Cardiovascular Outcomes Trials with GLP-1 Receptor Agonists
GLP-1 receptor agonists are newer non-insulin-based glucose-lowering therapies with demonstrated cardiovascular benefits. This educational module covers completed CVOTs involving GLP-1 receptor agonists, treatment options for type 2 diabetes, study designs, results, and a timeline of new treatment options. Various CVOTs with GLP-1 receptor agonists like liraglutide, exenatide, and ertugliflozin are discussed along with their outcomes. The modules provide valuable insights into the evolving landscape of diabetes management.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Cardiovascular outcomes trials with GLP-1 receptor agonists EDUCATIONAL SLIDE MODULE Date of preparation: September 2022 Version 5.0 SC-CRP-03320
CVOTs with GLP-1 receptor agonists Treatment options for T2D including recent therapeutic classes Completed GLP-1 receptor agonist CVOTs Study design of GLP-1 receptor agonist CVOTs Results of completed GLP-1 receptor agonist CVOTs Summary
CVOTs with GLP-1 receptor agonists Treatment options for T2D including recent therapeutic classes Completed GLP-1 receptor agonist CVOTs Study design of GLP-1 receptor agonist CVOTs Results of completed GLP-1 receptor agonist CVOTs Summary
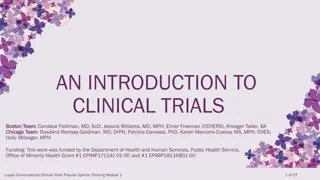
Timeline of new treatment options16 GLP-1 receptor agonists are newer, non-insulin-based glucose-lowering therapies 1920 1950 1960 1970 1980 1990 2000 2010 2012 2013 Discovery of insulin Insulin lispro developed Insulin glargine4 Pioglitazone (TZD)4 Initial FDA approval of: -glucosidase inhibitors TZDs Lente insulins introduced Recombinant human insulin FDA approved GLP-1 receptor agonists 4 7 Insulin degludec4 Metformin introduced to treat diabetes* Meglitinides Second- generation SUs first available in the US Third-generation SU (glimepiride) first available Sulphonylureas first available DPP-4 inhibitors4 SGLT2 inhibitors 4 GLP-1 receptor agonist SGLT2 inhibitor DPP-4 inhibitor Other *Metformin approved (1994) and introduced (1995) in the US3; Liraglutide, albiglutide, dulaglutide, oral semaglutide, and efpeglenatide have demonstrated CV benefit4 7; Superiority for 3P-MACE demonstrated by empagliflozin and canagliflozin; superiority for HHF or CV death but not for 3P-MACE was demonstrated for dapagliflozin; superiority for HHF demonstrated by ertugliflozin8 11 See slide notes for abbreviations and full list of references 4
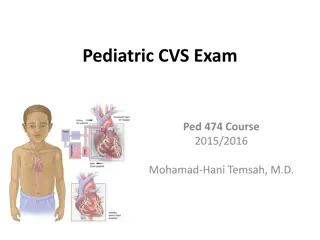
CVOTs are being conducted for compounds within the recent classes of glucose-lowering agents in patients with T2D DECLARE-TIMI 5816 Dapagliflozin N=17,160 3P-MACE and CV death or HHF FREEDOM-CVO7,8 ITCA 650 N=4156 4P-MACE SAVOR-TIMI 531 Saxagliptin N=16,492 EXSCEL11 Exenatide N=14,752 VERTIS CV19 Ertugliflozin N=8246 TECOS4 Sitagliptin N=14,671 4P-MACE EXAMINE2 Alogliptin N=5380 LEADER6 Liraglutide N=9340 CARMELINA12 Linagliptin N=6979 CAROLINA17 Linagliptin N=6041 AMPLITUDE-O20 Efpeglenatide N=4076 2013 2014 2015 2016 2017 2018 2019 2020 2021 ELIXA3 Lixisenatide N=6068 4P-MACE 2024 CANVAS Program10 Canagliflozin N=10,142 Harmony Outcomes13 Albiglutide N=9463 SOUL21 Semaglutide (oral) N=9642 EMPA-REG OUTCOME5 Empagliflozin N=7020 SUSTAIN-69 Semaglutide (inj.) N=3297 REWIND14,15 Dulaglutide N=9901 PIONEER 618 Semaglutide (oral) N=3183 GLP-1 receptor agonist SGLT2 inhibitor DPP-4 inhibitor Markers on timeline represent trial completion (except for SOUL, for which an estimated trial completion date is provided) as per ClinicalTrials.gov Primary endpoint is 3P-MACE unless otherwise indicated See slide notes for abbreviations and full list of references 5
CVOTs are being conducted for compounds within the GLP-1 receptor agonist class in patients with T2D FREEDOM-CVO3,4 ITCA 650 N=4156 4P-MACE EXSCEL6 Exenatide N=14,752 LEADER2 Liraglutide N=9340 AMPLITUDE-O11 Efpeglenatide N=4076 2013 2014 2015 2016 2017 2018 2019 2020 2021 ELIXA1 Lixisenatide N=6068 4P-MACE 2024 Harmony Outcomes7 Albiglutide N=9463 SOUL12 Semaglutide (oral) N=9642 SUSTAIN-65 Semaglutide (inj.) N=3297 REWIND8,9 Dulaglutide N=9901 PIONEER 610 Semaglutide (oral) N=3183 Markers on timeline represent trial completion (except for SOUL, for which an estimated trial completion date is provided) as per ClinicalTrials.gov Primary endpoint is 3P-MACE unless otherwise indicated See slide notes for full list of references 6
CVOTs with GLP-1 receptor agonists Treatment options for T2D including recent therapeutic classes Completed GLP-1 receptor agonist CVOTs Study design of GLP-1 receptor agonist CVOTs Results of completed GLP-1 receptor agonist CVOTs Summary
GLP-1 receptor agonists have pharmacological differences Pharmacological properties of GLP-1 receptor agonists Exendin based Non-exendin based Injectable semaglutide8 Oral Exenatide IR1Exenatide ER2Lixisenatide3Efpeglenatide*4,5Liraglutide6 Dulaglutide7 semaglutide9Albiglutide*10 2 mg 4 mg qw or 2 mg 4 mg 6 mg qw 0.75 1.5 mg 3 mg 4.5 mg qw 0.25 mg 0.5 mg 1 mg 2 mg qw 0.6 mg 1.2 1.8 mg qd 3 mg 7 mg 14 mg qd 5 g 10 g bid 10 g 20 g qd 30 50 mg qw Dosage 2 mg qw Peak plasma concentration (post dose) 2 hours 6 7 weeks 1 3.5 hours 48 72 hours 8 12 hours 48 hours 1 3 days 1 hour 3 5 days Elimination half-life Not 2.4 hours ~3 hours ~6.5 days ~13 hours ~5 days ~1 week ~1 week ~5 days determined Exendin-based therapies are based on the naturally occurring Heloderma suspectum peptide exendin 4, which shares ~50% homology with human GLP-111 *Not approved for treatment of T2D; All therapies administered subcutaneously except for oral semaglutide; For additional glycaemic control ER, extended release; IR, immediate release See slide notes for full list of references 8
Summary of completed GLP-1 receptor agonist CVOTs Harmony Outcomes5 ELIXA1 LEADER2 SUSTAIN-6 3 EXSCEL4 REWIND6 PIONEER 6 7 AMPLITUDE-O8 Efpeglenatide 2 mg qw 4 mg qw / 4 mg qw 6 mg qw Inj. semaglutide 0.5 mg qw/ 1.0 mg qw Lixisenatide 10 20 g qd Liraglutide 1.8 mg qd Exenatide ER 2 mg qw Albiglutide 30 50 mg qw Dulaglutide 1.5 mg qw Oral semaglutide 3 7 14 mg qd Study drug* 6068 9340 3297 14,752 9463 9901 3183 4076 Number of patients, N T2D + CVD and/or CKD stage 3 or higher or CV risk T2D T2D + CVD or CV risk T2D + CVD and/or CKD stage 3 or CV risk T2D + CVD or CV risk T2D + established CVD T2D + CVD or CV risk T2D + ACS with/without CV event Patient population 5.5 11.0 6.5 10.0 >7.0 NR >7.0 HbA1c inclusion, % 7.0 7.0 9.5 2.1 3.8 2.1 3.2 ~1.6 5.4 1.3 1.81 Median follow-up, years 805 1302 254 1744 766 1257 137 314 Number of MACE events HR 1.02 (95% CI 0.89, 1.17); p=0.81 HR 0.87 (95% CI 0.78, 0.97); p<0.01 HR 0.74 (95% CI 0.58, 0.95); p<0.02 ** HR 0.91 (95% CI 0.83, 1.00); p=0.06 HR 0.78 (95% CI 0.68, 0.90); p=0.0006 HR 0.88 (95% CI 0.79, 0.99); p=0.026 HR 0.79 (95% CI 0.57, 1.11); p=0.17 HR 0.73 (95% CI 0.58, 0.92); p=0.007 Primary outcome (MACE) result Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 RA trials included in the 2022 ADA Standards of Care9 are presented *All trials used placebo as a comparator; Non-inferiority margin for upper bound of 95% CI: <1.8; superiority testing for MACE was prespecified in PIONEER 6 but not in SUSTAIN-6; Dose-escalation regimen; p-value for superiority; all trials demonstrated non-inferiority vs comparator. All trials had a primary outcome of 3P-MACE, apart from ELIXA and FREEDOM-CVO, which used 4P-MACE; Nominal p-value; **Doses pooled for analysis See slide notes for abbreviations and full list of references 9
