it can be two stages of the same pathological process. Very often secondary deforming osteoarthritis precedes bone ankylosis. The clinical picture of bone ankylosis of the TMJ resembles the clinic of secondary deforming osteoarthritis. However, with bone ankylosis, the lower jaw is immovable and the patient can not open his mouth at all. Radiologically, the TMJ elements are virtually absent, as the bony growths occupy the entire articular gap (it is not visible), the articular cavity, sometimes even the semilunar incision, etc. There is complete or partial fusion of the condylar process of the lower jaw with the temporal bone. The most common cause of bone ankylosis is hematogenous osteomyelitis of the lower jaw, which occurs most often in young children.
Changing the shape of the head of the lower jaw with arthrosis of the TMJ Moving the incisal point when opening the mouth in patients with arthrosis
Neoarthrosis is a pathological articulation that arises from the displacement of the head of the n / h into a new position e under the influence of some pathological process; Leads to a slower growth of lower jaw . Clinical symptoms: The disease is detected at the age of 5-15 years, Underdevelopment of longitudinal dimensions of lower jaw on the side of the patient joint is absent or weakly expressed, Free or slightly limited movements of the jaw. Diagnostic X-ray signs: Unevenly deformed joint joint, The condylar process is shortened, The head is n / h flat, the bone is sclerotized.
Neoarthrosis or a false joint is a pathological joint in the immediate vicinity of the TMJ or instead of it, due to the displacement of the condylar process of the lower jaw or the lysis of its head. This is the most favorable outcome of osteoarthritis. Clinically, neoarthritis is characterized by asymmetry of the face, due to underdevelopment of the lower jaw on the "sick" side, malocclusion (oblique or cross), limited (but often normal) opening of the mouth. X-ray in this case there are all signs of neoarthrosis (closure of the cortical plate of the bone, etc.). Often the head of the condylar process is absent due to its lysis.
One of the outcomes of osteoarthritis in children is a secondary deforming osteoarthritis of the TMJ. This is a chronic joint disease, characterized by a combination of inflammatory, destructive and hyperplastic processes occurring at the articular ends of bones, cartilaginous tissue, ligamentous apparatus, etc. The disease develops again mainly in young children. Since the condylar process of the lower jaw is a zone of longitudinal growth of the lower jaw, as a result of this disease the longitudinal growth of the lower jaw from the "sick" side slows down or completely stops. At the same time, excessive bone formation occurs in the neck of the condylar overgrowth, due to chronic irritation of the periosteum. Locally, in addition to delaying the growth of the lower jaw and shifting the chin to the sore side, there is limited opening of the mouth, oblique (cross) bite, etc.X- ray joint joint is viewed as a straight line. The head of the condylar process is flat, the cervix is short, thick, sclerotized, the articular tubercle and fovea are weakly expressed. With the duration of the disease for several years, the shortening of the mandibular branch, the reflected deformation of the maxilla, and the like are determined.
Youthful dysfunction of the TMJ Etiology: -Parified infectious diseases; -Destruction of bite; -Orthodontic hardware treatment associated with n / h movement or overbiting. Clinical symptoms: - When you open your mouth - a click symptom; - Deviation of the jaw towards the joint with a smaller amplitude of movements; - Palpation - when the mouth is open, exit the head from the fossa with the formation of a westernization in front of the tragus of the ear. - Asyndrome of painful dysfunction is possible; - As a result of asynchronous "work" of both TMJ, S-shaped movements of the lower jaw are possible with maximum opening of the mouth (deviation of the lower jaw). Diagnostic X-ray signs: -Radiologically, with adolescent dysfunction of the TMJ, as a rule, pathological changes are not detected. When the mouth is open, exit the head from the fossa beyond the articular tubercle.
