Understanding the Cholinergic System and Cholinergic Drugs
The cholinergic system plays a crucial role in the transmission of signals within the nervous system. Acetylcholine (ACh) is the primary neurotransmitter involved in cholinergic transmission, impacting various physiological functions. Cholinergic neurons synthesize ACh through a complex process involving acetyl-CoA and choline. The release of ACh into the synaptic cleft is regulated by intricate mechanisms, including vesicle fusion and calcium influx. Understanding cholinergic transmission is essential for comprehending the effects of cholinergic drugs and their implications in medical practice.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
CHOLINERGIC SYSTEM AND CHOLINERGIC DRUGS Dr. KHAN IMU..BISHKEK KYRGYZSTAN
Sympathetic VsParasympathetic SYMPATHETIC Fight orFlight Increase BP & HR, glucose,perfusion to skeletal muscles, Mydriasis,Bronchodilatation PARASYMPATHETIC Rest and Digest Miosis, decreased HR, BP , bronchiasecretion, Insulin release, Digestion,excretion
SitesofCholinergicTransmission-Summary Acetylcholine (ACh) is major neurohumoral transmitter atautonomic, somatic and central nervoussystem: 1. All preganglionic sites (Both Parasympatheticand sympathetic) 2. All PostganglionicParasympatheticsitesandsympathetictosweatglandandsome bloodvessels 3. SkeletalMuscles 4. CNS:Cortex,Basalganglia,spinalchordandothers ParasympatheticStimulation Acetylcholine(Ach)releaseatneuroeffectorjunction- biologicaleffects Sympathetic stimulation Noradrenaline (NA) at neuroeffector junction - biologicaleffects
Cholinergic Transmission Synthesis: Cholinergic neurons contain large numbers of small membrane-bound vesicles (containing ACh) concentrated near the synaptic portion of the cell membrane ACh is synthesized in the cytoplasm from acetyl-CoA and choline by the catalytic action of Choline acetyltransferase (ChAT) Acetyl-CoA is synthesized in mitochondria, which are present in large numbers in the nerve ending Choline is transported from the extracellular fluid into the neuron terminal by a Na+- dependent membrane choline cotransporter (Carrier A). This carrier can be blocked by a group of drugs called hemicholiniums T h e action of the choline transporter is the rate-limiting step in ACh synthesis
Cholinergic Transmission Release: Synthesized, ACh is transported from the cytoplasm into the vesicles by an antiporter that removes protons (carrier B). This transporter can be blocked by vesamicol Release is dependent on extracellular Ca2+ and occurs when an action potential reaches the terminal and triggers sufficient influx of Ca2+ions The increased Ca2+concentration "destabilizes" the storage vesicles by interacting with special proteins associated with the vesicular membrane (VAMPs and SNAP- synaptosome associated protein) Fusion of the vesicular membranes with the terminal membrane results in exocytotic expulsion of ACh into the synaptic cleft The ACh vesicle release process is blocked by botulinum toxin through the enzymatic removal of two amino acids from one or more of the fusion proteins. Black widow spider??
Cholinergic Transmission: Destruction After release - ACh molecules may bind to and activate an ACh receptor (cholinoceptor) Eventually (and usually very rapidly), all of the ACh released will diffuse within range of an acetylcholinesterase (AChE) molecule AChE very efficiently splits ACh into choline and acetate, neither of which has significant transmitter effect, and thereby terminates the action of the transmitter. Most cholinergic synapses are richly supplied with AChE; the half-life of ACh in the synapse is therefore very short. AChE is also found in other tissues, eg, red blood cells. Another cholinesterase with a lower specificity for ACh, butyrylcholinesterase [pseudo cholinesterase], is found in blood plasma, liver, glial, and many other tissues
True Vs PseudoAChE True AChE Pseudo AChE All cholinergic sites, RBCs, gray matter Plasma, liver, Intestine and white matter Distribution Action on: Acetycholine Methacholine Function Very Fast Slower Slow Not hydrolyzed Hydrolysis of Ingested Esters More sensitive to Organophosphates Termination of Ach actio Inhibition More sensitive to Physostigmine