Baseline characteristics in completed GLP-1 receptor agonist CVOTs Harmony Outcomes5 (N=9463) AMPLITUDE- O8 (N=4076) ELIXA1 (N=6068) LEADER2 (N=9340) SUSTAIN-63 (N=3297) EXSCEL4 (N=14,752) REWIND6 (N=9901) PIONEER 67 (N=3183) Age, years, mean 60.3 64.3 64.6 62.7* 64.2 66.2 66 64.5 HbA1c, %, mean 7.7 8.7 8.7 8.0* 8.74 7.2* 8.2 8.91 BMI, kg/m2, mean 30.2 32.5 32.8 31.8* 32.3 32.3 32.3 32.7 SBP, mmHg, mean 130 135.9 135.6 135.0* 134.8 137.2 136 134.9 DBP, mmHg, mean NR 77.1 77.0 80.0* 76.8 78.5 76 76.7 HDL-C, mmol/l, mean 1.1 NR 1.1 NR NR 1.18 NR 1.11 LDL-C, mmol/l, mean 2.0 NR 2.1 2.3* NR 2.56 2.0 2.07 Current smoker/tobacco use, % 11.7 NR NR 11.7 16 14.2 11.0 15.5 Definitions of baseline characteristics vary across trials Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care9 are presented *Reported as median; Conversion factor: 1 mg/dl = 0.02586 mmol/l for cholesterol. NR, not reported 1. Pfeffer MA et al. N Engl J Med 2015;373:2247; 2. Marso SP et al. N Engl J Med 2016;375:311; 3. Marso SP et al. N Engl J Med 2016;375:1834; 4. Holman RR et al. N Engl J Med 2017;377:1228; 5. Hernandez AF et al. Lancet 2018;392:1519; 6. Gerstein HC et al. Lancet 2019;394:121; 7. Husain M et al. N Engl J Med 2019;381:841; 8. Gerstein HC et al. N Engl J Med 2021;385:896; 9. American Diabetes Association. Diabetes Care 2022;45:S1 10
Baseline CV disease in completed GLP-1 receptor agonist CVOTs Harmony Outcomes5 (N=9463) AMPLITUDE- O8 (N=4076) ELIXA1 (N=6068) LEADER2 (N=9340) SUSTAIN-63 (N=3297) EXSCEL4 (N=14,752) REWIND6 (N=9901) PIONEER 67 (N=3183) Established CV disease 100 81.3* 83.0* 73.1 100 31.5 84.7* 89.6 Coronary artery disease 100 NR 60.5 52.8 70.6 NR 23.0 NR 72.1 NR NR NR NR NR NR NR ACS 3 months prior History of MI 22.1 30.7 32.5 NR 47.1 16.2 36.1 NR Coronary artery bypass 8.4 NR NR NR 18.3 NR NR NR History of stroke 5.5 16.1 NR 22.4 17.8 6.9 15.9 NR Peripheral artery disease 7.7 NR NR 19.0 24.9 8.7 NR NR Heart failure 22.4 14.0 23.6 16.2 20.3 8.6 12.2 18.1 Hypertension 76.4 NR 92.8 NR 86.5 93.2 NR 91.3 Definitions of baseline characteristics vary across trials Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care9 are presented All data are proportion of patients (%). *Established CV disease stratum requires age 50 years and includes history of CKD; History of symptomatic coronary heart disease; Prior stroke or TIA; Chronic HF NYHA class II III. See slide notes for abbreviations 1. Pfeffer MA et al. N Engl J Med 2015;373:2247; 2. Marso SP et al. N Engl J Med 2016;375:311; 3. Marso SP et al. N Engl J Med 2016;375:1834; 4. Holman RR et al. N Engl J Med 2017;377:1228; 5. Hernandez AF et al. Lancet 2018;392:1519; 6. Gerstein HC et al. Lancet 2019;394:121; 7. Husain M et al. N Engl J Med 2019;381:841; 8. Gerstein HC et al. N Engl J Med 2021;385:896; 9. American Diabetes Association. Diabetes Care 2022;45:S1 11
Baseline kidney function in completed GLP-1 receptor agonist CVOTs Harmony Outcomes6 (N=9463) AMPLITUDE- O9 (N=4076) ELIXA1 (N=6068) LEADER2,3 (N=9340) SUSTAIN-64 (N=3297) EXSCEL5 (N=14,752) REWIND7 (N=9901) PIONEER 6*8 (N=3183) eGFR, ml/min/1.73 m2, mean 76.0 80.0 NR 76.3 79.0 74.9* 74 72.4 90 ml/min/1.73 m2, % 23.4 35.1 30.0 29.0 29.8 NR 28.9 NR 60 to <90 ml/min/1.73 m2, % 53.4 41.8 41.5 49.3 46.7 NR 43.6 NR <60 ml/min/1.73 m2, % 23.2 23.1 28.5 21.7 23.5 22.2 26.9 31.6 Definitions of baseline characteristics vary across trials Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care10 are presented *Median value; Out of 14,705 patients. NR, not reported 1. Pfeffer MA et al. N Engl J Med 2015;373:2247; 2. Marso SP et al. N Engl J Med 2016;375:311; 3. Mann JFE et al. N Engl J Med 2017;377:839; 4. Marso SP et al. N Engl J Med 2016;375:1834; 5. Holman RR et al. N Engl J Med 2017;377:1228; 6. Hernandez AF et al. Lancet 2018;392:1519; 7. Gerstein HC et al. Lancet 2019;394:121; 8. Husain M et al. N Engl J Med 2019;381:841; 9. Gerstein HC et al. N Engl J Med 2021;385:896; 10. American Diabetes Association. Diabetes Care 2022;45:S1 12
Baseline medications in completed GLP-1 receptor agonist CVOTs Harmony Outcomes5 (N=9463) AMPLITUDE- O8 (N=4076) ELIXA1 (N=6068) LEADER2 (N=9340) SUSTAIN-63 (N=3297) EXSCEL4 (N=14,752) REWIND6 (N=9901) PIONEER 67 (N=3183) Glucose-lowering medications Insulin Sulphonylurea Metformin SGLT2 inhibitor DPP-4 inhibitor CV medications Statin Anti-thrombotic RAAS inhibitor Beta blocker Diuretic 39.1 33.0 66.3 NR 44.6 50.7 76.5 58.0 42.8 73.2 0.2 0.2* 46.3 36.6 76.5 0.9 14.9 59.1 28.8 73.6 6.1 15.2 23.9 46.0 81.2 NR 5.7 60.6 32.3 77.4 9.6 <0.1* 62.8 25.4 73.2 15.2 Excluded <0.1 Excluded Excluded 92.7 97.5 85.0 84.4 NR 72.2 67.7 82.9 55.5 41.8 72.8 76.3 NR 57.4 38.2 73.5 73.4 77.2 55.6 43.7 84.1 77.0 81.6 66.7 41.4 66.1 54.0 81.5 45.6 NR 85.2 79.4 NR NR 39.6 80.8 25.7 NR 65.5 NR Definitions of baseline characteristics vary across trials Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care9 are presented All data are proportion of patients (%). *Exclusion criteria; Lipid-lowering drugs; Patients on antiplatelet therapy; Patients on aspirin NR, not reported; RAAS, renin angiotensin aldosterone system 1. Pfeffer MA et al. N Engl J Med 2015;373:2247; 2. Marso SP et al. N Engl J Med 2016;375:311; 3. Marso SP et al. N Engl J Med 2016;375:1834; 4. Holman RR et al. N Engl J Med 2017;377:1228; 5. Hernandez AF et al. Lancet 2018;392:1519; 6. Gerstein HC et al. Lancet 2019;394:121; 7. Husain M et al. N Engl J Med 2019;381:841; 8. Gerstein HC et al. N Engl J Med 2021;385:896; 9. American Diabetes Association. Diabetes Care 2022;45:S1 13
CVOTs with GLP-1 receptor agonists Treatment options for T2D including recent therapeutic classes Completed GLP-1 receptor agonist CVOTs Study design of GLP-1 receptor agonist CVOTs Results of completed GLP-1 receptor agonist CVOTs Summary
ELIXA: study design1,2 Aim: a phase III trial to assess CV morbidity and mortality associated with lixisenatide versus placebo in post-ACS patients with T2D (non-inferiority margin: upper bound of 95% CI <1.3, superiority if 95% CI <1.0) Lixisenatide 10 20 g qd* + standard of care Safety follow-up Placebo run-in Placebo + standard of care Safety follow-up 1 week Median follow-up: 2.1 years 805 primary events 3 days Randomisation (1:1) Double-blind End of treatment Key inclusion criteria T2D Aged 30 years ACS event 180 days prior to screening Key exclusion criteria HbA1c <5.5% or >11.0% Use of incretin-based agents other than study agent eGFR <30 ml/min/1.73 m2 4P-MACE (CV death, non-fatal MI, non-fatal stroke or hospitalisation for unstable angina) Primary endpoint Composite of 4P-MACE or HHF; composite of 4P-MACE, revascularisation or HHF; all-cause mortality; individual components of each composite endpoint Key secondary endpoints *Starting dose of 10 g administered during the first 2 weeks and then increased to 20 g at the investigators discretion; Event-driven trial ACS, acute coronary syndrome; HHF, hospitalisation for heart failure 1. Pfeffer MA et al. N Engl J Med 2015;373:2247; 2. ClinicalTrials.gov. NCT01147250 (accessed Aug 2022) 15