Treatment of arthritis: Restriction of opening the mouth, Anti-inflammatory and medicament Treatment of arthritis: treatment, Physiotherapy treatment, with contraindications phytotherapy (compresses from the ointment "Bagulnik" or "Rus", having a strong anti- inflammatory effect, medetherapy). to physiotherapy - as well as metal-
Treatment of bone ankylosis begins with surgical intervention (regardless of the age of the child), whose goal is to create a false joint as close as possible to the natural joint. To do this, use an osteotomy of the lower jaw with elastic stretching or osseous plastic of the lower jaw (arthroplasty). Later, mechanotherapy and orthodontic treatment are performed until 15-16 years, after which the question of the need for surgery for aesthetic or functional indications (contour or bone plastic) is decided. after immobilization,
Treatment of adolescent dysfunction should begin with activities that create rest in the joint. To do this, you can not take solid food, open your mouth wide, you should avoid traumatizing the lower jaw (sport), you can use a sling dressing, etc. In some cases, for the same purpose, you should use orthodontic devices that limit the opening of the mouth, especially with the habitual dislocation (Yadrovoy , The apparatus of Petrosov). In the presence of pain syndrome, it is possible to immobilize the lower jaw for 10-14 days with the help of ligature binding of teeth. At the same time, physiotherapy is carried out: UHF therapy, paraffin therapy, Novocain electrophoresis, potassium iodide; Phonophoresis of hydrocortisone, etc. Taking into account the pathogenesis of the disease, timely treatment can promote recovery by the time the organism grows to an end.
Treatment of arthrosis-arthritis of the TMJ similar, like juvenile the mandatory is addition, treatment is the use of non-hormonal anti- inflammatory drugs (salicylates). In adults, hormone therapy is treatment aimed at the prevention of habitual dislocation is not used in children. dysfunction. component In of possible. Surgical
Secondary inflammatory osteoarthritis and causes bone deformation of the articular ends of the bones: the condylar process and the articular surface of the temporal bone. Clinical symptoms: The underdevelopment of all lower jaw departments on the side of the affected joint, Limited mobility of the jaw. Diagnostic X-ray signs: Unevenly narrowed and deformed articular fissure, The condylar process is shortened, thickened, Compaction of the articular tubercle and fossa of the temporal bone. deforming bone osteoarthritis disease is a chronic after that develops
Evolution of secondary deforming osteoarthrosis of the TMJ: A-after birth trauma, - after the fracture of the condylar process, -after hematogenous osteomyelitis.
Kind of condylar process with secondary deforming osteoarthrosis:
Bony ankylosis is a pathological bone fusion of the condylar process with a temporal bone, which developed as a result of the death of the articular cartilage and the growth of bone tissue. Clinical symptoms: The disease is detected more often at the age of 2-3 years, The underdevelopment of all lower jaw departments on the side of the affected joint,Full immobility of the jaw. Diagnostic X-ray signs: The joint gap is absent, The bone of the condylar process without borders passes into the bone of the temporal bone.
Contracture is the restriction of mobility in the joint Common reasons: Joint destruction due to inflammation or trauma; Deformation of articular ends of bones (arthrosis, arthritis, trauma); Loss of elasticity of the joint capsule and ligaments (arthrosis, arthritis, periarthritis, trauma); Shortening of the muscles providing movement in the joint (paralysis, neuromuscular disease, trauma, surgery, post-burn scars, etc.). With contracture, the volume of possible movement in the joint is limited, up to its complete immobility (ankylosis). With complete ankylosis, only surgical treatment is possible, so we begin the development of contracture as early as possible. Surgical and non-surgical methods of treating contractures have been developed. We will offer you a course of non-surgical restorative treatment: Electrophoresis of caripazim (caripain); Degradative local treatment (compresses and ointments); Joint development and gymnastics; Special types of massage and self-massage. Electrophoresis of caripazim (caripain)
Treatment of secondary deforming osteoarthritis and ankylosis of the TMJ: Tasks: 1. Restoration of movement lower jaw surgically with fixation of the jaw of the jaw along the middle line of the face; 2. Orthodontic correction of deformities of the alveolar process of the upper and alveolar part of the lower jaw and correction of the occlusion; 3. Prevention of the development of secondary deformities of the upper jaw; 4. Physical development of masticatory and mimic muscles by myogymnia.
Orthopedic treatment: of occlusal Normalization polishing);Normalization of the form of dental rows (artificial crowns, bridges, clasp prostheses); Restoration of interalveolar height; Normalization of the position of the joints in the articular pits(Plastic kappa on the dentition, stamping plate on the entire dentition or on the lateral teeth, palatal plate with an inclined plane, mouth opening limiters); X-ray control; Prosthetics are carried out in 2-3 months from the beginning of using the device to restore the interalveolar height. contacts (selective














")













 of")