Alarming Malnutrition Situation in India: National Nutrition Policy and Strategies
 undefined
undefined
MAHARSHI DAYANAND SARASWATI
UNIVERSITY AJMER
E- CONTENT LEARNING LECTURE
COMMUNITY NUTRITION
NATIONAL NUTRITION POLICIES
DR. NAMITA S. MOYAL
DEPARTMENT OF FOOD SCIENCE AND
NUTRITION



National Nutrition Policy
•
The need for a National Nutrition Policy is implicit in both the paramountcy of
nutrition in development as well as in the complexity of the problem.
•
This general problem of under-nutrition should be
se
en as a part of a larger set of
processes that produces and consumes agricultural commodities on farms, trans
f
orms
them into food in the marketing sector and sells the food, to customen to satisfy
nutritional, aes
t
hetic and social needs.
•
Within this set, there are three sub-sets of issues, within the broad sectors of
agriculture, food and nutrition, with various linkages among them. In fact, the third
subset, viz. Nutrition, is the net- result of the other two subsets.
•
It is both possible as well as necessary to devise policy interventions for influencing
the working of these sets and thereby improving the nutritional status of the society.
The nature of linkages determine the fate of such interventions.

•
Malnutrition is a serious problem in India. The statistics regarding malnutrition is appalling.
•
The National Nutrition Strategy was released by the NITI Aayog in 2017.
•
The strategy talked about the negative impact of malnutrition on the productivity of the
population, and its contribution to the mortality rates.
•
It laid out objectives for the country to achieve in reducing malnutrition rates.
•
Malnutrition
•
Malnutrition in children implies that they are either too short or too thin according to their
age.
•
Stunting: Stunting indicates a child’s height is lower than the average for his/her age.
•
Wasting: Wasting indicates a child’s weight is lower than the average for his/her height.
•
Underweight: An underweight child’s weight is lower than the average for his/her age.
•
Malnutrition in India
•
As per data given by the UNICEF, India was at the 10th spot
among countries with the highest number of underweight children,
and at the 17th spot for the highest number of stunted children in
the world.
•
Malnutrition adversely impacts children’s chances of survival,
enhances their susceptibility to illness, decreases their ability to
learn, and causes them to be less productive in life later on.
•
Malnutrition is also estimated to be a contributing factor in 1/3rd
of all deaths of kids below the age of five years.
•
The graph below shows the rate of malnutrition in India for kids
under the age of 5:
R
ate of malnutrition in India for kids under the age of 5:
•
Although the rates of underweight and stunting have improved, there has been
an increase in wasting rates.
•
The prevalence of underweight children was found to be more in rural areas
than urban areas.
•
For 19% of the kids born in India, the national average birth weight is under 2.5
Kg. This is a worrying figure because according to the WHO, newborns weighing
under 2.5 Kg are twenty times more likely to die than heavier babies.
•
In addition, more than half of the children in the country are anaemic, implying
an insufficient amount of haemoglobin in the blood. This is caused by a
nutritional deficiency of iron and other essential minerals, and vitamins in the
body.
•
Another trend observed in India is that malnutrition is observed not only in
children, but also in adults. About 20% of men and 23% women in India are
considered undernourished.
•
However, 19% of men and 21% of women are obese.
The major nutrition problems of India
(1) Under-nutrition resulting in:
(a) Protein Energy Malnutrition (PEM);
(b) Iron deficie ncy;
(c) Iodine deficiency
(d)Vitamin deficiency.
(e) Low Birth Weight Q'Iildren;
•
(2) Seasonal dimensions of Nutrition;
•
(3) Natu ral calamities & the landless.
•
(4) Market Distortion and Disinformation;
•
(5) urbanisation.
•
(6) Special Nutritional Problems of Hill People, Industrial Workers, Migrant Work,ers, and other
special categories;
•
(7) Problems of Overn utrition, overweight and I')besity for a small section of urban population.
The Existing Policy Instruments for combating Mal
n
utrition:-
•
Till the end of the IV PIan. India's main emphasis was on the aggregate growth of
the economy and reliance was placed on the percolation effects of growth. In the
face of continuing poverty and malnutrition. an alternative strategy of
development c
o
mprising a frontal attacK on poverty, unemployment and
malnutrition became a national priority from the begining of'the V
p
Ian.
•
This shift in strategy has given rise to a number of interventions to increase the
purchasing power of the poor, to improve the provision of basic services to the
poor and to' devise a security system threugh which the most vulnerable sections
of the poor (viz. women and children) can be protected
•
The Strategy also includes steps to augment maternal nutrition and care such as:
•
Supplementary nutritional support during pregnancy and breastfeeding period
•
Nutrition and health counselling
•
Sufficient intake of iodised salt and screening for severe anaemia
•
Institutional childbirth, lactation management and better postnatal care
•
The Strategy also envisages some reforms in the governance aspects such as:
•
Convergence of district and state implementation plans for ICDS, NHM
and Swachh Bharat
•
Focus on the most vulnerable communities in districts with the highest levels of
child malnutrition
•
Service delivery models based on evidence of impact
Nutrition P
olic
y Instruments:
•
.
The Strategy: Nutrition is a multi-sectoral issue and needs to
be tackled at various levels. Nutrition affects development as
much as development affects nutrition. It is therefore. important
to tackle the problem of nutrition both through direct nutrition
intervention for specially vulnerable groups as well as through
various development policy instruments which will create
conditions for improved nutrition.
A
.Direct Int
e
rvent
i
on-Short Term
•
Nutrition Intervention for specially vulnerable
group
•
Fortification of Essential FoocIs:- Essential food items shall be fortified with
appropriate nutrients. for example, salt with iodine and/or iron.
•
Popularlsation of Low Cost Nutritious Food:- Efforts to produ
ce a
nd popularise
lo
wcost nutritious foods from indigenous and locally available raw material
shall be intensified. It is necessary to involve women particularly in this
activity
.
•
Control of Micro-Nutrient Defi
ciencies
amongst vulnerable Groups:-
•
Deficiencies of Vi
tamin
A, iron and folic acid and iodine among children.
pregnant women and nursing mothers sh
ou
l
d
be controlled through intensified
programmes. Iron supplementation to adolescent girls shall be introduced. The
programme shall be expanded to cover alle ligible members of the community.
Indirect Pol
ic
y Instruments: Long Term Ins
t
itutional & Structural
Changes:-
•
(i)
Food Security
: In order to ensure aggregate food sccurity. a per capita availability of 215
kg/person/year of foodgrains needs to be attained.
•
Improving the purchasing power: Poverty alleviation programmes, like the Integrated Rural
Development Programme (IRDP) and employment generation schemes like Jawahar Rozgar
Yojana, Nehru Rozgar Yojana and DWCRA are to be re-oriented and restructured to make a
forceful dent on the purchasi~g power of the lowest economic segments of the population.