LEADER: study design1,2 Aim: a phase III trial to assess the CV safety of liraglutide versus placebo on top of standard of care (non-inferiority margin: upper bound of 95% CI <1.3, superiority if 95% CI <1.0) Liraglutide 1.8 mg qd + standard of care Safety follow-up Placebo run-in Placebo + standard of care Safety follow-up 1 week Median follow-up:* 3.8 years 1302 primary events 30 days Randomisation (1:1) Double-blind End of treatment Key inclusion criteria T2D, HbA1c 7.0% Glucose-lowering drug na ve or 1 glucose-lowering agents and/or basal/premix insulin Aged 50 years with established CV disease or chronic kidney failure, or aged 60 years with 1 CV risk factor Key exclusion criteria T1D Acute coronary event or cerebrovascular event within 14 days before screening and randomisation Use of GLP-1 receptor agonists, DPP-4 inhibitors, pramlintide or rapid-acting insulin Familial or personal history of MEN-2 or MTC 3P-MACE (CV death, non-fatal MI or non-fatal stroke) Primary endpoint Composite of 3P-MACE, revascularisation, HHF or hospitalisation for unstable angina; all-cause mortality; composite of nephropathy or retinopathy Key secondary endpoints *Time- and event-driven trial; minimum planned duration of treatment exposure was 3.5 years HHF, hospitalisation for heart failure; MEN-2, multiple endocrine neoplasia type 2; MTC, medullary thyroid cancer 1. Marso SP et al. N Engl J Med 2016;375:311; 2. ClinicalTrials.gov. NCT01179048 (accessed Aug 2022) 16
SUSTAIN-6: study design1,2 Aim: a phase III trial to assess the CV safety of injectable semaglutide relative to current usual care (non-inferiority margin: upper bound of 95% CI <1.8; testing for superiority was not prespecified) Semaglutide Semaglutide 1.0 mg qw + standard of care Safety follow-up Semaglutide Semaglutide 0.5 mg qw + standard of care Safety follow-up Placebo Placebo + standard of care Safety follow-up Placebo Placebo + standard of care Safety follow-up Dose escalation 4 8 weeks Median follow-up:* 2.1 years 254 primary events 5 weeks Randomisation (1:1:1:1) Double-blind End of treatment Key inclusion criteria T2D, HbA1c 7.0% Glucose-lowering drug na ve or 2 glucose-lowering agents and/or basal/premix insulin Aged 50 years with established CV disease, chronic HF or CKD stage 3 or higher or aged 60 years with one CV risk factor Key exclusion criteria Use of GLP-1 receptor agonist or DPP-4 inhibitor Use of insulin other than basal/premix Coronary or cerebrovascular event within 90 days prior to study Chronic haemodialysis or chronic peritoneal dialysis 3P-MACE (CV death, non-fatal MI or non-fatal stroke) Composite of 3P-MACE, revascularisation, HHF or hospitalisation for unstable angina; composite of all-cause mortality, non-fatal MI or non-fatal stroke; retinopathy complications; new or worsening nephropathy Primary endpoint Key secondary endpoints *Event-driven trial; treatment duration of 2 years HHF, hospitalisation for heart failure 1. Marso SP et al. N Engl J Med 2016;375:1834; 2. ClinicalTrials.gov. NCT01720446 (accessed Aug 2022) 17
EXSCEL: study design1,2 Aim: aphase III trial to assess the CV safety of once-weekly exenatide versus placebo on top of standard of care in adults with T2D, with or without a previous CV event (margin for upper bound of 95% CI: non-inferiority, <1.3; superiority, <1.0) Exenatide ER 2 mg qw + standard of care Safety follow-up No placebo run-in* Placebo + standard of care Safety follow-up Median follow-up: 3.2 years 1744 primary events 70 days Randomisation (1:1) Double-blind End of treatment Key inclusion criteria Adults with T2D HbA1c 6.5% and 10.0% 70% of patients with a prior CV event 30% of patients with no prior CV event Key exclusion criteria eGFR <30 ml/min/1.73 m2 Prior use of GLP-1 receptor agonists T1D or history of DKA History of severe hypoglycaemia 3P-MACE (CV death, non-fatal MI or non-fatal stroke) Primary endpoint All-cause mortality, CV death, HHF, hospitalisation for ACS Key secondary endpoints EXSCEL was designed as a pragmatic trial with minimum protocol mandates and resource utilisation. *Absence of run-in period results in a protocol closer to routine clinical practice; Event-driven trial; Defined as history of major clinical manifestation of coronary artery disease, ischaemic cerebrovascular disease or atherosclerotic peripheral artery disease ACS, acute coronary syndrome; DKA, diabetic ketoacidosis; ER, extended release; HHF, hospitalisation for heart failure 1. Holman RR et al. N Engl J Med 2017;377:1228; 2. ClinicalTrials.gov. NCT01144338 (accessed Aug 2022) 18
Harmony Outcomes: study design1-3 Aim: a phase IV trial to assess the CV safety of albiglutide versus placebo on top of standard of care (margin for upper bound of 95% CI: non-inferiority, <1.3; superiority, <1.0) Albiglutide 30 50 mg qw* + standard of care (n=4731) Safety follow-up No placebo run-in Placebo + standard of care (n=4732) Safety follow-up Median follow-up: 1.6 years 766 primary events 5 weeks Randomisation (1:1) Double-blind End of treatment Key inclusion criteria Adults with T2D HbA1c 7.0% Atherosclerotic CV disease Key exclusion criteria eGFR <30 ml/min/1.73 m2 Current use of GLP-1 receptor agonists Previous or substantial risk of pancreatitis 3P-MACE (CV death, non-fatal MI, non-fatal stroke) Primary endpoint 4P-MACE, CV death, MI, stroke, composite of CV death or HHF, microvascular event composite, time to initiation of chronic insulin therapy, change in HbA1c and body weight Key secondary endpoints Albiglutide is not approved for the treatment of T2D *Dose could be uptitrated by the study investigator to 50 mg after 5 weeks of study treatment; Time- and event-driven trial; median planned duration of follow-up was 1.5 years; Defined as disease of the coronary, cerebrovascular or peripheral arterial circulation; Defined as CV death, MI, stroke or urgent revascularisation for unstable angina; Defined as need for kidney transplant or dialysis, new diabetes-related blindness and procedures (laser photocoagulation or anti-VEGF treatment or vitrectomy) HHF, hospitalisation for heart failure; VEGF, vascular endothelial growth factor 1. Green JB et al. Am Heart J 2018;203:30; 2. Hernandez AF et al. Lancet 2018;392:1519; 3. ClinicalTrials.gov. NCT02465515 (accessed Aug 2022) 19
