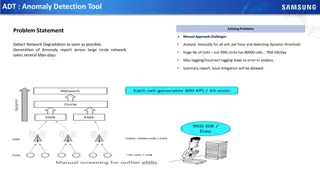
Revolutionary N-Assay: Transforming Pathogen Detection in Healthcare
Innovative N-Assay developed by Jonathan Faro, MD, PhD, offers a faster, more accurate, and cost-effective solution for detecting bacterial pathogens in healthcare settings. Unlike traditional assays, N-Assay differentiates between viable and non-viable pathogens, provides information on antibiotic effectiveness, and is customizable for various pathogens. Addressing the shortcomings of current diagnostics, this groundbreaking technology has the potential to revolutionize pathogen detection and improve patient outcomes.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
N-Assay Jonathan Faro, MD, PhD Medical Director, Nanologix, Inc Jonathan.Faro@outlook.com
Historical Context Historical Context -Traditionally, detection (via culture) of a clinically relevant bacterial pathogen takes 3 days -If the clinician needs to know what antibiotic to use, that may take an extra 2-3 days
As the patient is decompensating (experiencing deterioration of their system), the bacterial pathogen is flourishing!
State of Affairs State of Affairs In 2010, it was reported that 2 million people suffer from healthcare associated infections EVERY YEAR. Of these individuals, 90,000 DO NOT SURVIVE. Direct costs to hospitals due to these infections ranges from 28 to 45 billion, ANNUALLY. The majority of these infections ARE PREVENTABLE. However, the rate of these infections continues to rise. Patricia Stone, PhD. Economic Burden of Healthcare-Associated Infections: an American Perspective. Expert Rev Pharmacoecon Outcomes Res 2009 Oct:9(5):417-422
Immuno Immuno- -diagnostics diagnostics In order to more rapidly detect bacterial pathogens, a number of companies have offered tests that will more quickly identify bacteria Accelerate Diagnostics (Pheno System) Becton Dickinson (BD Max) bioMerieux (BACT-ALERT) Quidel (Solana Assay)
Problems with the current assays Problems with the current assays These assays are costly to run, and the machines are costly to maintain They require specialized training They lack sensitivity They lack specificity Overall, diagnostic accuracy is poor They are not able to differentiate between viable/non-viable pathogens They do not offer any info regarding the size of the inoculum These tests do not offer the clinician any information regarding which antibiotic will be effective/ineffective
The Solution: The N The Solution: The N- -Assay Assay Very inexpensive to manufacture Does not require specialized training to run Differentiates between viable and non-viable pathogens May be tailored for potentially any bacterial/fungal pathogen Shows an incredibly high degree of sensitivity and specificity Is faster than other tests, providing results in as little as 30 minutes to 6 hours. One huge advantage over the other tests: The N-Assay allows for the simultaneous detection of a bacteria and the determination of antibiotic susceptibility
How does the N How does the N- -Assay Work? Assay Work? Antibodies generated against the target pathogen pull down, or isolate the pathogen from a complex biological sample Sample may be from any body source, such as urine, blood, vaginal-rectal specimen, etc. After 30 minutes, a target antibody is applied, detecting high inoculum of specific pathogen present If lower inoculum is present, incubation time is increased, leading to the test delivering more sensitive results. Antibiotics may be added during a 6 hour incubation period, allowing the clinician to determine what antibiotics will work to target the pathogen more effectively. This allows for: More rapid de-escalation of antibiotics Reduction in the development of antimicrobial resistance Economic savings, as antibiotics are not wasted/used indiscriminately Reduction in the number of allergic reactions that occur, as patients are not needlessly exposed to antibiotics while they await the results of culture
Future of the N Future of the N- -Assay Assay Currently, the assay has been formulated for both dot-blot and ELISA methodologies. We are actively engaged in developing the assay into a lateral flow assay (LFA). Configuring the assay into an LFA will allow: True Point-of-care ability (POC). The test will then be able to be run in the clinic, on labor and delivery, at the patient s bedside, or even in some cases, by the patient themselves, at home. The test will also be configured in the format of specific panels, so that the clinician may run either a Sepsis N-Assay, a Chronic UTI N- Assay, or a Preterm labor/Early onset neonatal sepsis N-Assay, depending on the clinician s needs. Targeting the assay for specific clinical scenarios will help save money and streamline results.