•
In all poverty alleviation programmes nutritional objectives shall be incorporat
e
d explicitly
and the nutritional benefits of income gene
rati
on shall be taken for granted Existing
programmes shall be scrutinized for their nutrition component.
•
It is necessary to improve the purchasing power of the landless and the rural and urban poor
by implemen'ting employment generation programmes so that additional employment of at
least 100 days is created for each rural landless family and employment opportunities are
created in urban areas for slum dwellers and the urban poor.
•
(
ii
) Publi
c
Distribution System:
Ensuring an equitable food
distribution, through the expansi
o
n of the public-distribution
system. The Public distribution system shall ensure availability
of essential food artich:s. such a
s
coarse grains, pulses and
Jaggery, beside'! rice. wheat. sugar and oil; conveniently and at
reasonable prices to the public. particularly to those living
below the poverty line
n
ot only in urban areas but throughout
the country.
F
or this pur
po
se encouragement shall be given to
the consumer cooperatives and fair price shops shall be opened
in adequate number in all areas.
•
(iii)
Land Reforms:
•
(iv)
Health & Family Welfare
•
(v)
Basic Health and Nutrition Knowledge:
Basic health and. nutrition
knowledge with special focus on wholesome infant feeding practices,
shall be imparted to the people extensively and effectively.
•
Nutrition and health education concepts shall be effectively integrated
into the school curricula, as' well as into
all n
utrition programmes.
Nutrition and Health Education are very important in th
e
context of the
problems of Overnutrition also.
•
(vii) Prevention of Food A
d
ulteration:
Prevention of food adulteration must be
strengthened by gearing up the enforcement machinery.
•
(viii)Nutrition Su
rv
e
ill
ance:
Nutritio
na
l surveillance is another weak area requiring
immediate attention. The NNMB NIN of ICMR is to be strengthened so that
periodical monitoring of the nutritional status of children. adolescent girls, and
pregnant and lactating mothers below the poverty tine takes place through
representative samples and results are transmitted to all agencie
s
concerned.
•
The NNMB should not only try and assess the impact of ongoing nutrition and
development programmes but also serve as an Early Warning System for initiating
prompt action.
•
(xi) Equal Remuneration:
Special efforts should be made to improve the effectiveness of
progr"mmes related to women. The wagesof women shall be at par with that of men in order
to improve women's economic status. This requires a stricter enforcement of the Equal
Remuneration
a
ct. Special emphasis will have to be given for expanding employment
opportunities for women.
•
(xii) CommunIcation:
Communication through established media is one
o
f the most
important strategies to be adopted for the effective implementation of the Nutrition Policy. The
Department of Women,and Child Development will have a well-established, permanent
Communications Division. with adequate staff and fund support.
•
While using the communication tools both mass communication as well as group or inter-
personal communication should be used. Not only the electronic media but also folk and print
media should be used extensively
•
Monitoring of Nutrition Programmes:
Monitoring of Nutrition
Programmes (viz ICDS), and of Nutrition Education a
n
d Demonstration
by the Food & Nutrition Board, through all its 67 centres & field units,
should be continued.
•
Research:
.Research into various aspects of nutrition, both on the
consumption side as well as the supply side, is another essential aspect of
the strategy. Research must accurately identify those who are suffering
fr
o
m various degrees of malnutrition.
•
Research should enable selection of new varieties of food with high
nutrition value which can be within the purchasing power of the poor.
National Nutrition Strategy Objectives
•
Vision:
To achieve Kuposhan Mukt Bharat (malnutrition free India) by
2022.
•
Focus:
To prevent and reduce undernutrition across the lifecycle as early
as possible, particularly in the first 3 years of life.
•
Goals:
The Strategy envisions to contribute to major national
development goals for a more inclusive growth, like the reduction of
infant, maternal and infant mortality through the achievement of the
following targets:
•
1.Decrease in the rate of underweight children below 5 years to 20.7% by
2022. (Current rate is 35.7%)
•
2.Decrease in the prevalence of anemia in kids (6 – 59 months) to 19.5%
by 2022. (Current rate is 58.4%)
•
3.Decrease in the prevalence of anemia in women and girls (15 – 49
years) to 17.7% by 2022. (Current rate is 53.1%)
•
As a long term goal, the purpose of the National Nutrition Strategy is to
progressively reduce all forms of undernutrition by 2030.
•
Micronutrient supplements and twice a year deworming for children
•
The Strategy also includes steps to augment maternal nutrition and care such as:
•
Supplementary nutritional support during pregnancy and breastfeeding period
•
Nutrition and health counselling
•
Sufficient intake of iodised salt and screening for severe anaemia
•
Institutional childbirth, lactation management and better postnatal care
•
The Strategy also envisages some reforms in the governance aspects such as:
•
Convergence of district and state implementation plans for ICDS, NHM
•
and Swachh Bharat
•
Focus on the most vulnerable communities in districts with the highest levels
•
of child malnutritions
•
Service delivery models based on evidence of impact
National Nutrition Strategy Other Details
•
The POSHAN Abhiyaan (National Nutrition Mission) is being implemented as part of the
Strategy with the aim of ensuring a malnutrition free India by 2022. The key objective of this
Abhiyaan is to reduce stunting in children by improving usage of key Anganwadi services.
•
The Strategy envisions certain interventions such as:
•
Encouragement of breastfeeding for the first 6 months after birth
•
Universal access to young and infant child care (including Integrated Child Development
Services [ICDS] and crèches)
•
Enhanced care, referrals and management of severely undernourished and sick children
•
Twice yearly vitamin A supplements for children between the ages of 9 months and 5 years
•
V
I
S
I
O
N
2
0
2
2
•
The National Nutrition Strategy is committed to ensuring that
every child, adolescent girl and woman attains optimal
nutritional status- especially those from the most vulnerable
communities.
•
The focus is on preventing and reducing undernutrition across
the life cycle- as early as possible, especially in the first three
years of life. This commitment also builds on the recognition
that the first few years of life are forever - the foundation for
ensuring optimum physical growth, development, cognition and
cumulative lifelong learning.
•
The Vision - “Kuposhan Mukt Bharat”
•
Free from malnutrition, across the life cycle.
•
This is elaborated as –
•
“Healthy, optimally nourished children, realizing their growth and development
potential, active learning capacity and adult productivity;
•
Healthy, optimally nourished women realizing their social and economic
development potential;
•
In protective, nurturing, gender sensitive and inclusive community environments –
That enhance human and national development in the present - and in the future.
.
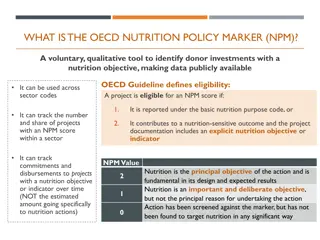
GOALS, OBJECTIVES & KEY INDICATORS
•
It is widely recognized that Maternal and Child Undernutrition is the underlying
cause of nearly half(4 5%) of the mortality of children under five years ( Black RE
et al, The LANCET 2013) and that one fifth of maternal mortality can be averted
by addressing maternal stunting and iron deficiency anemia (LANCET 2008).