REWIND: study design1,2 Aim: a phase III trial to assess the CV efficacy and safety of once-weekly dulaglutide versus placebo on top of standard of care in adults with T2D (superiority comparison to detect HR 0.82) Dulaglutide 1.5 mg qw + standard of care 3-week placebo run-in Placebo qw + standard of care Median follow-up:* 5.4 years 1257 primary events Screening Randomisation (1:1) Double-blind (N=9901) End of treatment Key inclusion criteria Adults aged 50 years with T2D and HbA1c 9.5% Aged 50 years with vascular disease Aged 55 years with subclinical vascular disease Aged 60 years with 2 risk factors Key exclusion criteria eGFR <15 ml/min/1.73 m2 or on dialysis at screening Coronary or cerebrovascular event in preceding 2 months Use of GLP-1 receptor agonist or DPP-4 inhibitor Severe hypoglycaemia in the preceding year 3P-MACE (CV death [or death from unknown causes], non-fatal MI, non-fatal stroke) Primary endpoint Non-fatal MI, non-fatal stroke, death from CV or unknown causes, composite microvascular outcome, all-cause mortality, heart failure requiring either hospital admission or an urgent visit requiring therapy, hospitalisation for unstable angina Key secondary endpoints *Event-driven trial; Previous MI, ischaemic stroke, revascularisation, hospital admission for unstable angina or imaging evidence of myocardial ischaemia; Myocardial ischaemia, coronary, carotid or lower extremity artery stenosis exceeding 50%, left ventricular hypertrophy, eGFR <60 ml/min/1.73 m2 or albuminuria; Tobacco use, dyslipidaemia, hypertension or abdominal obesity; Eye outcomes (photocoagulation, anti-VEGF therapy or vitrectomy) or kidney outcomes (UACR >33.9 mg/mmol in patients with a lower baseline concentration, sustained decline in eGFR of 30% or chronic renal replacement therapy) VEGF, vascular endothelial growth factor 1. Gerstein HC et al. Lancet 2019;394:121; 2. ClinicalTrials.gov. NCT01394952 (accessed Aug 2022) 20
PIONEER 6: study design1,2 Aim: a phase III trial to assess the CV safety of oral semaglutide versus placebo on top of standard of care in adults with T2D at high risk of CV events (margin for upper bound of 95% CI: non-inferiority, <1.8; superiority testing was performed on the primary outcome if non-inferiority confirmed) Safety follow-up Oral semaglutide 3 7 14 mg qd*+ standard of care No placebo run-in Oral placebo + standard of care Safety follow-up Median follow-up: 1.3 years 137 primary events 5 weeks Randomisation (1:1) Double-blind End of treatment Key inclusion criteria Adults with T2D (no lower HbA1c threshold) Aged 50 years with pre-existing CV disease and/or stage 3 CKD or aged 60 years with 1 CV risk factor Key exclusion criteria Haemodialysis or eGFR <30 ml/min/1.73 m2 Prior treatment with a GLP-1 receptor agonist, DPP-4 inhibitor or pramlintide <90 days before screening NYHA class IV HF 3P-MACE (CV death, non-fatal MI or non-fatal stroke) Primary endpoint Expanded composite outcome (3P-MACE + HHF or hospitalisation for unstable angina), composite of all-cause mortality, non-fatal MI or non-fatal stroke, individual components of composite CV outcomes Key secondary endpoints *Dose-escalation regimen to mitigate potential for GI AEs of 3 mg qd for 4 weeks, 7 mg qd for 4 weeks and 14 mg qd for the remainder of the trial; Event-driven trial; Patients had prior MI, prior stroke/TIA, coronary/carotid/peripheral arterial revascularisation, >50% stenosis of coronary/carotid/lower extremity arteries, history of CHD, asymptomatic cardiac ischaemia or chronic HF (NYHA class II III), or eGFR 30 59 ml/min/1.73 m2; Defined as microalbuminuria, proteinuria, LV dysfunction, ankle/brachial index <0.9, or hypertension and LV hypertrophy AE, adverse event; CHD, coronary heart disease; GI, gastrointestinal; HHF, hospitalisation for heart failure; LV, left ventricular; NYHA, New York Heart Association 1. Husain M et al. N Engl J Med 2019;381:841; 2. ClinicalTrials.gov. NCT02692716 (accessed Aug 2022) 21
AMPLITUDE-O: study design1,2 Aim: a phase III trial to assess the CV safety of efpeglenatide versus placebo on top of standard of care in adults with T2D at high CV risk (margin for upper bound of 95% CI: non-inferiority, <1.8; superiority testing was performed on the primary outcome if non-inferiority confirmed) Safety follow-up Efpeglenatide 2 4 mg qw* + standard of care No Efpeglenatide 2 4 6 mg qw + standard of care Safety follow-up placebo run-in Placebo + standard of care Safety follow-up Median follow-up: 1.81 years 314 primary events 6 weeks Randomisation (1:1:1) Quadruple-blind End of treatment Key inclusion criteria Adults with T2D and HbA1c >7% Aged 18 years with pre-existing CV disease or aged 50 years (if male) or aged 55 years (if female) with kidney disease and 1 additional CV risk factor Key exclusion criteria Gastroparesis, uncontrolled reflux, prolonged nausea or vomiting, severe retinal disease or pancreatitis Prior treatment with a GLP-1 receptor agonist, DPP-4 inhibitor <3 months before screening 3P-MACE (CV death [or death from unknown causes], non-fatal MI or non-fatal stroke) Primary endpoint Expanded composite outcome (3P-MACE + coronary revascularisation or hospitalisation for unstable angina), composite renal outcome (incident macroalbuminuria** + increase in UACR of 30% from baseline, 40% decrease in eGFR for 30 days, renal-replacement therapy for 90 days or eGFR of <15 ml/min/1.73 m2for 30 days) Key secondary endpoints *2 mg qw for 4 weeks and then 4 mg qw until the end of the trial; 2 mg qw for 4 weeks, then 4 mg qw for 4 weeks, and then 6 mg qw until the end of the trial; Defined as coronary artery disease, stroke or peripheral artery disease; Defined as eGFR 25.0 59.9 ml/min/1.73 m2; **Defined as UACR >300 mg/g or >33.9 mg/mmol 1. Gerstein HC et al. N Engl J Med 2021;385:896; 2. ClinicalTrials.gov. NCT03496298 (accessed Aug 2022) 22
CVOTs with GLP-1 receptor agonists Treatment options for T2D including recent therapeutic classes Completed GLP-1 receptor agonist CVOTs Study design of GLP-1 receptor agonist CVOTs Results of completed GLP-1 receptor agonist CVOTs Summary
MACE in completed GLP-1 receptor agonist CVOTs in patients with T2D FDA-mandated upper 95% CI for CV safety* Study drug Placebo IR IR n with event/ N analysed (%) n with event/ N analysed (%) (events/ 100 PY) (events/ 100 PY) p-value HR (95% CI) ELIXA1 (lixisenatide) LEADER2 (liraglutide) SUSTAIN-63 (inj. semaglutide) EXSCEL4 (exenatide) Harmony Outcomes5 (albiglutide) 406/3034 (13.4) 6.4 399/3034 (13.2) 6.3 1.02 (0.89, 1.17) 0.81 608/4668 (13.0) 3.4 694/4672 (14.9) 3.9 0.87 (0.78, 0.97) 0.01 108/1648 (6.6) 3.24 146/1649 (8.9) 4.44 0.74 (0.58, 0.95) 0.02 839/7356 (11.4) 3.7 905/7396 (12.2) 4.0 0.91 (0.83, 1.00) 0.06 338/4731 (7) 4.57 428/4732 (9) 5.87 0.78 (0.68, 0.90) 0.0006 REWIND 6 (dulaglutide) 594/4949 (12.0) 2.35 663/4952 (13.4) 2.66 0.88 (0.79, 0.99) 0.026 PIONEER 67 (oral semaglutide) AMPLITUDE-O8 (efpeglenatide) 61/1591 (3.8) 2.9 76/1592 (4.8) 3.7 0.79 (0.57, 1.11) 0.17 189/2127 (7.0) 3.9 125/1359 (9.2) 5.3 0.73 (0.58, 0.92) 0.007 1.3 1.8 0.25 0.5 1 2 Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care9 are presented *FDA-mandated upper 95% CI of the HR for CV safety is a margin of 1.3 for post-approval and 1.8 for pre-approval. SUSTAIN-6 and PIONEER 6 were pre-approval trials. p-values for superiority; all trials showed significance for non-inferiority; Nominal p-value; in SUSTAIN-6, testing for superiority was not prespecified or adjusted for multiplicity; After accounting for =0.009 spent on the primary outcome for the interim analysis, the for the final analysis is 0.0467 and the HR is 0.88 (95.33% CI 0.79, 0.99). See slide notes for abbreviations and full list of references Favours study drug Favours placebo 24