Clinical Applications Clinical Applications Urinary Tract Infections: Over 400,000 hospitalizations in 2011 alone Cost of 2.8 billion, or 4,500.00 - 6,500.00 per patient admission More patients with UTIs are being admitted, out of fear of the observed increase in antimicrobial resistance Link: 10.1093/ofid/ofw281
Clinical Applications Clinical Applications Very low Birth Weight (< 1,500 grams) or (< 3.3 Lbs) Preterm delivery, Ruptured membranes, Chorioamnionitis each contribute to low birth weight infants. This number represents 1.5% of all live births in the United States. Cost in the US alone is 13.4 billion dollars. This is 30% of the total newborn healthcare costs Average length of admission to the NICU is over 50 days. Link: 10.1016/j.jpeds.2012.07.013
Clinical Applications Clinical Applications Respiratory Infections 1.25 million patients are hospitalized each year for community-acquired respiratory tract infections Annual cost is over 4 billion dollars for these patients 300,000 thousand patients develop nosocomial upper respiratory tract infections each year Annual cost is over 470 million for these patients Outpatient costs exceed 10 billion dollars annually Cost to treat both upper and lower respiratory tract infections each year is over 15 billion dollars. Physicians charge approximately half of these fees, while hospital costs are approximately one quarter of these fees. Link: PMID4014287
Clinical Applications Clinical Applications Sepsis Sepsis is the most expensive condition to treat in the entire US healthcare system. In 2013, it was estimated that the cost was 24 billion, annually. Treatment of sepsis is responsible for over 6% of all funding for healthcare. Over 250,000 people die from sepsis in the US each year, or one person every two minutes. https://www.sepsis.org/sepsis-alliance-news/new-u-s-government-report-reveals- annual-cost-of-hospital-treatment-of-sepsis-has-grown-by-3-4-billion/
Global Diagnostics Market Global Diagnostics Market In the US alone, the market in diagnostics is expected to grow to 20 billion by the year 2022. Globally, this is anticipated to reach 31 billion by 2026. Given the unique features of the N-Assay (its ability to identify a pathogen and simultaneously determine the correct antibiotic to guide treatment), its ease of use (may be developed as a point-of- care test, which may be used at the patient s bedside, in the clinic, or even at home), its low cost to manufacture, its high rate of accuracy (see publications listed on next slide), and its ability to differentiate between viable and non-viable pathogens, this assay is well positioned to dominate the market.
References References Song JY, Lin LL, Shott S, Kimber N, Tangora J, Cohen A, Wells A, Maezes M, Aroutcheva A, Faro S. Evaluation of the Strep B OIA test compared to standard culture methods for detection of group B streptococci. Infect Dis Obstet Gynecol. 1999;7(4):202-5. https://doi.org/10.1002/(SICI)1098-0997(1999)7:4<202::AID-IDOG8>3.0.CO;2-D Davies HD, Miller MA, Faro S, Gregson D, Kehl SC, Jordan JA. Multicenter study of a rapid molecular-based assay for the diagnosis of group B Streptococcus colonization in pregnant women. Clin Infect Dis. 2004 Oct 15;39(8):1129-35. Faro J, Katz A, Bishop K, Riddle G, Faro S. Rapid diagnostic test for identifying group B streptococcus. Am J Perinatol. 2011 Dec;28(10):811-4. Faro JP, Bishop K, Riddle G, Ramirez MM, Katz AR, Turrentine MA, Faro S. Accuracy of an accelerated, culture-based assay for detection of group B streptococcus. Infect Dis Obstet Gynecol. 2013;2013:367935. http://dx.doi.org/10.1155/2013/367935 Faro J, Mitchell M, Chen YJ, Kamal S, Riddle G, Faro S. Development of a novel test for simultaneous bacterial identification and antibiotic susceptibility. Infect Dis Obstet Gynecol. 2016;2016:5293034. http://dx.doi.org/10.1155/2016/5293034