Statewide Pulmonary Rehabilitation Project Overview
 undefined
undefined
Q
L
D
P
R
N
e
t
w
o
r
k
D
a
t
a
C
o
l
l
e
c
t
i
o
n
Lung Foundation: Pulmonary Rehab Network Presentation
1 August 2023
James Walsh
Nadia Nestor


Respiratory (& Sleep) Clinical Network
•
Clinical Network steering committee meets every 6 weeks and
had a yearly one day forum
•
Clinical network has a number of workgroups: respiratory function
testing, smoking cessation, etc
•
Pulmonary rehabilitation (PR) workgroup
–
Pre-COVID era: Workgroup met x1/year and informal network
•
Clinical practice improvement payment was used previously
(2013-15) to establish a minimum data set and provided raw data
(excel output) of participating pulmonary rehab programs
Project presentation: Health Improvement Unit
Background
•
COPD & Asthma account for over 5% of the total burden of
disease in Qld
•
PR: considered standard care for people with chronic lung
diseases
–
Strong evidence base
–
COVID-19 response
:
Sudden cessation/ rapid change in models of care
•
Reduced capacity, delayed access, increase demand, staff re-deployment, increased
wait lists, etc
•
Still needed to provide PR
•
Raised with Steering Committee, Qld Respiratory Clinical Network and then
prioritised to progress within Clinical Excellence Queensland
3
Project presentation: Health Improvement Unit
•
O
p
p
o
r
t
u
n
i
t
i
e
s
–
Maintenance of service provision in COVID-19 future
–
Opportunity to embed virtual rehabilitation model into usual care
–
Equity: Improved access for those unable to attend centre-based care
–
Enhance choices for patients in the long term
•
Offer choice of modality not previously available
•
C
h
a
l
l
e
n
g
e
s
–
Balancing delivery of efficient and sustainable combination of care models
–
Virtual programs are resource intensive
•
Continued learnings of virtual model
–
Limited ability to evaluate implementation and outcomes
•
Lack of planned data collection and readily available data
–
Lack of coordinated support
–
Potential future increase in referrals for post COVID survivors
Statewide PR Project
Funded by Clinical Excellence Queensland, the Statewide Pulmonary
Rehabilitation Project commenced in October 2020 – June 2022.
P
r
o
j
e
c
t
s
A
i
m
:
To develop, implement and evaluate strategies to increase the capacity within
Queensland PR programs to support the equitable access for chronic respiratory
Patients.
P
r
o
j
e
c
t
O
b
j
e
c
t
i
v
e
s
:
1.Telerehabilitation Framework & trial different Telerehabilitation Models of Care
An evidence – based framework that supported and streamlined service provision
and inform the ongoing delivery of quality virtual models of PR.
2. Co-ordinate approach towards updated Data reporting and systems
Digital integration of Measuring Analysis and Reporting System (MARS) data
collection with Power BI benchmarking platform and QHERS automated reporting
system
3. Advocate and Support
Active engagement with PR service providers and programs within the statewide
PR working group network
5
Phase 1 (Oct 2020 to Jun 2021) Project Outcomes
•
Developed Virtual rehab framework
•
Started the update of state wide PR data collection