CV death in completed GLP-1 receptor agonist CVOTs in patients with T2D Study drug Placebo IR IR n with event/ N analysed (%) n with event/ N analysed (%) (events/ 100 PY) (events/ 100 PY) p-value HR (95% CI) ELIXA1 (lixisenatide) LEADER2 (liraglutide) SUSTAIN-63 (inj. semaglutide) EXSCEL4 (exenatide) Harmony Outcomes5 (albiglutide) 156/3034 (5.1) 2.3 158/3034 (5.2) 2.4 0.98 (0.78, 1.22) 0.85 219/4668 (4.7) 1.2 278/4672 (6.0) 1.6 0.78 (0.66, 0.93) 0.007* 44/1648 (2.7) 1.29 46/1649 (2.8) 1.35 0.98 (0.65, 1.48) 0.92 340/7356 (4.6) 1.4 383/7396 (5.2) 1.5 0.88 (0.76, 1.02) NR 122/4731 (3) 1.61 130/4732 (3) 1.72 0.93 (0.73, 1.19) 0.578 REWIND 6 (dulaglutide) 317/4949 (6.4) 1.22 346/4952 (7.0) 1.34 0.91 (0.78, 1.06) 0.21 PIONEER 67 (oral semaglutide) 15/1591 (0.9) 0.7 30/1592 (1.9) 1.4 0.49 (0.27, 0.92) NR AMPLITUDE-O8 (efpeglenatide) 75/2717 (2.8) 1.5 50/1359 (3.7) 2.1 0.72 (0.50, 1.03) NR 0.25 0.5 1 2 Favours study drug Favours placebo Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care9 are presented *Nominal p-value; p-value not reported in publication; Includes death from unknown cause IR, incidence rate; NR, not reported; PY, patient-years See slide notes for full list of references 25
Stroke in completed GLP-1 receptor agonist CVOTs in patients with T2D Study drug Placebo IR IR n with event/ N analysed (%) n with event/ N analysed (%) (events/ 100 PY) (events/ 100 PY) p-value HR (95% CI) ELIXA1 (lixisenatide) LEADER*2 (liraglutide) SUSTAIN-6*3 (inj. semaglutide) EXSCEL4 (exenatide) Harmony Outcomes5 (albiglutide) 67/3034 (2.2) 1.0 60/3034 (2.0) 0.9 1.12 (0.79, 1.58) 0.54 159/4668 (3.4) 0.9 1.0 177/4672 (3.8) 0.89 (0.72, 1.11) 0.30 27/1648 (1.6) 0.80 44/1649 (2.7) 1.31 0.61 (0.38, 0.99) 0.04 187/7356 (2.5) 0.8 218/7396 (2.9) 0.9 0.85 (0.70, 1.03) NR 94/4731 (2) 1.25 108/4732 (2) 1.45 0.86 (0.66, 1.14) 0.300 REWIND*6 (dulaglutide) 135/4949 (2.7) 0.52 175/4952 (3.5) 0.69 0.76 (0.61, 0.95) 0.017 PIONEER 6*7 (oral semaglutide) AMPLITUDE-O8 (efpeglenatide) 12/1591 (0.8) 0.6 16/1592 (1.0) 0.8 0.74 (0.35, 1.57) NR 47/2717 (1.7) 1.0 31/1359 (2.3) 1.3 0.74 (0.47, 1.17) NR 0.25 0.5 1 2 Favours study drug Favours placebo Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care9 are presented *Non-fatal stroke only; Nominal p-value; p-value not reported in publication IR, incidence rate; NR, not reported; PY, patient-years See slide notes for full list of references 26
MI in completed GLP-1 receptor agonist CVOTs in patients with T2D Study drug Placebo IR IR n with event/ N analysed (%) n with event/ N analysed (%) (events/ 100 PY) (events/ 100 PY) p-value HR (95% CI) ELIXA1 (lixisenatide) LEADER*2 (liraglutide) SUSTAIN-6*3 (inj. semaglutide) EXSCEL4 (exenatide) Harmony Outcomes5 (albiglutide) 270/3034 (8.9) 4.2 261/3034 (8.6) 4.1 1.03 (0.87, 1.22) 0.71 1.6 1.9 281/4668 (6.0) 317/4672 (6.8) 0.88 (0.75, 1.03) 0.11 47/1648 (2.9) 1.40 64/1649 (3.9) 1.92 0.74 (0.51, 1.08) 0.12 483/7356 (6.6) 2.1 493/7396 (6.7) 2.1 0.97 (0.85, 1.10) NR 181/4731 (4) 2.43 240/4732 (5) 3.26 0.75 (0.61, 0.90) 0.003 REWIND*6 (dulaglutide) 205/4949 (4.1) 0.80 212/4952 (4.3) 0.84 0.96 (0.79, 1.16) 0.65 PIONEER 6*7 (oral semaglutide) AMPLITUDE-O8 (efpeglenatide) 37/1591 (2.3) 1.8 31/1592 (1.9) 1.5 1.18 (0.73, 1.90) NR 91/2717 (3.3) 1.9 58/1359 (4.3) 2.4 0.75 (0.54, 1.05) NR 0.25 0.5 1 2 Favours study drug Favours placebo Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care9 are presented *Non-fatal MI only; p-value not reported in publication; Nominal p-value IR, incidence rate; NR, not reported; PY, patient-years See slide notes for full list of references 27
All-cause mortality in completed GLP-1 receptor agonist CVOTs in patients with T2D Study drug Placebo IR IR n with event/ N analysed (%) n with event/ N analysed (%) (events/ 100 PY) (events/ 100 PY) p-value HR (95% CI) ELIXA1 (lixisenatide) LEADER2 (liraglutide) SUSTAIN-63 (inj. semaglutide) EXSCEL4 (exenatide) Harmony Outcomes5 (albiglutide) 211/3034 (7.0) 3.1 223/3034 (7.4) 3.3 0.94 (0.78, 1.13) 0.50 381/4668 (8.2) 2.1 447/4672 (9.6) 2.5 0.85 (0.74, 0.97) 0.02* 62/1648 (3.8) 1.82 60/1649 (3.6) 1.76 1.05 (0.74, 1.50) 0.79 507/7356 (6.9) 2.0 584/7396 (7.9) 2.3 0.86 (0.77, 0.97) NR 196/4731 (4) 2.44 205/4732 (4) 2.56 0.95 (0.79, 1.16) 0.644 REWIND6 (dulaglutide) 536/4949 (10.8) 2.06 592/4952 (12.0) 2.29 0.90 (0.80, 1.01) 0.067 PIONEER 67 (oral semaglutide) AMPLITUDE-O8 (efpeglenatide) 23/1591 (1.4) 1.1 45/1592 (2.8) 2.2 0.51 (0.31, 0.84) NR 111/2717 (4.1) 2.2 69/1359 (5.1) 2.8 0.78 (0.58, 1.06) NR 0.25 0.5 1 2 Favours study drug Favours placebo Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care9 are presented *Nominal p-value; p-value not reported in publication IR, incidence rate; NR, not reported; PY, patient-years See slide notes for full list of references 28
HHF in completed GLP-1 receptor agonist CVOTs in patients with T2D Study drug Placebo IR IR n with event/ N analysed (%) n with event/ N analysed (%) (events/ 100 PY) (events/ 100 PY) p-value HR (95% CI) ELIXA1 (lixisenatide) 122/3034 (4.0) 1.8 127/3034 (4.2) 1.9 0.96 (0.75, 1.23) 0.75 LEADER2 (liraglutide) 218/4668 (4.7) 1.2 248/4672 (5.3) 1.4 0.87 (0.73, 1.05) 0.14 SUSTAIN-63 (inj. semaglutide) 59/1648 (3.6) 1.8 54/1649 (3.3) 1.6 1.11 (0.77, 1.61) 0.57 EXSCEL4 (exenatide) 219/7356 (3.0) 0.9 231/7396 (3.1) 1.0 0.94 (0.78, 1.13) NR* Harmony Outcomes 5 (albiglutide) 188/4731 (4) 218/4732 (5) 0.85 (0.70, 1.04) 0.113 2.49 2.92 REWIND 6 (dulaglutide) 213/4949 (4.3) 0.83 226/4952 (4.6) 0.89 0.93 (0.77, 1.12) 0.46 PIONEER 67 (oral semaglutide) 21/1591 (1.3) 1.0 24/1592 (1.5) 1.2 0.86 (0.48, 1.55) NR* 0.25 0.5 1 2 Favours study drug Favours placebo Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care9 are presented *p-value not reported in publication; CV death or HHF was a composite secondary endpoint; HHF data alone were not reported in the primary publication5; HHF or urgent visit See slide notes for abbreviations and full list of references 29
Kidney outcomes in patients with T2D: LEADER and SUSTAIN-6 Study drug Placebo IR n with event/ N analysed (%) n with event/ N analysed (%) IR (events/ 100 PY) p-value (events/ 100 PY) HR (95% CI) Composite kidney outcome New onset of persistent macroalbuminuria Persistent doubling of serum creatinine 268/4668 (5.7) 1.50 337/4672 (7.2) 1.90 0.78 (0.67, 0.92) 0.003* LEADER1 (liraglutide) 161/4668 (3.4) 0.90 215/4672 (4.6) 1.21 0.74 (0.60, 0.91) 0.004* 97/4672 (2.1) 0.55 87/4668 (1.9) 0.49 0.89 (0.67, 1.19) 0.43 ESKD 64/4672 (1.4) 0.36 56/4668 (1.2) 0.31 0.87 (0.61, 1.24) 0.44 Death due to kidney disease Composite kidney outcome Persistent macroalbuminuria Persistent doubling of serum creatinine Need for continuous RRT 5/4672 (0.1) 0.03 8/4668 (0.2) 0.04 1.59 (0.52, 4.87) 0.41 62/1648 (3.8) 1.86 100/1649 (6.1) 3.06 0.64 (0.46, 0.88) 0.005* SUSTAIN-62 (inj. semaglutide) 44/1648 (2.7) 1.31 81/1649 (4.9) 2.47 0.54 (0.37, 0.77) 0.001* 18/1648 (1.1) 0.53 14/1649 (0.8) 0.41 1.28 (0.64, 2.58) 0.48 11/1648 (0.7) 0.32 12/1649 (0.7) 0.35 0.91 (0.40, 2.07) 0.83 0.25 0.5 1 2 4 Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care3 are presented *Nominal p-value; With eGFR <45 ml/min/1.73 m2; Described as new or worsening nephropathy; With CrCl <45 ml/min/1.73 m2 (MDRD). See slide notes for abbreviations 1. Mann JFE et al. N Engl J Med 2017;377:839; 2. Marso SP et al. N Engl J Med 2016;375:1834; 3. American Diabetes Association. Diabetes Care 2022;45:S1 Favours study drug Favours placebo 30
