Behavioral Health Alliance of Montana: Advocating for Behavioral Health Providers and Clients

Formed in 2017 by the Montana Healthcare Foundation, the Behavioral Health Alliance of Montana serves as a unified voice for advocacy on behalf of behavioral health providers and clients in the Central Service Area Authority. With a focus on supporting adult and children's mental health, substance use disorder, and Tribal behavioral health, the organization represents over 40 state-approved Medicaid agencies. Despite facing budget cuts in January 2018, the Alliance has been working diligently to rebuild and enhance programs, including targeted case management, treatment services, and community support initiatives for individuals across Montana.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Behavioral Health Alliance of Montana Central Service Area Authority 2021 Annual Congress Mary Windecker
Formed in 2017 by the Montana Healthcare Foundation to provide one voice for advocacy for behavioral health providers and clients. We re an independent non-profit and our members are Behavioral Health providers who treat adult or children mental health, substance use disorder or Tribal behavioral health. Over 40 state-approved Medicaid agencies across the state.
$49.5M Cuts in January 2018 to community- Based programs in behavioral health Programs recreated since July 2018 2.99% cut to all Medicaid Providers 2.99% Reinstated to Medicaid Providers 50% cut to Children s Targeted Case Management Taskforce implemented new model with $15.90/15 min unit paid for 80% of kids. Prior to 2018, it was $19.48/15 min unit. 2018-2020 the rate was $8.45/15 min unit. Budget Cuts in Budget Cuts in January 2018 January 2018 and program and program work since then. work since then. 58% cut to Adult Targeted Case Management Adult CM rate not raised but new Adult Continuum of Care Program implemented with PACT, ImPACT Residential, and Community Maintenance Program. Intensive Outpatient Substance Use Disorder (SUD) Treatment Cuts Implemented new rates for Intensive Outpatient SUD with enhanced bundled rates. SUD Assessment Rate Cuts No change Children s Home Support Services Cut Rate came back as $18.50/unit. This is too low to provide care for the acute and/or rural families in this program. Most providers will not reestablish HSS. Room and Board for Therapeutic Children s Homes Cut No change Numerous cuts to people living with disabilities programs No change 4
AMDD Presentation to CFHHS 9/22/2021 https://leg.mt.gov/content/Committees/Interim/2021-2022/Children-Families/Studies/SJR-14/sept2021-ammd-powerpoint.pdf 5
Program of Assertive Community Treatment (PACT) is provided in urban counties in Montana. It is a multi-disciplinary, self-contained clinical team approach providing long-term intensive care and all mental health services in natural community settings to Medicaid members. Interventions focus on achieving maximum reduction of physical and mental disability and restoration of the member s best possible functional level. PACT, MACT and CMP PACT, MACT and CMP Levels of Community Levels of Community Care Care Community Maintenance Program (CMP) is a step-down service provided by the larger PACT team for those clients who have improved and need less intensive care. Typically includes case management an Montana Assertive Community Treatment (MACT) is intended to provide a smaller team in rural counties and is intended to provide medication and community support for members who require long- term, ongoing support to be maintained successfully in the community and remain out of higher levels of care for members who can successfully reside outside of a structured setting. 6
AMDD PACT/MACT REGIONS 7
Central Services Area Authority Counties: Blaine, Broadwater, Cascade, Chouteau, Gallatin, Glacier, Hill, Jefferson, Lewis & Clark, Liberty, Meagher, Park, Pondera, Teton, and Toole. 8
Dramatic increase in substance abuse and mental illness due to financial instability, job loss, housing concerns, etc. Behavioral Health wasn t immediately recognized in MT as essential health care so not FEMA funding was available. COVID-19 PANDEMIC DPHHS relaxed rules around telehealth, pre-authorizations and other administrative regulations to allow for quicker treatment. Federal relief focused on lost expenses not increased costs so was of limited use to behavioral health agencies. DPHHS reimbursed behavioral health providers for Personal Protective Equipment (PPE) costs. 9
Shodair has 74 beds for children and adolescents; only 30 beds can currently be staffed due to worker shortages. Shodair currently has a waiting list of 66 kids. Yellowstone Boys & Girls Ranch receives 110 referrals a month; they can only accept up to 10 kids per month at most. AWARE, due to staff shortages, has closed three children s homes, and has consolidated day services for an additional two therapeutic group homes and four developmental disability residences. Intermountain has closed one children s home due to an inability to staff the home. Youth Dynamics has 80 beds in 10 group homes and are at a full census and there is a current waiting list of 46 children. They have referrals for over 130 community children in need of services that are awaiting assessments to be performed. Rimrock has an adult substance use residential home closed due to staff shortages, with a waiting list of 6-8 weeks for residential homes that are in operation. Youth Homes is at capacity and is seeing dramatic increases in referrals from State agencies to accept children who are denied admission to higher levels of care due to lack of capacity. 10
Use 10% Federal Match increase for provider rate increases. Offer stipends for daycare for employees in Medicaid state-approved agencies who earn between 185-250% of Federal Poverty Level. Offer stipends for housing for employees in the same criteria. Increase payments to PRTF and TGH providers to keep kids in-state. Offer loan repayments and tuition incentives for employees in the above criteria. Set up SNAP-eligible rapid retraining for direct care workers. Create a career ladder for Behavioral Health Paraprofessionals that can be certified and work toward Medicaid reimbursement for the certification. Developed Quality Database for benchmarking outcome tracking tools. Behavioral Health Workforce Crisis 11
The SDMI Case Management Waiver contract was held by Summit over the past several years. There were many difficulties with case management, so AMDD put out a Request for Proposal. AWARE received the contract award for non- conflict Case Management for the SDMI Waiver Members in July. DPHHS has not yet signed the contract with AWARE, so transition has been difficult. The CFHHS Committee asked that the contract be signed within the next two weeks at the latest. SDMI Case Management Contract 13
DPHHS Reorganization 14
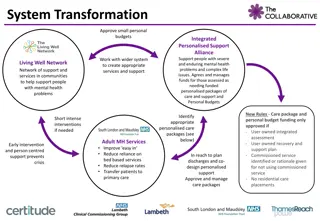
Create a level reimbursement playing field for behavioral health within the health care ecosystem. Long-Term Behavioral Health System Transformation in Montana 1. Vet Certified Community Behavioral Health Centers (CCBHCs) for Montana. 2. Vet Prospective Payment System (PPS) reimbursement system for Montana. 3. Must consider Managed Care . 4. ?????? 15
Follow Childrens and Family Health and Human Services Committee during the interim: The Committee oversees DPHHS and are doing studies on the adult and children s mental health system. Follow the DPHHS provider rate study. Get involved with vetting potential systems. Follow the legislature when it s in session. Partner with, NAMI, MACO, BHAM, MACDS, and Disability Rights to carry a common message. Action Steps for SAAs 16





 is")