•
Supported Qld PR providers
–
Monthly meetings, scaffolded start up of tele programs, PD events
•
Identified opportunities to increase PR access
•
Trialled telerehab in 4 existing (unfunded) PR sites
–
Pre Lung Transplant PR (4 patients) work up for listing:
R
e
d
u
c
e
d
t
r
a
v
e
l
t
i
m
e
o
f
8
,
7
0
4
k
m
a
n
d
1
1
4
h
o
u
r
s
,
a
n
d
t
r
a
v
e
l
-
r
e
l
a
t
e
d
c
o
s
t
s
a
v
i
n
g
o
f
o
v
e
r
$
6
,
2
6
6
f
o
r
t
h
e
i
n
i
t
i
a
l
4
t
r
i
a
l
s
i
t
e
p
a
r
t
i
c
i
p
a
n
t
s
6
Phase 2 (Jul 2021 to Jun 2022) Project Outcomes
•
Developed Clinical Implementation guide
•
Funded 4 regional/rural tele PR programs
•
14/19 Qld PR programs transitioned to virtual PR
–
Rapid implementation Jan 2022
•
Update of state wide PR data collection (MARS)
–
To assess different models of care and real time benchmarking
•
Developed & endorsed Quality Indicators
–
Data dictionary to interpret MARS, dashboard and quality indicators
•
Automated patient completion letter
•
Real Time Power Bi Dashboard
7
V
i
r
t
u
a
l
P
u
l
m
o
n
a
r
y
R
e
h
a
b
i
l
i
t
a
t
i
o
n
F
r
a
m
e
w
o
r
k
Developed a virtual PR framework
Completed 10 virtual trials
Demonstrated virtual models of PR
are effective and safe
Reported
adverse
events
S
t
a
t
e
w
i
d
e
P
u
l
m
o
n
a
r
y
R
e
h
a
b
i
l
i
t
a
t
i
o
n
P
r
o
j
e
c
t
2
0
2
0
-
2
0
2
2
Updated MARS data platform
Access to benchmarking dashboard
Automated patient completion reporting
Development of state-wide quality
indicators (program and clinical)
Statewide PR Data dictionary
D
i
g
i
t
a
l
l
y
I
n
t
e
g
r
a
t
e
d
D
a
t
a
B
e
n
c
h
m
a
r
k
i
n
g
P
u
l
m
o
n
a
r
y
R
e
h
a
b
i
l
i
t
a
t
i
o
n
P
r
o
v
i
d
e
r
s
I
n
c
r
e
a
s
e
d
A
c
c
e
s
s
t
o
c
a
r
e
1
4
/
1
9
PR programs
transitioned
virtual into
Business as
Usual
Patient Feedback
20% new
programs
offered
Decreased
time to access
service*
0
13/15
HHS have PR
498
virtual patients
^
1
0
n
e
w
v
i
r
t
u
a
l
P
R
p
r
o
g
r
a
m
s
3
v
i
r
t
u
a
l
o
n
l
y
P
R
s
e
r
v
i
c
e
s
*As of MARS Power Bi 27/6/22
3
0
/
3
2
PR locations in
Queensland are
participating
^FY 21/22 facility reported data
Real time
statewide
benchmark
reporting
Staff Feedback
Flexible, patient centred options
Delivery of care closer to home
Pandemic proof
Increased equity for rural and remote
chronic respiratory patients
P
r
o
j
e
c
t
A
i
m
s
Regular community of practice meetings
Education and shared learnings
Clinician support pathways
Advocacy, support with high engagement
1
9
H
H
S
P
r
o
g
r
a
m
s
3
2
l
o
c
a
t
i
o
n
s
7
0
c
l
i
n
i
c
i
a
n
s
“
virtual allows us to reach those consumers
the often miss out on these programs due to
geography, transport limitations, fear of gyms
and groups, costs, hospital parking”
“I enjoyed seeing patients have the
opportunity to participate in a program that
was so beneficial for them and seeing them
improve in their function. “
“ we have a good understanding of virtual
model now and look forward to being able to
using in a multi-model approach to PR”
“Telehealth was wonderful. I was able to save
financially and on travel time. I was able to
work around other commitments I had
without the worry of travel time.”