Kidney outcomes in patients with T2D: REWIND and AMPLITUDE-O Placebo Study drug n with event/ N analysed (%) Rate/ 100 PY n with event/ N analysed (%) Rate/ 100 PY p-value HR (95% CI) 848/4949 (17.1) 3.47 970/4952 (19.6) 4.07 Composite kidney outcome 0.85 (0.77, 0.93) 0.0004* REWIND*1 (dulaglutide) New macroalbuminuria Sustained decline of 30% in eGFR 441/4949 (8.9) 1.76 561/4952 (11.3) 2.29 0.77 (0.68, 0.87) <0.0001* 453/4949 (9.2) 1.79 500/4952 (10.1) 2.00 0.89 (0.78, 1.01) 0.066 Chronic kidney replacement therapy 16/4949 (0.3) 0.06 21/4952 (0.4) 0.08 0.75 (0.39, 1.44) 0.39 Serious kidney AE Composite kidney outcome with sustained decline of 40% in eGFR Composite kidney outcome with sustained decline of 50% in eGFR 84/4949 (1.7) 0.32 93/4952 (1.9) 0.36 0.90 (0.67, 1.20) 0.46 587/4949 (11.9) 2.36 751/4952 (15.2) 3.10 0.76 (0.68, 0.84) <0.0001* 496/4949 (10.0) 1.99 649/4952 (13.1) 2.66 0.74 (0.66, 0.84) <0.0001* Composite kidney outcome event** 353/2717 (13.0) 7.7 250/1359 (18.4) 11.6 0.68 (0.57, 0.79) <0.001 AMPLITUDE-O2 (efpeglenatide) New macroalbuminuria Composite kidney-function outcome with sustained decline of 40% in eGFR 348/2717 (12.8) 7.6 244/1359 (18.0) 11.3 0.68 (0.58, 0.80) NR 121/2717 (4.5) 2.5 76/1359 (5.6) 3.1 0.77 (0.57, 1.02) 0.07 0.25 0.5 1 2 4 Favours study drug Favours placebo Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care3 are presented *Nominal p-value; UACR >33.9 mg/mmol in patients with lower baseline concentration; Requiring dialysis or kidney transplantation; Sensitivity analyses; Exploratory outcome; **UACR >33.9 mg/mmol plus 30% increase in UACR from baseline, decrease in eGFR of 40% for 30 days, renal-replacement therapy for 90 days, and eGFR of <15 ml/min/1.73 m2 for 30 days; Decrease in eGFR of 40% for 30 days, end-stage kidney disease (dialysis for 90 days, kidney transplantation, or eGFR of <15 ml/min/1.73 m2for 30 days), or death from any cause; Exploratory outcome AE, adverse event; NR, not reported; PY, patient-years 1. Gerstein HC et al. Lancet 2019;394:131; 2. Gerstein HC et al. N Engl J Med 2021;385:896; 3. American Diabetes Association. Diabetes Care 2022;45:S1 31
Retinopathy outcomes in completed GLP-1 receptor agonist CVOTs in patients with T2D Study drug Placebo IR IR n with event/ N analysed (%) n with event/ N analysed (%) (events/ 100 PY) (events/ 100 PY) p-value HR (95% CI) LEADER1 (liraglutide) SUSTAIN-6*2 (inj. semaglutide) EXSCEL3 (exenatide) Harmony Outcomes4 (albiglutide) 106/4668 (2.3) 0.6 92/4672 (2.0) 0.5 1.15 (0.87, 1.52) 0.33 50/1648 (3.0) 1.49 29/1649 (1.8) 0.86 1.76 (1.11, 2.78) 0.02 214/7344 (2.9) 238/7389 (3.2) NR NR 78/4717 (2.0) 89/4715 (2.0) 0.88 (0.65, 1.18) NR REWIND 5 (dulaglutide) 95/4949 (1.9) 0.37 76/4952 (1.5) 0.30 1.24 (0.92, 1.68) 0.16 PIONEER 66 (oral semaglutide) AMPLITUDE-O7 (efpeglenatide) 113/1591 (7.1) 6.0 101/1592 (6.3) 5.0 NR NR 47/2717 (1.7) 27/1359 (2.0) NR 0.50 0.25 0.5 1 2 4 Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care8 are presented *Retinopathy complications include vitreous haemorrhage, onset of diabetes-related blindness, and the need for treatment with an intravitreal agent or retinal photocoagulation; Retinopathy outcomes were listed as adverse events, hence no p-values were reported; p-value not reported in publication; Photocoagulation, anti-VEGF therapy or vitrectomy See slide notes for abbreviations and full list of references Favours study drug Favours placebo 32
Overview of selected AEs from completed GLP-1 receptor agonist CVOTs in patients with T2D Harmony Outcomes5 ELIXA1 LEADER2 SUSTAIN-63 EXSCEL4 REWIND6 PIONEER 67 AMPLITUDE-O8 Oral Placebo (n=3032) Lixisenatide (n=3031) Placebo (n=4672) Liraglutide (n=4668) Placebo (n=1649) Semaglutide (n=1648) Placebo (n=7372) Exenatide (n=7344) Placebo (n=4715) Albiglutide (n=4717) Placebo (n=4952) Dulaglutide (n=4949) Placebo (n=1592) Placebo (n=1359) Efpeglenatide (n=2717) semaglutide (n=1591) Serious AEs 22.1 20.6 50.4 49.7 38.0 34.3 16.6 16.8 21.7 19.8 22.5 18.9 AEs leading to discontinuation 7.2 11.4 7.3 9.5 6.7 13.0 1.4* 1.5* 3.8 3.0 6.3 9.1 6.5 11.6 3.6 5.4 Severe hypoglycaemia 0.8 0.3 3.3 2.4 21.2 22.4 3.0 3.4 1 1 1.5 1.3 0.8 1.4 1.0 0.9 Retinopathy 0.4* 0.3* 2.0 2.3 1.8 3.0 3.2 2.9 2 2 6.3 7.1 2.0 1.7 GI conditions 2.7* 2.2* 1.9 3.1 35.4 51.5 3.9 6.0 2* 2* 2.4* 2.4* 1.6 6.8 1.8** 3.3** 0.2 0.1 0.5 0.4 Pancreatitis 0.3 0.2 0.5 0.4 0.7 0.5 0.3 0.4 <1 <1 0.3 0.5 Neoplasms 2.0* 2.4* 9.1 9.9 8.4 9.4 4.9 4.8 7.0 7.1 3.0 2.6 2.7 2.6 Pancreatic cancer 0.3 0.1 0.1 0.3 0.2 0.1 0.2 0.2 <1 <1 0.2 0.4 0.2 <0.1 Thyroid cancer <0.1 0.1 0.1 <0.1 0 0 0.1 0.1 0 0.1 0 0 Medullary thyroid cancer*** <0.1 0 0 0 <0.1 <0.1 0 0 0 0 0 <0.1 Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care9 are presented All data are n (%) of patients. *Reported as serious AEs; Reported as eye events; Reported as a secondary outcome; Acute gallstone disease; Leading to treatment discontinuation; **Reported as severe GI events; Adjudicated acute pancreatitis; Adjudicated as possible or definite pancreatitis by a treatment-blind committee; Based on the first occurrence of acute pancreatitis; Adjudicated, excluding malignant thyroid neoplasms; ***Of total thyroid cancers; Reported as thyroid C-cell neoplasm. See slide notes for abbreviations and full list of references 33
CVOTs with GLP-1 receptor agonists Treatment options for T2D including recent therapeutic classes Completed GLP-1 receptor agonist CVOTs Study design of GLP-1 receptor agonist CVOTs Results of completed GLP-1 receptor agonist CVOTs Summary
GLP-1 receptor agonist CVOTs: summary Liraglutide, dulaglutide and efpeglenatide were the only agents to achieve superiority for the primary outcome*1 7 The majority of patients treated with liraglutide and efpeglenatide had established CV disease; the majority of patients treated with dulaglutide had multiple risk factors for CV disease2,5,7 Lixisenatide, injectable and oral semaglutide, and exenatide met non-inferiority for the primary outcome1,3,4,6 Primary endpoint Differences in CV and mortality outcomes were observed across the class:1 7 The rate of CV death or death from any cause was lower for liraglutide and oral semaglutide vs placebo; this was not noted with other GLP-1 receptor agonists Inference of mortality benefit with oral semaglutide is not possible as PIONEER 6 was designed to rule out an upper limit of the 95% CI of the HR 1.86 Available data suggest there is no effect on heart failure outcomes for any GLP-1 receptor agonist1 7 Other CV outcomes Microvascular outcomes Liraglutide, injectable semaglutide, dulaglutide and efpeglenatide reduced the risk of a composite kidney outcome, driven by a reduction in new macroalbuminuria3,7 9 High of gastrointestinal AEs and retinopathy AEs were observed with most GLP-1 receptor agonists. There was no increased risk of pancreatic AEs or neoplasms1 7 Safety Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology *Testing for superiority was not prespecified in SUSTAIN-6, although injectable semaglutide demonstrated a 26% RRR for 3P-MACE; Exploratory outcome See slide notes for abbreviations and full list of references 35