Cholinergicreceptors-2types Muscarinic (M) and Nicotinic(N): Nicotinic (N) ligand gated Muscarinic (M) - GPCR
Muscarinic Receptors?? 1. Selectively stimulated by Muscarine and blocked by Atropine all areG- protein coupledreceptors 2. Primarily locatedinautonomiceffector cellsin heart,eye,smoothmuscles andglandsofGITandCNS 3. SubsidiaryMreceptorsarealsopresentingangliafor modulation long lasting lateEPSP 4. Autoreceptors(Mtype) arepresentinpostganglionic prejunctional cholinergicNerveendings inhibitsAChrelease 1.alsoin adrenergicnerveterminals(inhibitsNArelease)leading to vasodilatation when ACh isinjected 5. Bloodvessels:Allbloodvesselshavemuscarnincreceptorsalthoughno cholinergicinnervations EDRF SMrelaxation-Vasodilatation
Muscarinic Receptors -Subtypes Pharmacologically- M1, M2, M3, M4andM5 M4andM5arepresentincertainareasof Brainandregulateother neurotransmitters M1,M3andM5fallinoneclass,whileM2andM4inanotherclass However- M1,M2andM3aremajoronesandpresentineffector cellsand prejunctionalnerveendingsinPeripheralorgansandCNS Allsubtypeshavelittle agonistselectivitybut selectiveantagonistselectivity Mostorgansusuallyhavemorethanonesubtypebut onesubtypepredominatesin atissue
Muscarinic Receptors -Location M1:AutonomicganglionCells,GastricglandsandCentralNeurons(cortex, hippocampus, corpusstriatum) PhysiologicalRole:Mediation ofGastricacidsecretion andrelaxationof LES(vagal) Learning,memoryandmotor functions M2:Cardiac Muscarinicreceptors M3:Visceralsmoothmuscles,glandsandvascularendothelium.AlsoIrisandCiliary muscles Mediate vagalbradycardia Alsoautoreceptorsincholinergic nerveendings CNS Tremor,analgesia
Muscarinic ReceptorSubtypes M1 M2 M3 SMs of Viscera, Eye, exocrine glands and endothelium Visceral SM contraction, glandular secretions, Constriction of pupil, contraction of Cilliary muscle and vasodilatation (EDRF -BNetOh)anechol Darifenacin Autonomic ganglia, Gastric glands and CNS Depolarization (late EPSP) & Histamine release & acid secretion, relaxation of LES, CNS learning and motor functions Location Heart and CNS Less impulse generation, less velocity of conduction, decreased contractility, less ACh release (auto) Functions Agonists Antagonists Oxotremorine Pirenzepine Methacholine Methoctramine & Triptramine K+ channel opening and decresed cAMP IP3/DAG and increase Ca++ and PG synthesis Transducer IP3/DAG and PLA2 increase Ca++ and PG
Acetylcholine (cholinergicreceptors) MuscarinicReceptors Selectively stimulated by Muscarine and blocked by Atropine M1 M2 M3 Ganglia, gastric gland and CNS Visceral Smooth Muscles, Iris and cilliary muscle Heart Cholinergic Nerves
Nicotinic (N)Receptors Nicotinicreceptors:nicotinicactionsofACharethosethat can be reproduced by the injection of Nicotine (Nicotiana tabacum) Canbeblockedbytubocurarineandhexamethonium Ligand-gated ionchannels activation resultsinarapidincreaseincellularpermeability to Na+andCa++resulting- depolarizationandinitiation ofactionpotential TWOTypes:NMandNN basedonlocation
Question? Apersonishavingseverecholinergic symptomslike vomiting, salivationand lacrimation etc. after accidental consumption of poisonous mushroom. Whatsubtypeof receptorisinvolvedinthemediationof suchreaction ..???? Answer:M3
Question? Whatsideeffectsmight youexpectto seeinapatienttaking acholinergic drug? Hint = Colon-Urgent .Cholinergic
Cholinergic Drugs or Cholinomimeticor Parasympathomimetics DrugsproducingactionssimilartoAcetylcholineby 1)interacting with Cholinergic receptors or 2) increasing availability of Acetylcholine at thesesites
Classifiction - Direct-acting (receptoragonists) M agonist :>>.. N agonist Mixed acting Muscarin, nicotine methacholine bethonichol Pilocarpin acetylcholine carbachol
Cholinergic Drugs Indirectacting Reversible Natural:Physostigmine Synthetic: Neostigmine, Pyridostigmine,, Rivastigmine, Donepezil,, Edrophonium,, Irreversibleanticholinesterases: Organophosphorous Compounds (OPC) Diisopropyl fluorophosphate (DFP), Ecothiophate, Parathion, malathion, diazinon (insecticides and pesticides) Tabun, sarin, soman (nerve gases inwar)