•
The link between the vicious cycle of undernutrition, disease/infections and
mortality has also been highlighted in the Nutrition Situation Analysis.
•
In this perspective, the National Nutrition Strategy will therefore contribute to key
national development goals for more inclusive growth, such as the reduction of
maternal, infant and young child mortality, through its focus on the following
monitorable targets-
•
- To prevent and reduce undernutrition (underweight prevalence) in children (0- 3
years) by 3
percentage points per annum from NFHS 4 levels by 2022.
•
- To reduce the prevalence of anemia among young children, adolescent girls and
women in the reproductive age group (15- 49 years) by one third of NFHS 4 levels
by 2022.
•
The achievement of the above monitorable targets will contribute to improved
learning outcomes in elementary education, improved adult productivity, women’s
empowerment and gender equality and the National Development Agenda.
Achievement of these national development goals will also significantly shape
progress towards global sustainable development goals.
•
In a longer term perspective, the strategy will also aim to progressively reduce all
forms of undernutrition by 2030. The focus of this strategy over the next five years
is on preventing and reducing child undernutrition.
•
While undernutrition affects large segments of the population – the strategy accords
priority to and focus on the most vulnerable and critical age groups, which also
determine nutrition in later life and inter generationally.
Monitorable Outcomes
•
Monitorable Outcomes Current status Target 2022 Means of verification
•
1. Reduction in % age of underweight (Below-2SD) children below 5 years 35.7
20.7 NFHS
•
2. Reduction in prevalence of anemia in children (6-59 months). 58.4 19.5 -do-
•
3. Reduction in prevalence of anemia in women and girls (15-49 years). 53.1 17.7 -
do-
•
The above goals will also contribute significantly to shaping the achievement of
global Sustainable Development Goals related to ending hunger, achieving food
security and improved nutrition, ending poverty, ensuring healthy lives, ensuring
inclusive and equitable quality education, achieving gender equality and
empowering women and girls. At least 12 of the 17 Sustainable Development Goals
contain indicators that are relevant for nutrition, demonstrating that nutrition is the
foundation for ensuring
sustainable development.
•
This will also contribute to achieving global nutrition targets endorsed in 2012, through the
World Health Assembly Resolution 65.6, committing to a comprehensive implementation
plan on maternal, infant and young child nutrition.
•
This specified a set of six global nutrition targets for 2025 that aim to:
•
– Achieve a 40% reduction in the number of children under-5 who are stunted;
•
– Achieve a 50% reduction of anemia in women of reproductive age;
•
– Achieve a 30% reduction in low birth weight;
•
– Ensure that there is no increase in childhood overweight;
•
– Increase the rate of exclusive breastfeeding in the first 6 months up to at least 50%;
•
– Reduce and maintain childhood wasting to less than 5%.
GUIDING PRINCIPLES
•
The implementation of the National Nutrition Strategy will be
guided by the following key principles of action-
A LIFE CYCLE APPROACH
•
Recognizing that there is an intergenerational cycle of
undernutrition, as described in the situation analysis, a life
cycle approach will be adopted, with a focus on critical
periods of nutritional vulnerability and opportunity for
enhancing human development potential.
EARLY PREVENTIVE ACTION
•
Recognizing that growth and development deficits that
compromise child health and survival and achievement of
optimal learning outcomes are cumulative and largely
irreversible – there will be emphasis on preventing under
nutrition, as early as possible, across the life cycle.
INCLUSIVE AND GENDER SENSITIVE
•
It will be rooted in a rights based framework that seeks to
promote the rights of women and children to survival,
development, protection and participation – without
discrimination. In this, strategies for ensuring social inclusion of
marginalized community groups will be pursued- recognizing
that nutritional vulnerability is compounded by multiple
deprivations - based on socio economic status, high burden of
disease, natural factors such as floods/droughts and/or other
conditions such as lack of access to services. Efforts will focus
on reaching the most vulnerable and deprived.
COMMUNITY EMPOWERMENT AND OWNERSHIP
•
Families and communities will be enabled for improved care
behaviors and nutrition of children and women, to demand
quality services, to contribute to increased service utilization
and to participate in community based monitoring.
VALUING, RECOGNIZING AND ENHANCING THE CONTRIBUTION OF
ANGANWADI WORKERS HELPERS AND ASHAS
•
The approach will be to improve the working conditions, skills, development
pathways and motivatio n ofAnganwadi workers, helpers and also ASHAs - a
frontline team of over 33 lakh women from the local community covering 13.42
lakh habitations across the country– recognizing that they are prime movers of social
change.
DECENTRALIZATION AND FLEXIBILITY
•
Contextually relevant, decentralized approaches will be promoted, with greater
flexibility at State, distric tand local levels for greater and sustained programme
effectiveness and impact, in harmony with the approach of cooperative federalism.
This will also enable utilization of opportunities provided by the recommendations
of the Fourteenth Finance Commission with greater devolution of resources to
States- mobilizing and catalyzing state resources and action for Nutrition.
OWNERSHIP OF PANCHAYATI RAJ INSTITUTIONS AND URBAN LOCAL
BODIES
•
Strengthening the ownership of Panchayati Raj Institutions and urban local bodies is a
key principle – to ensure that local self governments own, promote, monitor and sustain
nutrition initiatives – effecting convergence of action at the grass roots. This is essential
as the subjects allocated in the 73rd Amendment include those addressing the immediate
and underlying determinants of undernutrition such as Health and Sanitation, Family
Welfare, Drinking Water, Women and Child Development, Public Distribution Systems,
Agriculture, Education, Poverty Alleviation and Social Welfare, among others. This is
even more relevant in the light of the Fourteenth Finance Commission
Recommendations.
FOSTER INNOVATION
•
Innovation will be encouraged and recognized - including through quality circles which
encourage a cluster of frontline teams to identify best practices and replicate the same –
with a ripple effect and widening of the innovation. Best practices will be identified and
local adaptation and replication or scaling up encouraged.
INFORMED BY SCIENCE AND EVIDENCE
Programme strategies will be evidence based, informed by the state of the science (as
well as by the state of the practice) and updated as new evidence emerges related to
nutrition, health and development.
ENSURE THAT THERE IS NO CONFLICT OF INTEREST
An underlying principle of action is that policy development and programme
implementation must be transparent, open to public scrutiny and kept free from conflict
of interest, with requisite safeguards.
(This includes ensuring that representation on policy, technical advisory groups and
various management committees at different levels is free from conflict of interest.)