“
I
h
a
v
e
r
e
c
o
m
m
e
n
d
e
d
a
f
r
i
e
n
d
t
h
a
t
h
a
s
h
e
a
v
y
b
r
e
a
t
h
i
n
g
t
o
s
e
e
i
f
h
e
c
a
n
g
e
t
r
e
f
e
r
r
e
d
t
o
t
h
e
r
e
s
p
i
r
a
t
o
r
y
c
l
i
n
i
c
s
o
t
h
a
t
h
e
c
a
n
s
o
m
e
t
o
P
R
”
“
Banter on the side was good and everyone
was really happy with the care provide”
“
H
i
c
k
u
p
s
a
l
o
n
g
t
h
e
w
a
y
w
i
t
h
t
e
c
h
n
o
l
o
g
y
b
u
t
v
i
r
t
u
a
l
I
f
e
l
t
h
a
s
l
e
s
s
i
n
t
e
r
r
u
p
t
i
o
n
s
t
h
a
n
f
a
c
e
t
o
f
a
c
e
”
Care closer to home
Flexible and tailored options
Reduced travel time and costs
Improved Exercise capacity
Improved Quality of Life
S
e
r
v
i
c
e
B
e
n
e
f
i
t
s
Standardised outcome reporting
Service planning
Models of care impact &
outcomes
Future capacity for healthcare
utilisation analysis
P
a
t
i
e
n
t
B
e
n
e
f
i
t
s
P
r
o
j
e
c
t
A
c
h
i
e
v
e
m
e
n
t
s
Endorsed Quality Indicators
M
e
a
s
u
r
i
n
g
A
n
a
l
y
s
i
s
a
n
d
R
e
p
o
r
t
i
n
g
S
y
s
t
e
m
(
M
A
R
S
)
August 2021 & May 2022
Upgrade completed and available
-
Goal: Improve data accuracy and
provider efficiency with entry
-
Average Time to complete <8 mins
Indicated data required for both
-
Patient Completion Letter
-
PRP Benchmarking Dashboard
C
a
n
b
e
c
o
m
m
e
n
c
e
d
,
s
a
v
e
d
a
n
d
c
o
m
p
l
e
t
e
d
a
t
m
u
l
t
i
p
l
e
p
o
i
n
t
s
i
n
p
a
t
i
e
n
t
’
s
P
R
P
j
o
u
r
n
e
y
b
y
m
u
l
t
i
p
l
e
t
e
a
m
m
e
m
b
e
r
s
.
A
u
t
o
m
a
t
e
d
P
a
t
i
e
n
t
P
R
P
C
o
m
p
l
e
t
i
o
n
L
e
t
t
e
r
-
Q
H
E
R
S
•
Available within 24 hours of data submission
•
Scheduled or print on demand options
•
Default option for printing is PDF
•
Export in Microsoft Word (editable)
•
Access can be granted to all QH staff
•
Completed from MARS Data Elements
20
Phase 3 (Jul 2022 onwards) Project
•
Data supported for further funding opportunities to address
equity of access within regional and remote programs
•
Upgrades to the Quality Indicators and MARS are still required
•
Additional QUERS reporting letter suite
•
Referral management links
•
Hospital utilisation data impacts
•
Improving quality of Data input
•
State wide PR Program Advisor
21
The Statewide Pulmonary Rehabilitation Project, funded by Clinical Excellence Queensland, aims to enhance care models for chronic lung diseases like COPD and asthma. The project explores virtual rehabilitation integration, ensuring equity and improved access for patients. Challenges include resource intensiveness and data collection gaps. Started in 2020, the project seeks to provide sustainable, efficient care post-COVID.