Pilocarpine Alkaloidfromleavesof Jaborandi(Pilocarpusmicrophyllus) Prominent muscarinicactions Profuse salivation, lacrimation,sweating Dilates blood vessels, causeshypotension Highdoses:RiseinBPandtachycardia(ganglionicaction) OnEyes:producesmiosisandspasmof accommodation Lowersintraocularpressure(IOP)inGlaucomawhenappliedaseyedrops Tootoxic for systemicuse CNStoxicity Diaphoretic (?), xerostomiaand Sj gren s syndrome
Pilocarpine contd. 1. Usedaseyedropsintreatmentof narrow angle glaucoma toreduce IOP 2. Toreversemydriaticeffectofatropine 3. To break adhesion between iris and cornea/lens alternated withmydriatic Pilocarpinenitrateeyedrops(1to 4%) Atropine used as antidote in acute pilocarpinepoisoning(1-2mgIV8hrly)
Pilocarpine inGlaucoma Constriction of circular muscle of Iris Contraction of ciliary muscle Spasm of accommodation fixed at near vision
Muscarine Alkaloid frommushroom Amanita muscaria Only muscarinicactions No clinicaluse Mushroompoisoningdueto ingestionof poisonousmushroom 1.Early onset mushroom poisoning (Muscarinetype) inocybe and clitocybe 2.Late onset mushroom poisoning aminata phallides 3.Hallucinogenictype aminata muscira
MushroomPoisoning EarlyOnsetMushroomPoisoning:Occurs to1hour Symptomsarecharacteristicof Muscarinicactions Inocybe or Clitocybe severe cholinergic symptoms like vomiting, salivation, lacrimation, headache,bronchospasm,diarrhoeabradycardia,dyspnoea,hypotension, weakness,cardiovascularcollapse,convulsionsandcoma AntidoteisAtropinesulphate(2-3mgIMeveryhrlytill improvement) Hallucinogenictype:amanita muscira dueto Muscimolor ibotenic acid present in A. muscria. Blocks muscarinic receptors in brain and activate amino acid receptors. No specific treatment Atropine contraindicated.
Late OnsetMushroom Poisoning Occurswithin6- 15hours Amanitaphylloides(deadlynightcap),Galerina dueto peptidetoxins Inhibit RNA and proteinsynthesis Irritability, restlessness,nausea,vomiting,bloodydiarrhoeaataxia,hallucination, delirium,sedation,drowsinessandsleep Kidney,liverandGITmucosaldamage Maintain blood pressure,respiration Inj. Diazepam 5 mgIM Atropinecontraindicatedasit maycauseconvulsionsanddeath- penicillin, thioctic acid and silibinin(antidote?) Gastric lavage and activatedcharcoal DELAYEDONSETType (morethan24Hours) Nephrotoxicsyndromes
AChEs -MOA Normally Acetylcholinesterase (AchE)hydrolyses Acetylcholine TheactivesiteofAChEismadeupof two subsites anionic andesteratic Theanionicsiteservesto bindamoleculeof ACh to theenzyme Once the ACh is bound, the hydrolytic reaction occursat asecondregionofthe activesitecalled the esteraticsubsite TheAChEitselfgetsacetylatedat serinesite Acetylated enzyme reacts + water = aceticacid andcholine Choline - immediately taken up again by the high affinity choline uptake systempresynaptic membrane Tryptophan Glutamateand histidine
AChEs -MOA Anticholinesterasesalsoreactwith theenzymeChEsinsimilarfashionlike Acetylcholine Carbamates carbamylatetheactivesiteof theenzyme Phosphates Phosphorylate theenzyme Bothreactsimilarfashioncovalently with serine Carbamylated(reversibleinhibitors)reactswith waterslowlyandtheesteraticsite isfreedandreadyfor action 30minutes (lessthansynthesisof freshenzyme) But,Phosphorylated(irreversible)reactsextremelyslowlyornot at all takesmore time thansynthesisof freshenzyme Sometimesphosphorylated enzymelossesonealkylgroupandbecomeresistantto hydrolysis aging Edrophoniumandtacrinereactonlyat anionicsite shortactingwhile Organophosphatesreactonlyat esteraticsite
Physostigmine Alkaloidfromdryripenedseed(Calabarbean)ofAfricanplant Physostigma venenosum Tertiaryamine,lipid soluble,wellabsorbedorallyandcrossesBBB Hydrolyzedinliverandplasmabyesterases Longlastingaction(4-8hours) Penetratescorneareadily onlocalapplicationineye-Muscarinicactionon eyecausingmiosisandspasmof accommodationonlocalapplication Salivation,lacrimation,sweatingandincreasedtracheobronchialsecretions Increasedheartrate&hypotension
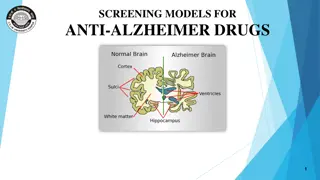