Nutrition Interventions
• Infant and Young Child Care and Nutrition
• Infant and Young Child Health
• Maternal Care, Nutrition and Health
• Adolescent Care, Nutrition and Health
• Addressing Micronutrient Deficiencies -including Anemia
• Community Nutrition (Interventions addressing the community)
Infant and Young Child Care and Nutrition
•
These interventions will focus on children under 3 years, through the promotion of -
•
• Universal early initiation (within 1 hour of birth) and exclusive breastfeeding for
the first six months of life.
•
• Universal timely and appropriate complementary feeding after six months, along
with
•
continued breastfeeding for two years or beyond.
•
• Universal growth monitoring and promotion of young children-using WHO CGS
with counseling of mothers/families using the Mother Child Protection Card.
•
• Universal access to infant and young child care (including ICDS, crèches,
linkages with MGNREGA), with improved supplementary nutritional support/THR
through ICDS.
•
• Enhanced care, improved feeding during and after illness, nutritional support,
referrals and management of severely and acutely undernourished and/or sick
children.
Infant and Young Child Health
•
The set of interventions related to Infant and Young Child Health therefore
envisage the promotion of-
•
• Improved new born care and care of low birth weight babies.
•
• Bi annual vitamin A supplementation for children 9-59 months
•
Universal, timely and complete immunization of infants against vaccine
preventable diseases (and subsequent booster doses) with quality assurance.
•
• Ensuring that young children receive micronutrient supplementation and bi
annual deworming as per MHFW guidelines. This includes-
•
• IFA supplementation for children 6-59 months.
•
• Bi annual deworming for children Over 1 year-59 months (linked to bi annual
VAS rounds).
•
• Prevention and management of common neonatal and childhood illnesses such
as diarrhoea (with ORS and zinc supplementation) and Acute Respiratory
Infections (ARI) and severe acute malnutrition, at community and facility levels.
Maternal Care, Health and Nutrition
•
Interventions for maternal care, health and nutrition therefore include the promotion
of-
•
• Improved supplementary nutritional support during pregnancy and lactation
(ICDS).
•
• Improved antenatal care - including health and nutrition counseling (also family
support for extra diet and rest to ensure adequate weight gain), IFA supplementation,
consumption of adequately iodized salt and screening /management of severe
anemia.
•
• Enhanced maternity protection (through the effective implementation of PMMVY)
•
• Institutional deliveries, lactation management, improved post-natal and new born
care.
•
• Promoting marriage at the right age, first pregnancy at the right age, inter
pregnancy recoupment/ birth spacing and shared care/ parenting responsibilities.
•
• Promoting Women’s Literacy and Empowerment.
Adolescent Nutrition
•
The interventions here - especially for improving the nutrition status of adolescent
girls- will focus on the promotion of-
•
• Equal care of the girl child at different stages of the life cycle- linked to the Beti
Bachao Beti Padhao initiative.
•
• Improved access to health care, counseling support through school health
programmes, ARSH and deworming as per MHFW National Deworming Initiative.
•
• Improved access to nutritional support through Mid-Day Meals in schools
(MHRD) and through SABLA for out of school girls.
•
• Universal access of girls in school and girls out of school to IFA supplementation.
•
• Girls’ education, skill development and female literacy.
•
• Changing gender constructs -Gender sensitization and life skills for adolescents.
•
• No Child Marriage- Marriage of young women after the age of 18 years.
Community Nutrition
•
These interventions include, among others-
•
• Ensuring universal access to safe drinking water, sanitation and hygiene, in an open
defecation free environment, through Swachh Bharat.
•
• Prevention and treatment for malaria through the –
•
- Use of bed-nets and/or intermittent preventive therapy for malaria (as per MHFW
protocols) in malaria-endemic areas - Facilitating mosquito control measures.
•
Other relevant health /disease control measures specific for the state/district, relevant
for improving nutrition at community levels - such as JE, kala azar etc.
•
• Ensuring access to household food security, social protection systems and safety nets.
•
• Nutrition Education to ensure that optimal feeding and caring practices, dietary
diversity
,
nutritious foods; sanitation and hygiene and healthy lifestyles
Core Strategies - “HOW”
•
• Governance Reform- Nutrition Centre Stage and Public Accountability
•
• Leading by Example- Kuposhan Mukt States, districts and panchayats.
•
• Convergence- of State/ District Implementation Plans for ICDS, NHM and Swachh Bharat and others,
addressing different determinants of undernutrition together.
•
• Prioritize Action- Reaching the most vulnerable communities in the districts/blocks with the
•
highest levels of child undernutrition.
•
• Counseling to Reach the Critical Age Group- pregnant and lactating mothers, and children under 3
years, through skilled counselors, peer counselors and support groups.
•
• Continuum of care- across the life-cycle that includes preventive, promotive and curative care, linking
families, communities, AWCs, health centers and health facilities.
•
• Innovative Service Delivery Models- demonstration and ripple effect, with evidence of impact.
•
• Community Based Monitoring- Making undernutrition visible to families, communities, Enabling
Actions- Implementing innovative components of ICDS Restructuring; Crèches through MGNREGA;
Extending SABLA and implementing Maternity Benifits through Pradhan Mantri Matru Vandana Yojana
and Strengthening Nutrition within the Health System tracking and informed action.
TRACKING & RECOGNIZING PROGRESS
•
The new Nutrition Monitoring System will enable tracking of progress at different levels and
identification of states/ districts/blocks/ AWCs that are performing well and those that are lagging
behind, using lead indicators and tools such as dashboards and score cards, with wide dissemination
of the same, including display on the relevant websites of the Ministry/State government
department/district.
•
This will be reviewed regularly by the proposed NNM Mission Steering Groups at National/ state
levels and by NNM District Committees, with corrective actions suggested.
•
NATIONAL NUTRITION SURVEILLANCE SYSTEM
•
A National Nutrition Surveillance System should be set up, building on previous experience in states
such as Andhra Pradesh. This will include an early warning system for increase in nutritional
vulnerabilities, through assessment and analysis with trigger points for timely corrective action,
through
•
development programmes and safety nets. The use of sentinel sites will be pursued
and multiple vulnerabilities tracked such as those related to socio-economic
deprivation, agrarian distress, seasonal migration, distress, seasonal migration,
disruptions in access to services, lack of access to social protection measures, disease
outbreaks, endemic disease areas, natural disasters etc.
•
Mapping of undernourished endemic zones of the country in terms of identifying
‘high risk and vulnerable districts’ for the rest of districts, cases of severe
undernutrition in children should be included in the routine disease reporting system.
•
The surveillance system will also enable epidemiological investigation of
‘malnutrition clusters’ and traditional endemic zones, using verbal autopsy to
determine the underlying causes of deaths, besides the immediate cause.
•
The nutrition surveillance system will be GIS (Geographic Information System)
based for tracking severely undernourished children, families and communities in the
long run. This will not only ensure child-wise tracking, appropriate care, feeding and
medical interventions for severely undernourished children- but also help link the
families of severely undernourished children with social protection measures, food
security measures and to access employment through MGNREGA/ other livelihood
options.
