Motor Abilities in Williams Syndrome and Their Importance
Motor abilities play a crucial role in the developmental journey of individuals with Williams Syndrome. From simple reflex movements to fine and gross motor skills, these abilities impact daily living, academic achievements, and overall cognitive and physical growth. Research on motor skills in both children and adults with Williams Syndrome sheds light on milestones achieved and areas for improvement. Understanding the significance of motor skills can lead to interventions that enhance independence and quality of life for individuals with this syndrome.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
MOTOR ABILITIES IN WILLIAMS SYNDROME AND WHY THEY ARE IMPORTANT L E I G H A N N E M AYA L L P H D S T U D E N T S U P E RV I S O R S : P R O F E M I LY FA R R A N , P R O F A N DY TO L M I E U C L I N S T I T U T E O F E D U C AT I O N L E I G H A N N E . M AYA L L . 1 4 @ U C L . AC . U K
OVERVIEW Why are motor skills important for independent/daily living and academic achievement? What are motor abilities like in children with Williams Syndrome? My research: what are motor abilities like in adults with Williams Syndrome? Implications Suggestions of what could be done to improve motor abilities Questions
WHAT DO WE MEAN BY MOTOR ABILITIES? Automatic/reflex movements: movement that we don t think about Breathing, facial expression, body language Non-automatic/learnt movement: movement that we choose to do Fine motor ability: writing and drawing, handling small objects Gross motor ability: playing sports, walking, jumping, skipping Non-automatic movement can become more automatic over time with practice.
WHY ARE MOTOR SKILLS IMPORTANT? From birth, typically developing infants begin learning by interacting with their environment through motor acts, such as reactions to interesting stimuli by orientating the head (Berthental, 1996). These simple movements will, over time, evolve into more complex motor behaviours by helping infants to learn new motor skills, such as sitting unsupported, standing and eventually, walking (Burton, 1998). The learning of new motor abilities provides new learning opportunities. In this way, gross motor skills that are learnt in the first few months facilitate other motor and cognitive skills in later childhood in both typical development and in individuals at risk of developmental delay.
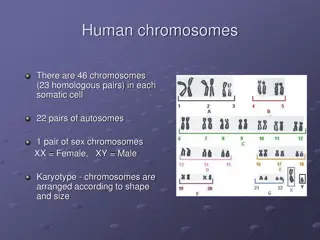
MOTOR MILESTONES IN WILLIAMS SYNDROME Carrasco, Castillo, Aravena, Rothhammer and Aboitiz (2005)
WHO WS group (N=20) Age in months at which Milestone achieved M (SD) Range N M (SD) P tile Range Sit without support Crawl hands and knees Stand with assistance Stand without support Walk with assistance Walk without support 6 (1.1) 3.8 - 9.2 9 12.222 (5.911) 15.500 (5.612) 16.286 (6.130) 24.600 (9.370) 21.167 (9.131) 24.615 (8.921) >99th 2-24 8.5 (1.7) 5.2 11.4 6 >99th 5-21 7.6 (1.4) 4.8 11.4 7 >99th 10-24 11.0 (1.9) 6.9 16.9 5 >99th 12-36 9.2 (1.5) 6 13.7 6 >99th 12-36 12.1 (1.8) 8.2 17.6 13 >99th 15-42
MOTOR ABILITY IN CHILDREN WITH WILLIAMS SYNDROME Fine motor ability (e.g. drawing shapes and manipulation of small objects) is impaired in children with WS (Tsai et al., 2008; Wuang et al., 2016). Inconsistent evidence for impaired gross motor ability (e.g. walking in a straight line, hopping, sit ups, etc.) in children with WS. Tsai et al. (2008) report impairment. Wuang et al. (2016) demonstrated that only 60% of their group (aged 6-12 years) showed impairment. It was also found that full scale IQ, was strongly correlated with fine motor ability, and moderately correlated with gross motor ability (Wuang et al, 2016).
WHY MIGHT MOTOR PERFORMANCE BE IMPAIRED IN WS? Brain differences (cerebellum and basal ganglia) Genetic (gene GTF2IRD1; Schneider et al, 2012) Negative past experiences (bullying, social pressure, self esteem) Motivation Anxiety (fear of failure, fear of getting hurt) Cascading effects of delayed motor milestones Limited motor strategies
MY RESEARCH 1) What is the full profile of fine and gross motor abilities for adults with WS? 2) Is motor competence associated with the extent to which individuals with WS partake in physical activity?