MACE outcomes in completed SGLT2 inhibitor and GLP-1 receptor agonist CVOTs in patients with T2D Drug class Trial (study drug) HR (95% CI) 0.86 (0.74, 0.99) SGLT2 inhibitor EMPA-REG OUTCOME1 (empagliflozin) 0.86 (0.75, 0.97) CANVAS Program2 (canagliflozin) DECLARE-TIMI 583 (dapagliflozin) 0.93 (0.84, 1.03) VERTIS CV4 (ertugliflozin) 0.97 (0.85, 1.11) ELIXA5 (lixisenatide) GLP-1 RA 1.02 (0.89, 1.17) LEADER6 (liraglutide) 0.87 (0.78, 0.97) SUSTAIN-67 (inj. semaglutide) 0.74 (0.58, 0.95) PIONEER 6*8 (oral semaglutide) 0.79 (0.57, 1.11) EXSCEL9 (exenatide) 0.91 (0.83, 1.00) Harmony Outcomes10 (albiglutide) 0.78 (0.68, 0.90) REWIND*11 (dulaglutide) 0.88 (0.79, 0.99) AMPLITUDE-O*12 (efpeglenatide) 0.73 (0.58, 0.92) Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care13 are presented ELIXA data are for 4P-MACE, all other data are for 3P-MACE *3P-MACE includes death from unknown causes; 95.6% CI See slide notes for full list of references 0.5 1 2 Favours study drug Favours placebo 37
HHF outcomes in completed SGLT2 inhibitor and GLP-1 receptor agonist CVOTs in patients with T2D Drug class Trial (study drug) HR (95% CI) SGLT2 inhibitor EMPA-REG OUTCOME1 (empagliflozin) 0.65 (0.50, 0.85) CANVAS Program2 (canagliflozin) 0.67 (0.52, 0.87) DECLARE-TIMI 583 (dapagliflozin) 0.73 (0.61, 0.88) VERTIS CV4 (ertugliflozin) 0.70 (0.54, 0.90) ELIXA5 (lixisenatide) GLP-1 RA 0.96 (0.75, 1.23) LEADER6 (liraglutide) 0.87 (0.73, 1.05) SUSTAIN-67 (inj. semaglutide) 1.11 (0.77, 1.61) PIONEER 68 (oral semaglutide) 0.86 (0.48, 1.55) EXSCEL9 (exenatide) 0.94 (0.78, 1.13) Harmony Outcomes*10 (albiglutide) 0.85 (0.70, 1.04) REWIND 11 (dulaglutide) 0.93 (0.77, 1.12) 0.25 0.5 1 2 Favours study drug Favours placebo Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care12 are presented *CV death or HHF; HHF data alone were not reported in the primary publication; Hospital admission for HF or urgent visit See slide notes for abbreviations and full list of references 38
CV death outcomes in completed SGLT2 inhibitor and GLP-1 receptor agonist CVOTs in patients with T2D Drug class Trial (study drug) HR (95% CI) 0.62 (0.49, 0.77) SGLT2 inhibitor EMPA-REG OUTCOME1 (empagliflozin) 0.87 (0.72, 1.06) CANVAS Program2 (canagliflozin) 0.98 (0.82, 1.17) DECLARE-TIMI 583 (dapagliflozin) 0.92 (0.77, 1.11) VERTIS CV4 (ertugliflozin) ELIXA5 (lixisenatide) GLP-1 RA 0.98 (0.78, 1.22) LEADER6 (liraglutide) 0.78 (0.66, 0.93) SUSTAIN-67 (inj. semaglutide) 0.98 (0.65, 1.48) PIONEER 68 (oral semaglutide) 0.49 (0.27, 0.92) EXSCEL 9 (exenatide) 0.88 (0.76, 1.02) Harmony Outcomes10 (albiglutide) 0.93 (0.73, 1.19) REWIND*11 (dulaglutide) 0.91 (0.78, 1.06) AMPLITUDE-O12 (efpeglenatide) 0.72 (0.50, 1.03) Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Empagliflozin is FDA approved to reduce the risk of CV death Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care13 are presented *Includes death from unknown cause; 95.8% CI See slide notes for full list of references 0.25 0.5 1 2 Favours study drug Favours placebo 39
Composite kidney outcomes in SGLT2 inhibitor and GLP-1 receptor agonist CVOTs and cardiorenal trials in patients with T2D Patients Events Weights (%)1 HR (95% CI) HR (95% CI) SGLT2 inhibitor* 1 6185 913 EMPA-REG OUTCOME (empagliflozin)2 0.61 (0.53, 0.70) 24.9 10,142 847 CANVAS Program (canagliflozin)3 25.0 0.57 (0.50, 0.66) 17,160 365 DECLARE-TIMI 58 (dapagliflozin)4 50.1 0.53 (0.43, 0.66) 4401 585 CREDENCE (canagliflozin)5 0.70 (0.59, 0.82) GLP-1 RA* 1 6063 3751 ELIXA (lixisenatide)6 20.0 0.84 (0.68, 1.02) 9340 605 LEADER (liraglutide)7 32.2 0.78 (0.67, 0.92) 3297 162 SUSTAIN-6 (inj. semaglutide)8 7.7 0.64 (0.46, 0.88) 14,752 773 EXSCEL (exenatide)9 40.1 0.88 (0.76, 1.01) 9901 1818 REWIND (dulaglutide)10 0.85 (0.77, 0.93) 0.25 0.5 1 2 Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care11 are presented p-value for subgroup differences between SGLT2 inhibitors and GLP-1 receptor agonists was 0.01 *Composite kidney outcomes were defined differently across trials. See slide notes for endpoints; Q statistic=2.99; p=0.22, I2=33.2% (excluding CREDENCE); Q statistic=3.60; p=0.31, I2=16.6%(excluding REWIND) See slide notes for full list of references Favours study drug Favours placebo 40
Hard kidney outcomes in SGLT2 inhibitor, GLP-1 receptor agonist and DPP-4 inhibitor CVOTs and cardiorenal trials in patients with T2D Patients Events Weights (%)1 HR (95% CI) HR (95% CI) SGLT2 inhibitor* 1 6968 152 EMPA-REG OUTCOME (empagliflozin)2 20.9 0.54 (0.40, 0.75) 10,142 249 CANVAS Program (canagliflozin)3 34.0 0.60 (0.47, 0.77) 17,160 365 DECLARE-TIMI 58 (dapagliflozin)4 45.1 0.53 (0.43, 0.66) 8246 283 VERTIS CV (ertugliflozin)5 0.81 (0.63, 1.04)** 4401 377 CREDENCE (canagliflozin)6 0.66 (0.53, 0.81) GLP-1 RA* 1 6063 76 ELIXA (lixisenatide)7 9.5 1.16 (0.74, 1.83) 9340 184 LEADER (liraglutide)8 23.4 0.89 (0.67, 1.19) 3297 162 SUSTAIN-6 (inj. semaglutide)9 4.0 0.64 (0.46, 0.88) 12,925 519 EXSCEL (exenatide)10 63.1 0.88 (0.74, 1.05) DPP-4 inhibitor 16,492 372 SAVOR-TIMI 53 (saxagliptin) 11 1.08 (0.88, 1.32) 6979 633 CARMELINA (linagliptin) 12 1.04 (0.89, 1.22) 0.25 0.5 1 2 Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care13 are presented p-value for subgroup differences between SGLT2 inhibitors and GLP-1 receptor agonists was <0.001 *Hard kidney outcomes were defined differently across trials. See slide notes for endpoints; Q statistic=0.59; p=0.74, I2=0% (excluding CREDENCE); Q statistic=2.18; p=0.54, I2=0%; Doubling of serum creatinine, initiation of dialysis, renal transplantation or creatinine >6.0 mg/dl; Sustained ESKD, sustained 40% decrease in eGFR from baseline or death due to kidney disease; **95.8% CI See slide notes for full list of references Favours study drug Favours placebo 41
Hard kidney outcomes and albuminuria in completed CV, cardiorenal and HF trials in patients with T2D Hard kidney outcomes* BENEFIT NEUTRAL HARM BENEFIT Empagliflozin (EMPA-REG OUTCOME1) Canagliflozin (CANVAS,2 CREDENCE3) Dapagliflozin (DECLARE-TIMI 58,4 DAPA-HF5) LEADER (liraglutide)6 SUSTAIN-6 (inj. semaglutide)7 REWIND (dulaglutide)8 CARMELINA (linagliptin)9 Albuminuria NEUTRAL EXSCEL (exenatide)10 SAVOR-TIMI 53 (saxagliptin)11 HARM SGLT2 inhibitor GLP-1 RA DPP-4 inhibitor Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Canagliflozin is FDA approved to reduce the risk of end-stage kidney disease, doubling of serum creatinine, CV death and HHF in adults with T2D and diabetic nephropathy with albuminuria Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care12 are presented *Exploratory outcomes in all trials except for CREDENCE; hard kidney outcomes were most commonly doubling of serum creatinine or need for chronic dialysis, end-stage kidney disease, and death due to kidney causes; In CREDENCE, patients were required to have CKD, defined as eGFR 30 to <90 ml/min/1.73 m2 and albuminuria; the primary composite outcome was end-stage kidney disease, sustained doubling of serum creatinine, or death due to kidney causes or CV death3 See slide notes for abbreviations and full list of references 42