Physostigmine -uses 1. Usedasmioticdropsto decreaseIOPinGlaucoma 2. To antagonizemydriatic effectof atropine 3. Tobreakadhesionsbetweenirisandcorneaalternating with mydriatic drops 4. Belladonnapoisoning,TCAs&Phenothiazinepoisoning 5. Alzheimer sdisease-pre-senileorseniledementia 6. Atropineisantidote inphysostigminepoisoning. ADRs CNS stimulation followed bydepression
Neostigmine Synthetic reversible anticholinesterasedrug Quaternaryammoniumcompoundandlipidinsoluble Cannot crossBBB Hydrolysedbyesterasesinliver& plasma Shortdurationof action(3-5hours) Directactiononnicotinic(NM)receptorspresentinneuromuscularjunction(motor endplate)of skeletalmuscle Antagonises(reverses)skeletalmusclerelaxation(paralysis)causedby tubocurarine andother competitiveneuromuscularblockers Stimulates autonomic gangliainsmalldoses- Largedosesblockganglionic transmission No CNSeffects
Neostigmine Uses andADRs Usedinthetreatmentof MyastheniaGravisto increasemusclestrength Post-operative reversal ofneuromuscular blockade Post-operativecomplications gastricatonyparalytic ileus,urinarybladder atony Cobra snakebite Producestwitchings &fasciculationsof musclesleadingto weakness Atropineistheantidote inacuteneostigminepoisoning
Physostigmine VsNeostigmine Physostigmine Natural Tertiary amine Neostigmine Source Chemistr y Oral absorption CNS action Eye Effect Uses Dose Synthetic Quaternary ammonium compound Poor Absent Poor penetration Muscle Mysthenia gravis 0.5-2.5 mg IM/SC 15-30 mg orally 3-4 Hrs Good Present Penetrates cornea Ganglia Miotic 0.5-1 mg oral/parenteral 0.1-1% eye drop 4-6 Hrs Duration of action
OtherDrugs Pyridostigmine: Same as Neostigmine - less potent butlonger acting Edrophonium: Same as Neostigmine shorter duration ofaction (1--30minutes) diagnosticuseinMG Tacrine: Acts like edrophonium, lipid soluble, crosses BBB increasesbrainACh symptomaticimprovementinAlzheimer`s disease(AD) Rivastigmine,donepezil,galantamine allusedinAD
Myastheniagravis (Myo +asthenia) Autoimmune disorder affecting 1in 10,000population (?) reduction in number of NMreceptors Symptoms: Weakness andeasy fatigability ptosis todiaphragmatic paralysis Causes: Development ofantibodies directedto Nicotinicreceptorsin muscle end plate reduction in number by 1/3rd ofNM receptors Structural damage toNM junction
Myasthenia gravis otherdrugs Neostigmine 15to 30mg.orallyevery6hrly Adjustedaccordingto theresponse Pyridostigmine less frequency ofdosing Otherdrugs:Corticosteroids(prednisolone30-60mg/day) immunosuppression InhibitsproductionofNRantibodiesandmayincreasesynthesisorNRs Azathioprin and cyclosporinalso Plasmapheresis
Myastheniccrisis Acute weakness and respiratoryparalysis Tracheobronchial intubationand mechnical ventilation Methylprednisolone IVwith withdrawalofAChE Gradualreintroduction ofAChE Thymectomy Theproblem overtreatmentVsactualdisease(oppositetreatments) Diagnosisbyvarioustests TensilonTest Injection of Edrophonium 2mg(observe) afterhalfaminute 8mg(observe) In overtreatment symptoms worsen InMG symptomswill improve
OverallTherapeuticUsescholinergicdrugs 1. 2. 1. 1. 2. 3. Myastheniagravis:Edrophoniumto diagnoseandNeostigmine, Pyridostigmine & Distigmine totreat Tostimulatebladder& bowelafter surgery: Bethanechol, Carbachol,Distigmine. TolowerIOPinchronicsimpleglaucoma: Pilocarpine,Physostigmine To improvecognitivefunctioninAlzheimer sdisease:Rivastigmine, Gallantamine,Donepezil. Physostigmine in Belladonnapoisoning CobraBite
Pharmacotherapy ofOrganophosphate Poisoning Complexeffects Muscarinic,NicotinicandCNS Signs andsymptoms: 1. Irritationof eye,lacrmation, salivation,tracheo-bronchialsecretions,colic,blurring of vision, defaecation andurination 2. FallinBP ,tachyorbradycardia andCVScollapse 3. Muscularfasciculations,weakness,andrespiratoryparalysis 4. Irritability,disorientation,ataxia,tremor, convulsinsandcoma Treatment ABC Airway amaintance Breathing Give oxygen Circulation : two wide bore calunas then give normal saline Pass NG tube Pass foleys catheter ANTIDOT PRALIDOXIME Atropine 2mg IV every 10 minutes till dryness of mouth
Mukhtiar khan IMU KYRGYSTAN/Thank you













")
Receptors")



")