METHODS Participants: 20 individuals with WS aged 16-50 and 40 typically developing children aged 4-7 years. The age range for the typically developing children was chosen to match the range of motor ability in the WS group. Motor ability was assessed using the Bruininks-Oseretsky Test of Motor Proficiency, Second Edition short form (BOT2-SF; Bruininks & Bruininks, 2005). This measure was designed for ages 3 to 21 years. The BOT2-SF measures an individuals fine and gross motor ability using a series of motor tasks. Physical activity was measured using a questionnaire where participants were asked how many times on week-days and weekends they engaged in sports and exercise (excluding P.E.). This included things like: swimming, tennis, football, dance, yoga, gym, etc
RESULTS: OVERALL MOTOR ABILITY The WS group are performing at the 4-5 year old level (p>.05), and both the WS and 4-5 year old group are performing below the 6-7 year old level (p<.05 for both). The WS group are all performing in the below average or well below average zone of the BOT2-SF, whereas the TD groups are all performing in the average to well above average zones
RESULTS: PHYSICAL ACTIVITY Group The WS group took part in a similar amount of physical activity as the 4-5 year old children, and significantly less than the 6-7 year olds. Sports WS TD4-5 (N=20) TD6-7 (N=20) (N=20) 1.75 (1.48) 2.00 (1.26) 3.10 (2.10) WS (n=20) r=.349, p=.065 TD (n=40) r=.298, p=.031 Correlational analyses revealed significant correlations between fine and gross motor ability and physical activity for the TD group, but not the WS group. Gross Motor X physical activity r=.297, p=.102 r=.482, p=.001 Fine Motor X physical activity
CONCLUSIONS Relative strength: Upper limb control: familiar task Relative weakness: Balance: unfamiliar task. Cerebellar abnormalities. Familiarity of motor tasks is linked to available motor strategies. The hypothesis that individuals with better motor abilities would be involved in more sports was not supported in the WS group, as neither fine nor gross motor ability correlated with participation in sports in this group. This is probably related to less availability of sports and other physical activities in the area, which is likely to impact the WS group more than the TD participants.
IMPLICATIONS OF POOR MOTOR SKILLS The severity of motor problems suggests that motor ability in WS could be affecting other aspects of the individuals lives, e.g. independence Individuals with WS may also show difficulties with many everyday activities involving fine motor skills such as doing up buttons and shoe laces when getting dressed and using a pen or pencil. Stair assent and decent is another gross motor ability that is likely to be affected in WS. Adults with WS may have limited independence and might not have the same freedom to explore as typical adults. Low scores on motor tasks was often due to less confidence. This could also account for the low levels of participation in physical activity. The low levels of involvement in physical activity could also be effecting social skills.
SUGGESTIONS Academically: make sure that teachers are aware that fine motor skills are impaired, so things like handwriting and drawing will be more of a challenge. P.E. is also likely to be a difficulty for people with WS, both because gross motor skills are impaired, but also because of potential feelings of anxiety and embarrassment when with peers who may be more motorically able. Practicing unfamiliar routes, e.g. before starting a new job. Visit new places and know what kinds of route and what the building is like to get around it. Be aware that the motor difficulties are not straightforward, and if the individual is prone to anxiety then they might be less likely to want to engage. If they are likely to be doing something that they are anxious about due to motor skills then practice them with them before to improve confidence. People with WS need a safe and supportive place to practice motor skills. Need to be able to enjoy physical activity to practice motor skills. Encourage people with WS to engage in sports and exercise/walk a bit further/try new things.
SUMMARY Infants with WS show delays in reaching motor milestones, which is likely to impact later motor skill development and cognitive abilities. Children with WS score significantly lower on standardized motor assessments. Our research shows that these low motor scores persist into adulthood, and are associated with cognitive abilities. These poor motor skills are likely to impact cognitive development, social skills, confidence and independence.
ACKNOWLEDGEMENTS Prof Emily Farran Dr Hana D Souza Prof Andrew Tolmie Miss Fatima Esfandi All the families who participated!
THANK YOU FOR LISTENING QUESTIONS?