Evidence from CVOTs has shown that some glucose-lowering therapies have beneficial effects on CV outcomes MACE BENEFIT NEUTRAL HARM BENEFIT EMPA-REG OUTCOME (empagliflozin)1 CANVAS Program and CREDENCE (canagliflozin)2,3 DECLARE-TIMI 58 (dapagliflozin)4 VERTIS CV (ertugliflozin)5 ELIXA (lixisenatide)10 EXSCEL (once-weekly exenatide)11 PIONEER 6 (oral semaglutide)12 EXAMINE (alogliptin)13 TECOS (sitagliptin)14 CARMELINA (linagliptin)15 HHF* LEADER (liraglutide)6 SUSTAIN-6 (inj. semaglutide)7 Harmony Outcomes (albiglutide) 8 REWIND (dulaglutide) 9 NEUTRAL HARM SAVOR-TIMI 53 (saxagliptin)16 SGLT2 inhibitor GLP-1 RA DPP-4 inhibitor Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Empagliflozin is FDA approved to reduce the risk of CV death Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care17 are presented AMPLITUDE-O achieved 3P-MACE but did not evaluate HHF, therefore the study was not included in this comparison18 *Exploratory outcomes; CV death or HHF was a composite secondary endpoint; HHF data alone were not reported in the primary publication; HF outcome was hospital admission for HF or urgent visit See slide notes for abbreviations and full list of references 43
Overview of CV outcomes from GLP-1 receptor agonist CVOTs in patients with T2D (1/4) Study drug n with event/N analysed (%) Placebo Trial (study drug) p-value* Outcome HR (95% CI) 4P-MACE 406/3034 (13.4) 399/3034 (13.2) 1.02 (0.89, 1.17) 0.81 ELIXA1 (lixisenatide) CV death 156/3034 (5.1) 158/3034 (5.2) 0.98 (0.78, 1.22) 0.85 Fatal or non-fatal MI 270/3034 (8.9) 261/3034 (8.6) 1.03 (0.87, 1.22) 0.71 Fatal or non-fatal stroke 67/3034 (2.2) 60/3034 (2.0) 1.12 (0.79, 1.58) 0.54 Unstable angina 11/3034 (0.2) 10/3034 (0.1) 1.11 (0.47, 2.62) 0.81 HHF 122/3034 (4.0) 127/3034 (4.2) 0.96 (0.75, 1.23) 0.75 All-cause mortality 211/3034 (7.0) 223/3034 (7.4) 0.94 (0.78, 1.13) 0.50 3P-MACE 608/4668 (13.0) 694/4672 (14.9) 0.87 (0.78, 0.97) 0.01 LEADER2 (liraglutide) CV death 219/4668 (4.7) 278/4672 (6.0) 0.78 (0.66, 0.93) 0.007 Non-fatal MI 281/4668 (6.0) 317/4672 (6.8) 0.88 (0.75, 1.03) 0.11 Non-fatal stroke 159/4668 (3.4) 177/4672 (3.8) 0.89 (0.72, 1.11) 0.30 HHF 218/4668 (4.7) 248/4672 (5.3) 0.87 (0.73, 1.05) 0.14 All-cause mortality 381/4668 (8.2) 447/4672 (9.6) 0.85 (0.74, 0.97) 0.02 0.25 1 4 Favours study drug Favours placebo Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care3 are presented *Only p-values for 3P/4P-MACE are for superiority. Both trials showed significance for non-inferiority regarding the primary endpoint; Nominal p-value See slide notes for abbreviations 1. Pfeffer MA et al. N Engl J Med 2015;373:2247; 2. Marso SP et al. N Engl J Med 2016;375:311; 3. American Diabetes Association. Diabetes Care 2022;45:S1 44
Overview of CV outcomes from GLP-1 receptor agonist CVOTs in patients with T2D (2/4) Study drug n with event/N analysed (%) Placebo Trial (study drug) p-value* Outcome HR (95% CI) SUSTAIN-61 (injectable semaglutide) 3P-MACE 108/1648 (6.6) 146/1649 (8.9) 0.74 (0.58, 0.95) 0.02 CV death 44/1648 (2.7) 46/1649 (2.8) 0.98 (0.65, 1.48) 0.92 Non-fatal MI 47/1648 (2.9) 64/1649 (3.9) 0.74 (0.51, 1.08) 0.12 Non-fatal stroke 27/1648 (1.6) 44/1649 (2.7) 0.61 (0.38, 0.99) 0.04 HHF 59/1648 (3.6) 54/1649 (3.3) 1.11 (0.77, 1.61) 0.57 All-cause mortality 62/1648 (3.8) 60/1649 (3.6) 1.05 (0.74, 1.50) 0.79 EXSCEL2,3 (exenatide) 3P-MACE 839/7356 (11.4) 905/7396 (12.2) 0.91 (0.83, 1.00) 0.06 CV death 340/7356 (4.6) 383/7396 (5.2) 0.88 (0.76, 1.02) NR Fatal or non-fatal MI 483/7356 (6.6) 493/7396 (6.7) 0.97 (0.85, 1.10) NR Fatal or non-fatal stroke 187/7356 (2.5) 218/7396 (2.9) 0.85 (0.70, 1.03) NR HHF 219/7356 (3.0) 231/7396 (3.1) 0.94 (0.78, 1.13) NR All-cause mortality 507/7356 (6.9) 584/7396 (7.9) 0.86 (0.77, 0.97) NR 0.25 1 4 Favours study drug Favours placebo Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the ADA 2022 Standards of Care4 are presented *Only p-values for 3P-MACE are for superiority. Both trials showed significance for non-inferiority regarding the primary endpoint; Nominal p-value; p-value not reported in publication See slide notes for abbreviations 1. Marso SP et al. N Engl J Med 2016;375:1834; 2. Holman RR et al. N Engl J Med 2017;377:1228; 3. Kristensen SL et al. Lancet Diabetes Endocrinol 2019;7:776; 4. American Diabetes Association. Diabetes Care 2022;45:S1 45
Overview of CV outcomes from GLP-1 receptor agonist CVOTs in patients with T2D (3/4) Study drug n with event/N analysed (%) Placebo Trial (study drug) p-value* Outcome HR (95% CI) Harmony Outcomes1 (albiglutide) 3P-MACE 338/4731 (7) 428/4732 (9) 0.78 (0.68, 0.90) 0.0006 4P-MACE 373/4731 (8) 468/4732 (10) 0.78 (0.69, 0.90) 0.0005 CV death 122/4731 (3) 130/4732 (3) 0.93 (0.73, 1.19) 0.578 Fatal or non-fatal MI 181/4731 (4) 240/4732 (5) 0.75 (0.61, 0.90) 0.003 Fatal or non-fatal stroke 94/4731 (2) 108/4732 (2) 0.86 (0.66, 1.14) 0.300 CV death or HHF 188/4731 (4) 218/4732 (5) 0.85 (0.70, 1.04) 0.113 All-cause mortality 196/4731 (4) 205/4732 (4) 0.95 (0.79, 1.16) 0.644 REWIND2 (dulaglutide) 3P-MACE 594/4949 (12.0) 663/4952 (13.4) 0.88 (0.79, 0.99) 0.026 CV death 317/4949 (6.4) 346/4952 (7.0) 0.91 (0.78, 1.06) 0.21 Non-fatal MI 205/4949 (4.1) 212/4952 (4.3) 0.96 (0.79, 1.16) 0.65 Non-fatal stroke 135/4949 (2.7) 175/4952 (3.5) 0.76 (0.61, 0.95) 0.017 All-cause mortality 536/4949 (10.8) 592/4952 (12.0) 0.90 (0.80, 1.01) 0.06 HHF or urgent visit 213/4949 (4.3) 226/4952 (4.6) 0.93 (0.77, 1.12) 0.46 HUA 88/4949 (1.8) 77/4952 (1.6) 1.14 (0.84, 1.54) 0.41 0.25 1 4 Favours study drug Favours placebo Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care3 are presented *Only p-values for 3P-MACE are for superiority; Nominal p-value See slide notes for abbreviations 1. Hernandez AF et al. Lancet 2018;392:1519; 2. Gerstein HC et al. Lancet 2019;394:121; 3. American Diabetes Association. Diabetes Care 2022;45:S1 46
Overview of CV outcomes from GLP-1 receptor agonist CVOTs in patients with T2D (4/4) Study drug n with event/N analysed (%) Placebo Trial (study drug) p-value Outcome HR (95% CI) 3P-MACE Expanded composite outcome CV death 61/1591 (3.8) 76/1592 (4.8) 0.79 (0.57, 1.11) 0.17* PIONEER 61 (oral semaglutide) 83/1591 (5.2) 100/1592 (6.3) 0.82 (0.61, 1.10) NR 15/1591 (0.9) 30/1592 (1.9) 0.49 (0.27, 0.92) NR Non-fatal MI 37/1591 (2.3) 31/1591 (1.9) 1.18 (0.73, 1.90) NR Non-fatal stroke 12/1591 (0.8) 16/1592 (1.0) 0.74 (0.35, 1.57) NR HHF 21/1591 (1.3) 24/1592 (1.5) 0.86 (0.48, 1.55) NR All-cause mortality 23/1591 (1.4) 45/1592 (2.8) 0.51 (0.31, 0.84) NR 3P-MACE 189/2717 (7.0) 125/1359 (9.2) 0.73 (0.58, 0.92) 0.007 AMPLITUDE-O2 (efpeglenatide) CV death 75/2717 (2.8) 50/1359 (3.7) 0.72 (0.50, 1.03) NR Non-fatal MI 85/2717 (3.1) 53/1359 (3.9) 0.78 (0.55, 1.10) NR Non-fatal stroke 41/2717 (1.5) 25/1359 (1.8) 0.80 (0.48, 1.31) NR All-cause mortality 111/2717 (4.1) 69/1359 (5.1) 0.78 (0.58, 1.06) NR 0.25 1 4 Favours study drug Favours placebo Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Only GLP-1 receptor agonists included in the 2022 ADA Standards of Care3 are presented *p-value for superiority. The trial showed significance for non-inferiority regarding the primary endpoint; CV death, non-fatal MI, non-fatal stroke, HUA or HHF; p-value not reported in publication. See slide notes for abbreviations 1. Husain M et al. N Engl J Med 2019;381:841; 2. Gerstein HC et al. N Engl J Med 2021;385:896; 3. American Diabetes Association. Diabetes Care 2022;45:S1 47