- Pulmonary Rehabilitation
- Chronic Lung Diseases
- Virtual Rehabilitation
- Healthcare Improvement
- Clinical Excellence

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
QLD PR Network Data Collection Lung Foundation: Pulmonary Rehab Network Presentation 1 August 2023 James Walsh Nadia Nestor
Respiratory (& Sleep) Clinical Network Clinical Network steering committee meets every 6 weeks and had a yearly one day forum Clinical network has a number of workgroups: respiratory function testing, smoking cessation, etc Pulmonary rehabilitation (PR) workgroup Pre-COVID era: Workgroup met x1/year and informal network Clinical practice improvement payment was used previously (2013-15) to establish a minimum data set and provided raw data (excel output) of participating pulmonary rehab programs
Project presentation: Health Improvement Unit Background COPD & Asthma account for over 5% of the total burden of disease in Qld PR: considered standard care for people with chronic lung diseases Strong evidence base COVID-19 response: Sudden cessation/ rapid change in models of care Reduced capacity, delayed access, increase demand, staff re-deployment, increased wait lists, etc Still needed to provide PR Raised with Steering Committee, Qld Respiratory Clinical Network and then prioritised to progress within Clinical Excellence Queensland 3
Project presentation: Health Improvement Unit Opportunities Maintenance of service provision in COVID-19 future Opportunity to embed virtual rehabilitation model into usual care Equity: Improved access for those unable to attend centre-based care Enhance choices for patients in the long term Offer choice of modality not previously available Challenges Balancing delivery of efficient and sustainable combination of care models Virtual programs are resource intensive Continued learnings of virtual model Limited ability to evaluate implementation and outcomes Lack of planned data collection and readily available data Lack of coordinated support Potential future increase in referrals for post COVID survivors
Statewide PR Project Funded by Clinical Excellence Queensland, the Statewide Pulmonary Rehabilitation Project commenced in October 2020 June 2022. Projects Aim: To develop, implement and evaluate strategies to increase the capacity within Queensland PR programs to support the equitable access for chronic respiratory Patients. Project Objectives: 1.Telerehabilitation Framework & trial different Telerehabilitation Models of Care An evidence based framework that supported and streamlined service provision and inform the ongoing delivery of quality virtual models of PR. 2. Co-ordinate approach towards updated Data reporting and systems Digital integration of Measuring Analysis and Reporting System (MARS) data collection with Power BI benchmarking platform and QHERS automated reporting system 3. Advocate and Support Active engagement with PR service providers and programs within the statewide PR working group network 5
Phase 1 (Oct 2020 to Jun 2021) Project Outcomes Developed Virtual rehab framework Started the update of state wide PR data collection Supported Qld PR providers Monthly meetings, scaffolded start up of tele programs, PD events Identified opportunities to increase PR access Trialled telerehab in 4 existing (unfunded) PR sites Pre Lung Transplant PR (4 patients) work up for listing: Reduced travel time of 8,704km and 114 hours, and travel-related cost saving of over $6,266 for the initial 4 trial site participants 6
Phase 2 (Jul 2021 to Jun 2022) Project Outcomes Developed Clinical Implementation guide Funded 4 regional/rural tele PR programs 14/19 Qld PR programs transitioned to virtual PR Rapid implementation Jan 2022 Update of state wide PR data collection (MARS) To assess different models of care and real time benchmarking Developed & endorsed Quality Indicators Data dictionary to interpret MARS, dashboard and quality indicators Automated patient completion letter Real Time Power Bi Dashboard 7
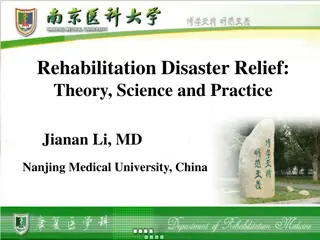
Statewide Pulmonary Rehabilitation Project 2020-2022 Project Aims Project Achievements 0 Virtual Pulmonary Rehabilitation Framework 14 /19 Developed a virtual PR framework Completed 10 virtual trials Demonstrated virtual models of PR are effective and safe Reported adverse events PR programs transitioned virtual into Business as Usual Updated MARS data platform Access to benchmarking dashboard Automated patient completion reporting Development of state-wide quality indicators (program and clinical) Statewide PR Data dictionary Real time statewide benchmark reporting Digitally Integrated Data Benchmarking 30/32 PR locations in Queensland are participating 13/15 HHS have PR Decreased time to access service* Flexible, patient centred