•
As required, linkages will also be established with the National Integrated Disease
Surveillance System, as a significant proportion of under 5 child deaths reflect the
vicious cycle of severe undernutrition and disease/infections. The design of the
proposed National Nutrition Surveillance System will be developed subsequently by
the National Nutrition Mission, with support from National Institute of Nutrition.
R
E
S
E
A
R
C
H
&
E
V
A
L
U
A
T
I
O
N
NUTRITION SURVEY
The Nutrition Strategy will use a systematic population sample
based survey to assess baseline, mid term and final evaluation of
Nutrition outcomes and overall progress of the key monitorable
targets, nutrition outcomes, related nutrition and health process
indicators.
This will include anthropometric indices as related to maternal
and child nutrition, as well as assessment of anemia prevalence.
Data from service providers (ICDS, NHM) will be used for
regular programmatic monitoring for improved programme
effectiveness and efficiency.
•
ESTIMATED RESOURCE REQUIREMENT
•
It may be assumed that the Strategy will be implemented using resources of the major
flagship programmes involved - NHM, ICDS, Swachh Bharat and resources earmarked for
the upcoming National Nutrition Mission (including ICT enabled monitoring and a Nutrition
Surveillance System).
•
The increased provision of 25 % of flexi funds for States in Centrally sponsored schemes and
the enhanced resources devolved to States, panchayats and urban local bodies would also be
catalyzed for the purpose.
•
Additional resources would be needed for flexible responses at district level (as in MP), local
innovation, gap filling and incentivisation of good performance.
THANK YOU
Malnutrition remains a serious issue in India, with high rates of underweight, stunting, and wasting among children. The National Nutrition Policy emphasizes the need for a comprehensive approach to address the complexities of malnutrition. Despite some improvements, malnutrition continues to impact children's health, learning abilities, and overall productivity. Policy interventions and strategies are crucial to improve the nutritional status of the population and reduce mortality rates associated with malnutrition.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
MAHARSHI DAYANAND SARASWATI UNIVERSITY AJMER E- CONTENT LEARNING LECTURE COMMUNITY NUTRITION NATIONAL NUTRITION POLICIES DR. NAMITA S. MOYAL DEPARTMENT OF FOOD SCIENCE AND NUTRITION
National Nutrition Policy The need for a National Nutrition Policy is implicit in both the paramountcy of nutrition in development as well as in the complexity of the problem. This general problem of under-nutrition should be seen as a part of a larger set of processes that produces and consumes agricultural commodities on farms, transforms them into food in the marketing sector and sells the food, to customen to satisfy nutritional, aesthetic and social needs. Within this set, there are three sub-sets of issues, within the broad sectors of agriculture, food and nutrition, with various linkages among them. In fact, the third subset, viz. Nutrition, is the net- result of the other two subsets. It is both possible as well as necessary to devise policy interventions for influencing the working of these sets and thereby improving the nutritional status of the society. The nature of linkages determine the fate of such interventions.
Malnutrition is a serious problem in India. The statistics regarding malnutrition is appalling. The National Nutrition Strategy was released by the NITI Aayog in 2017. The strategy talked about the negative impact of malnutrition on the productivity of the population, and its contribution to the mortality rates. It laid out objectives for the country to achieve in reducing malnutrition rates. Malnutrition Malnutrition in children implies that they are either too short or too thin according to their age. Stunting: Stunting indicates a child s height is lower than the average for his/her age. Wasting: Wasting indicates a child s weight is lower than the average for his/her height. Underweight: An underweight child s weight is lower than the average for his/her age.
Malnutrition in India As per data given by the UNICEF, India was at the 10th spot among countries with the highest number of underweight children, and at the 17th spot for the highest number of stunted children in the world. Malnutrition adversely impacts children s chances of survival, enhances their susceptibility to illness, decreases their ability to learn, and causes them to be less productive in life later on. Malnutrition is also estimated to be a contributing factor in 1/3rd of all deaths of kids below the age of five years. The graph below shows the rate of malnutrition in India for kids under the age of 5:
Although the rates of underweight and stunting have improved, there has been an increase in wasting rates. The prevalence of underweight children was found to be more in rural areas than urban areas. For 19% of the kids born in India, the national average birth weight is under 2.5 Kg. This is a worrying figure because according to the WHO, newborns weighing under 2.5 Kg are twenty times more likely to die than heavier babies. In addition, more than half of the children in the country are anaemic, implying an insufficient amount of haemoglobin in the blood. This is caused by a nutritional deficiency of iron and other essential minerals, and vitamins in the body. Another trend observed in India is that malnutrition is observed not only in children, but also in adults. About 20% of men and 23% women in India are considered undernourished. However, 19% of men and 21% of women are obese.
The major nutrition problems of India (1) Under-nutrition resulting in: (a) Protein Energy Malnutrition (PEM); (b) Iron deficie ncy; (c) Iodine deficiency (d)Vitamin deficiency. (e) Low Birth Weight Q'Iildren; (2) Seasonal dimensions of Nutrition; (3) Natu ral calamities & the landless. (4) Market Distortion and Disinformation; (5) urbanisation. (6) Special Nutritional Problems of Hill People, Industrial Workers, Migrant Work,ers, and other special categories; (7) Problems of Overn utrition, overweight and I')besity for a small section of urban population.
The Existing Policy Instruments for combating Malnutrition:- Till the end of the IV PIan. India's main emphasis was on the aggregate growth of the economy and reliance was placed on the percolation effects of growth. In the face of continuing poverty and malnutrition. an alternative strategy of development comprising a frontal attacK on poverty, unemployment and malnutrition became a national priority from the begining of'the V pIan. This shift in strategy has given rise to a number of interventions to increase the purchasing power of the poor, to improve the provision of basic services to the poor and to' devise a security system threugh which the most vulnerable sections of the poor (viz. women and children) can be protected
The Strategy also includes steps to augment maternal nutrition and care such as: Supplementary nutritional support during pregnancy and breastfeeding period Nutrition and health counselling Sufficient intake of iodised salt and screening for severe anaemia Institutional childbirth, lactation management and better postnatal care The Strategy also envisages some reforms in the governance aspects such as: Convergence of district and state implementation plans for ICDS, NHM and Swachh Bharat Focus on the most vulnerable communities in districts with the highest levels of child malnutrition Service delivery models based on evidence of impact
Nutrition Policy Instruments: .The Strategy: Nutrition is a multi-sectoral issue and needs to be tackled at various levels. Nutrition affects development as much as development affects nutrition. It is therefore. important to tackle the problem of nutrition both through direct nutrition intervention for specially vulnerable groups as well as through various development policy instruments which will create conditions for improved nutrition.