options Delivery of care closer to home Pandemic proof Increased equity for rural and remote chronic respiratory patients 20% new programs offered Increased Accessto care 498 virtual patients^ *As of MARS Power Bi 27/6/22 10 new virtual PR programs Regular community of practice meetings Education and shared learnings Clinician support pathways Advocacy, support with high engagement Pulmonary Rehabilitation Providers 19 HHS Programs 32 locations 70 clinicians 3 virtual only PR services Staff Feedback Patient Benefits Patient Feedback Telehealth was wonderful. I was able to save financially and on travel time. I was able to work around other commitments I had without the worry of travel time. ^FY 21/22 facility reported data Care closer to home Flexible and tailored options Reduced travel time and costs Improved Exercise capacity Improved Quality of Life virtual allows us to reach those consumers the often miss out on these programs due to geography, transport limitations, fear of gyms and groups, costs, hospital parking I have recommended a friend that has heavy breathing to see if he can get referred to the respiratory clinic so that he can some to PR I enjoyed seeing patients have the opportunity to participate in a program that was so beneficial for them and seeing them improve in their function. Service Benefits Standardised outcome reporting Service planning Models of care impact & outcomes Future capacity for healthcare utilisation analysis Banter on the side was good and everyone was really happy with the care provide Hick ups along the way with technology but virtual I felt has less interruptions than face to face we have a good understanding of virtual model now and look forward to being able to using in a multi-model approach to PR
Endorsed Quality Indicators P2. Comprehensive Assessment & Completion. For an enrolled patient to be considered to have completed their program a participant should have completed a comprehensive assessment at pre- and post-program and having attended 75% of all available supervised exercise sessions for that program and model of care offered. P3: Program Components. Delivery of a comprehensive pulmonary rehabilitation programs will have both an individually tailored exercise component (regardless of delivery mode or frequency) and provided an appropriate education component for its participants. P1. Referral to Pulmonary Rehabilitation Service. That pulmonary rehabilitation referrals, regardless of respiratory condition and post exacerbation status, to the service have commenced within 90 days from receipt of initial referral for 80% of all referrals to the program. Program/ Service Delivery C2: Health-Related Quality of Life Assessment . Assessment of patient completed Health-Related Quality of Life is completed by services utilising the St. George Respiratory Questionnaire (SGRQ) and/or COPD Assessment Tool (CAT) and that the MID of either test will indicate impact of intervention. C1: Exercise Capacity Assessment. Assessment of exercise capacity: there is strong evidence for field walking testing (6MWT) at pre and post assessment over other tests such as a functional strength endurance testing (STS). C3: Dyspnoea Assessment. Assessment of dyspnoea via the modified Medical Research Council (mMRC) is completed to ensure that a measure of dyspnoea on impact activity limitation is assessed for the patient. Clinical Outcome Indicators Optional Indicator C4: Assessment of Nutritional Status. This can only be assessed with Body Mass Index (BMI) currently within MARS system currently but there is a recommendation to add Malnutrition Screen Tool (MST) to MARS
Measuring Analysis and Reporting System (MARS) August 2021 & May 2022 Upgrade completed and available - Goal: Improve data accuracy and provider efficiency with entry Average Time to complete <8 mins - Indicated data required for both - Patient Completion Letter - PRP Benchmarking Dashboard Can be commenced, saved and completed at multiple points in patient s PRP journey by multiple team members.
Automated Patient PRP Completion Letter - QHERS Available within 24 hours of data submission Scheduled or print on demand options Default option for printing is PDF Export in Microsoft Word (editable) Access can be granted to all QH staff Completed from MARS Data Elements
Phase 3 (Jul 2022 onwards) Project Data supported for further funding opportunities to address equity of access within regional and remote programs Upgrades to the Quality Indicators and MARS are still required Additional QUERS reporting letter suite Referral management links Hospital utilisation data impacts Improving quality of Data input State wide PR Program Advisor 21

 Clinical Network")



 Project Outcomes")
 Project Outcomes")













 Project")