A .Direct Intervention-Short Term Nutrition Intervention for specially vulnerable group Fortification of Essential FoocIs:- Essential food items shall be fortified with appropriate nutrients. for example, salt with iodine and/or iron. Popularlsation of Low Cost Nutritious Food:- Efforts to produce and popularise lowcost nutritious foods from indigenous and locally available raw material shall be intensified. It is necessary to involve women particularly in this activity. Control of Micro-Nutrient Deficiencies amongst vulnerable Groups:- Deficiencies of Vitamin A, iron and folic acid and iodine among children. pregnant women and nursing mothers should be controlled through intensified programmes. Iron supplementation to adolescent girls shall be introduced. The programme shall be expanded to cover alle ligible members of the community.
Indirect Policy Instruments: Long Term Institutional & Structural Changes:- (i) Food Security: In order to ensure aggregate food sccurity. a per capita availability of 215 kg/person/year of foodgrains needs to be attained. Improving the purchasing power: Poverty alleviation programmes, like the Integrated Rural Development Programme (IRDP) and employment generation schemes like Jawahar Rozgar Yojana, Nehru Rozgar Yojana and DWCRA are to be re-oriented and restructured to make a forceful dent on the purchasi~g power of the lowest economic segments of the population. In all poverty alleviation programmes nutritional objectives shall be incorporated explicitly and the nutritional benefits of income generation shall be taken for granted programmes shall be scrutinized for their nutrition component. It is necessary to improve the purchasing power of the landless and the rural and urban poor by implemen'ting employment generation programmes so that additional employment of at least 100 days is created for each rural landless family and employment opportunities are created in urban areas for slum dwellers and the urban poor. Existing
(ii) Public Distribution System: Ensuring an equitable food distribution, through the expansion of the public-distribution system. The Public distribution system shall ensure availability of essential food artich:s. such as coarse grains, pulses and Jaggery, beside'! rice. wheat. sugar and oil; conveniently and at reasonable prices to the public. particularly to those living below the poverty line not only in urban areas but throughout the country.For this purpose encouragement shall be given to the consumer cooperatives and fair price shops shall be opened in adequate number in all areas.
(iii) Land Reforms: (iv) Health & Family Welfare (v) Basic Health and Nutrition Knowledge: Basic health and. nutrition knowledge with special focus on wholesome infant feeding practices, shall be imparted to the people extensively and effectively. Nutrition and health education concepts shall be effectively integrated into the school curricula, as' well as into all nutrition programmes. Nutrition and Health Education are very important in the context of the problems of Overnutrition also.
(vii) Prevention of Food Adulteration: Prevention of food adulteration must be strengthened by gearing up the enforcement machinery. (viii)Nutrition Surveillance: Nutritional surveillance is another weak area requiring immediate attention. The NNMB NIN of ICMR is to be strengthened so that periodical monitoring of the nutritional status of children. adolescent girls, and pregnant and lactating mothers below the poverty tine takes place through representative samples and results are transmitted to all agencies concerned. The NNMB should not only try and assess the impact of ongoing nutrition and development programmes but also serve as an Early Warning System for initiating prompt action.
(xi) Equal Remuneration: Special efforts should be made to improve the effectiveness of progr"mmes related to women. The wagesof women shall be at par with that of men in order to improve women's economic status. This requires a stricter enforcement of the Equal Remuneration act. Special emphasis will have to be given for expanding employment opportunities for women. (xii) CommunIcation: Communication through established media is one of the most important strategies to be adopted for the effective implementation of the Nutrition Policy. The Department of Women,and Child Development will have a well-established, permanent Communications Division. with adequate staff and fund support. While using the communication tools both mass communication as well as group or inter- personal communication should be used. Not only the electronic media but also folk and print media should be used extensively
Monitoring of Nutrition Programmes: Monitoring of Nutrition Programmes (viz ICDS), and of Nutrition Education and Demonstration by the Food & Nutrition Board, through all its 67 centres & field units, should be continued. Research:.Research into various aspects of nutrition, both on the consumption side as well as the supply side, is another essential aspect of the strategy. Research must accurately identify those who are suffering from various degrees of malnutrition. Research should enable selection of new varieties of food with high nutrition value which can be within the purchasing power of the poor.
National Nutrition Strategy Objectives Vision: To achieve Kuposhan Mukt Bharat (malnutrition free India) by 2022. Focus: To prevent and reduce undernutrition across the lifecycle as early as possible, particularly in the first 3 years of life. Goals: The Strategy envisions to contribute to major national development goals for a more inclusive growth, like the reduction of infant, maternal and infant mortality through the achievement of the following targets: 1.Decrease in the rate of underweight children below 5 years to 20.7% by 2022. (Current rate is 35.7%) 2.Decrease in the prevalence of anemia in kids (6 59 months) to 19.5% by 2022. (Current rate is 58.4%) 3.Decrease in the prevalence of anemia in women and girls (15 49 years) to 17.7% by 2022. (Current rate is 53.1%)
Micronutrient supplements and twice a year deworming for children The Strategy also includes steps to augment maternal nutrition and care such as: Supplementary nutritional support during pregnancy and breastfeeding period Nutrition and health counselling Sufficient intake of iodised salt and screening for severe anaemia Institutional childbirth, lactation management and better postnatal care The Strategy also envisages some reforms in the governance aspects such as: Convergence of district and state implementation plans for ICDS, NHM and Swachh Bharat Focus on the most vulnerable communities in districts with the highest levels of child malnutritions Service delivery models based on evidence of impact
National Nutrition Strategy Other Details The POSHAN Abhiyaan (National Nutrition Mission) is being implemented as part of the Strategy with the aim of ensuring a malnutrition free India by 2022. The key objective of this Abhiyaan is to reduce stunting in children by improving usage of keyAnganwadi services. The Strategy envisions certain interventions such as: Encouragement of breastfeeding for the first 6 months after birth Universal access to young and infant child care (including Integrated Child Development Services [ICDS] and cr ches) Enhanced care, referrals and management of severely undernourished and sick children Twice yearly vitamin Asupplements for children between the ages of 9 months and 5 years
VISION 2022 The National Nutrition Strategy is committed to ensuring that every child, adolescent girl and woman attains optimal nutritional status- especially those from the most vulnerable communities. The focus is on preventing and reducing undernutrition across the life cycle- as early as possible, especially in the first three years of life. This commitment also builds on the recognition that the first few years of life are forever - the foundation for ensuring optimum physical growth, development, cognition and cumulative lifelong learning
The Vision - Kuposhan Mukt Bharat Free from malnutrition, across the life cycle. This is elaborated as Healthy, optimally nourished children, realizing their growth and development potential, active learning capacity and adult productivity; Healthy, optimally nourished women development potential; In protective, nurturing, gender sensitive and inclusive community environments That enhance human and national development in the present - and in the future. realizing their social and economic
. GOALS, OBJECTIVES & KEY INDICATORS It is widely recognized that Maternal and Child Undernutrition is the underlying cause of nearly half(4 5%) of the mortality of children under five years ( Black RE et al, The LANCET 2013) and that one fifth of maternal mortality can be averted by addressing maternal stunting and iron deficiency anemia (LANCET 2008). The link between the vicious cycle of undernutrition, disease/infections and mortality has also been highlighted in the Nutrition SituationAnalysis. In this perspective, the National Nutrition Strategy will therefore contribute to key national development goals for more inclusive growth, such as the reduction of maternal, infant and young child mortality, through its focus on the following monitorable targets- - To prevent and reduce undernutrition (underweight prevalence) in children (0- 3 years) by 3percentage points per annum from NFHS 4 levels by 2022.
- To reduce the prevalence of anemia among young children, adolescent girls and women in the reproductive age group (15- 49 years) by one third of NFHS 4 levels by 2022. The achievement of the above monitorable targets will contribute to improved learning outcomes in elementary education, improved adult productivity, women s empowerment and gender equality and the National Development Agenda. Achievement of these national development goals will also significantly shape progress towards global sustainable development goals. In a longer term perspective, the strategy will also aim to progressively reduce all forms of undernutrition by 2030. The focus of this strategy over the next five years is on preventing and reducing child undernutrition. While undernutrition affects large segments of the population the strategy accords priority to and focus on the most vulnerable and critical age groups, which also determine nutrition in later life and inter generationally.
Monitorable Outcomes Monitorable Outcomes Current status Target 2022 Means of verification 1. Reduction in % age of underweight (Below-2SD) children below 5 years 35.7 20.7 NFHS 2. Reduction in prevalence of anemia in children (6-59 months). 58.4 19.5 -do- 3. Reduction in prevalence of anemia in women and girls (15-49 years). 53.1 17.7 - do- The above goals will also contribute significantly to shaping the achievement of global Sustainable Development Goals related to ending hunger, achieving food security and improved nutrition, ending poverty, ensuring healthy lives, ensuring inclusive and equitable quality education, achieving gender equality and empowering women and girls. At least 12 of the 17 Sustainable Development Goals contain indicators that are relevant for nutrition, demonstrating that nutrition is the foundation for ensuring sustainable development.
This will also contribute to achieving global nutrition targets endorsed in 2012, through the World Health Assembly Resolution 65.6, committing to a comprehensive implementation plan on maternal, infant and young child nutrition. This specified a set of six global nutrition targets for 2025 that aim to: Achieve a 40% reduction in the number of children under-5 who are stunted; Achieve a 50% reduction of anemia in women of reproductive age; Achieve a 30% reduction in low birth weight; Ensure that there is no increase in childhood overweight; Increase the rate of exclusive breastfeeding in the first 6 months up to at least 50%; Reduce and maintain childhood wasting to less than 5%.
GUIDING PRINCIPLES The implementation of the National Nutrition Strategy will be guided by the following key principles of action- ALIFE CYCLEAPPROACH Recognizing that there is an intergenerational cycle of undernutrition, as described in the situation analysis, a life cycle approach will be adopted, with a focus on critical periods of nutritional vulnerability and opportunity for enhancing human development potential. EARLY PREVENTIVEACTION Recognizing that growth and development deficits that compromise child health and survival and achievement of
INCLUSIVEAND GENDER SENSITIVE It will be rooted in a rights based framework that seeks to promote the rights of women and children to survival, development, protection and discrimination. In this, strategies for ensuring social inclusion of marginalized community groups will be pursued- recognizing that nutritional vulnerability is compounded by multiple deprivations - based on socio economic status, high burden of disease, natural factors such as floods/droughts and/or other conditions such as lack of access to services. Efforts will focus on reaching the most vulnerable and deprived. COMMUNITY EMPOWERMENTAND OWNERSHIP Families and communities will be enabled for improved care participation without
VALUING, RECOGNIZING AND ENHANCING THE CONTRIBUTION OF ANGANWADI WORKERS HELPERSAND ASHAS The approach will be to improve the working conditions, skills, development pathways and motivatio n ofAnganwadi workers, helpers and also ASHAs - a frontline team of over 33 lakh women from the local community covering 13.42 lakh habitations across the country recognizing that they are prime movers of social change. DECENTRALIZATION AND FLEXIBILITY Contextually relevant, decentralized approaches will be promoted, with greater flexibility at State, distric tand local levels for greater and sustained programme effectiveness and impact, in harmony with the approach of cooperative federalism. This will also enable utilization of opportunities provided by the recommendations of the Fourteenth Finance Commission with greater devolution of resources to States- mobilizing and catalyzing state resources and action for Nutrition.
OWNERSHIP OF PANCHAYATI RAJ INSTITUTIONS AND URBAN LOCAL BODIES Strengthening the ownership of Panchayati Raj Institutions and urban local bodies is a key principle to ensure that local self governments own, promote, monitor and sustain nutrition initiatives effecting convergence of action at the grass roots. This is essential as the subjects allocated in the 73rd Amendment include those addressing the immediate and underlying determinants of undernutrition such as Health and Sanitation, Family Welfare, Drinking Water, Women and Child Development, Public Distribution Systems, Agriculture, Education, Poverty Alleviation and Social Welfare, among others. This is even more relevant in the light of Recommendations. the Fourteenth Finance Commission FOSTER INNOVATION Innovation will be encouraged and recognized - including through quality circles which encourage a cluster of frontline teams to identify best practices and replicate the same with a ripple effect and widening of the innovation. Best practices will be identified and
INFORMED BY SCIENCEAND EVIDENCE Programme strategies will be evidence based, informed by the state of the science (as well as by the state of the practice) and updated as new evidence emerges related to nutrition, health and development. ENSURE THAT THERE IS NO CONFLICT OF INTEREST An underlying principle of action is that policy development and programme implementation must be transparent, open to public scrutiny and kept free from conflict of interest, with requisite safeguards. (This includes ensuring that representation on policy, technical advisory groups and various management committees at different levels is free from conflict of interest.)
Nutrition Interventions Infant and Young Child Care and Nutrition Infant and Young Child Health Maternal Care, Nutrition and Health Adolescent Care, Nutrition and Health Addressing Micronutrient Deficiencies -includingAnemia Community Nutrition (Interventions addressing the community)
Infant and Young Child Care and Nutrition These interventions will focus on children under 3 years, through the promotion of - Universal early initiation (within 1 hour of birth) and exclusive breastfeeding for the first six months of life. Universal timely and appropriate complementary feeding after six months, along with continued breastfeeding for two years or beyond. Universal growth monitoring and promotion of young children-using WHO CGS with counseling of mothers/families using the Mother Child Protection Card. Universal access to infant and young child care (including ICDS, cr ches, linkages with MGNREGA), with improved supplementary nutritional support/THR through ICDS. Enhanced care, improved feeding during and after illness, nutritional support, referrals and management of severely and acutely undernourished and/or sick children.
Infant and Young Child Health The set of interventions related to Infant and Young Child Health therefore envisage the promotion of- Improved new born care and care of low birth weight babies. Bi annual vitamin Asupplementation for children 9-59 months Universal, timely and complete immunization of infants against vaccine preventable diseases (and subsequent booster doses) with quality assurance. Ensuring that young children receive micronutrient supplementation and bi annual deworming as per MHFW guidelines. This includes- IFAsupplementation for children 6-59 months. Bi annual deworming for children Over 1 year-59 months (linked to bi annual VAS rounds). Prevention and management of common neonatal and childhood illnesses such as diarrhoea (with ORS and zinc supplementation) and Acute Respiratory Infections (ARI) and severe acute malnutrition, at community and facility levels
Maternal Care, Health and Nutrition Interventions for maternal care, health and nutrition therefore include the promotion of- Improved supplementary nutritional support during pregnancy and lactation (ICDS). Improved antenatal care - including health and nutrition counseling (also family support for extra diet and rest to ensure adequate weight gain), IFA supplementation, consumption of adequately iodized salt and screening /management of severe anemia. Enhanced maternity protection (through the effective implementation of PMMVY) Institutional deliveries, lactation management, improved post-natal and new born care. Promoting marriage at the right age, first pregnancy at the right age, inter pregnancy recoupment/ birth spacing and shared care/ parenting responsibilities. Promoting Women s Literacy and Empowerment.
Adolescent Nutrition The interventions here - especially for improving the nutrition status of adolescent girls- will focus on the promotion of- Equal care of the girl child at different stages of the life cycle- linked to the Beti Bachao Beti Padhao initiative. Improved access to health care, counseling support through school health programmes, ARSH and deworming as per MHFW National Deworming Initiative. Improved access to nutritional support through Mid-Day Meals in schools (MHRD) and through SABLA for out of school girls. Universal access of girls in school and girls out of school to IFAsupplementation. Girls education, skill development and female literacy. Changing gender constructs -Gender sensitization and life skills for adolescents. No Child Marriage- Marriage of young women after the age of 18 years.
Community Nutrition These interventions include, among others- Ensuring universal access to safe drinking water, sanitation and hygiene, in an open defecation free environment, through Swachh Bharat. Prevention and treatment for malaria through the - Use of bed-nets and/or intermittent preventive therapy for malaria (as per MHFW protocols) in malaria-endemic areas - Facilitating mosquito control measures. Other relevant health /disease control measures specific for the state/district, relevant for improving nutrition at community levels - such as JE, kala azar etc. Ensuring access to household food security, social protection systems and safety nets. Nutrition Education to ensure that optimal feeding and caring practices, dietary diversity, nutritious foods; sanitation and hygiene and healthy lifestyles
Core Strategies - HOW Governance Reform- Nutrition Centre Stage and PublicAccountability Leading by Example- Kuposhan Mukt States, districts and panchayats. Convergence- of State/ District Implementation Plans for ICDS, NHM and Swachh Bharat and others, addressing different determinants of undernutrition together. PrioritizeAction- Reaching the most vulnerable communities in the districts/blocks with the highest levels of child undernutrition. Counseling to Reach the Critical Age Group- pregnant and lactating mothers, and children under 3 years, through skilled counselors, peer counselors and support groups. Continuum of care- across the life-cycle that includes preventive, promotive and curative care, linking families, communities, AWCs, health centers and health facilities. Innovative Service Delivery Models- demonstration and ripple effect, with evidence of impact. Community Based Monitoring- Making undernutrition visible to families, communities, Enabling Actions- Implementing innovative components of ICDS Restructuring; Cr ches through MGNREGA; Extending SABLA and implementing Maternity Benifits through Pradhan Mantri Matru Vandana Yojana and Strengthening Nutrition within the Health System tracking and informed action.
TRACKING & RECOGNIZING PROGRESS The new Nutrition Monitoring System will enable tracking of progress at different levels and identification of states/ districts/blocks/ AWCs that are performing well and those that are lagging behind, using lead indicators and tools such as dashboards and score cards, with wide dissemination of the same, including display on the relevant websites of the Ministry/State government department/district. This will be reviewed regularly by the proposed NNM Mission Steering Groups at National/ state levels and by NNM District Committees, with corrective actions suggested. NATIONALNUTRITION SURVEILLANCE SYSTEM A National Nutrition Surveillance System should be set up, building on previous experience in states such as Andhra Pradesh. This will include an early warning system for increase in nutritional vulnerabilities, through assessment and analysis with trigger points for timely corrective action, through
development programmes and safety nets. The use of sentinel sites will be pursued and multiple vulnerabilities tracked such as those related to socio-economic deprivation, agrarian distress, seasonal migration, distress, seasonal migration, disruptions in access to services, lack of access to social protection measures, disease outbreaks, endemic disease areas, natural disasters etc. Mapping of undernourished endemic zones of the country in terms of identifying high risk and vulnerable districts for the rest of districts, cases of severe undernutrition in children should be included in the routine disease reporting system. The surveillance system will also enable epidemiological investigation of malnutrition clusters and traditional endemic zones, using verbal autopsy to determine the underlying causes of deaths, besides the immediate cause.
The nutrition surveillance system will be GIS (Geographic Information System) based for tracking severely undernourished children, families and communities in the long run. This will not only ensure child-wise tracking, appropriate care, feeding and medical interventions for severely undernourished children- but also help link the families of severely undernourished children with social protection measures, food security measures and to access employment through MGNREGA/ other livelihood options. As required, linkages will also be established with the National Integrated Disease Surveillance System, as a significant proportion of under 5 child deaths reflect the vicious cycle of severe undernutrition and disease/infections. The design of the proposed National Nutrition Surveillance System will be developed subsequently by the National Nutrition Mission, with support from National Institute of Nutrition.
RESEARCH & EVALUATION NUTRITION SURVEY The Nutrition Strategy will use a systematic population sample based survey to assess baseline, mid term and final evaluation of Nutrition outcomes and overall progress of the key monitorable targets, nutrition outcomes, related nutrition and health process indicators. This will include anthropometric indices as related to maternal and child nutrition, as well as assessment of anemia prevalence. Data from service providers (ICDS, NHM) will be used for regular programmatic monitoring for improved programme effectiveness and efficiency
ESTIMATED RESOURCE REQUIREMENT It may be assumed that the Strategy will be implemented using resources of the major flagship programmes involved - NHM, ICDS, Swachh Bharat and resources earmarked for the upcoming National Nutrition Mission (including ICT enabled monitoring and a Nutrition Surveillance System). The increased provision of 25 % of flexi funds for States in Centrally sponsored schemes and the enhanced resources devolved to States, panchayats and urban local bodies would also be catalyzed for the purpose. Additional resources would be needed for flexible responses at district level (as in MP), local innovation, gap filling and incentivisation of good performance.












 Public Distribution System: Ensuring an equitable")
 Land Reforms:")
 Prevention of Food Adulteration: Prevention of")
 Equal Remuneration: Special efforts should be made to")