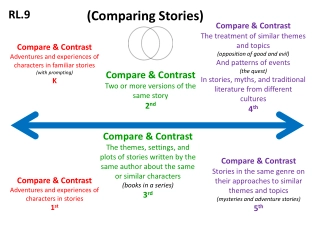
Exploring PrEP Retention Strategies: Insights and Real-Life Stories
This content delves into PrEP retention protocols and real-life stories of individuals discontinuing PrEP due to various reasons such as gaps in sexual activity, entering long-term relationships, or concerns about side effects. It highlights the challenges in retaining individuals on PrEP and emphasizes the importance of tailored retention strategies for diverse populations.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Orange County 2021 PrEP Navigation TA Workshop June 29-July 1, 2021 Retention Robert Wilder Blue, MSW California Prevention Training Center Robert.Blue@ucsf.edu No financial disclosures
PrEP Retention Protocol @SF City Clinic ______________________________ Follow-up call 7 days after initiation Visit reminder 2 weeks before expected 3- month follow-up Missed visit contact 1 week after patient expected for follow-up Patient remains in retention system 6 months after missed visit; receives 3-month reminder; then considered lost-to-follow-up Extra care for vulnerable patients
______________________________ Program administration: cohort management PrEP Retention
_______________________________ Defining retention and persistence (1)(2) Retention in PrEP care (also called persistence on PrEP) does not have a standard definition. Most research and implementation analyses have looked at retention as remaining in PrEP care for 6 months. Data indicate that 25 63% of people who initiate PrEP are still in PrEP care at 6 months. PrEP Retention
________________________________ Data to Real Life Retention stories (3, 4) Gaps in sexual activity motivated one 37-year-old Black MSM to repeatedly pause and then finally discontinue PrEP: If a month went by, or two months went by where I wasn t having sex, then I would stop taking it. And I wouldn t have sex unless I was on PrEP for at least a week. So, I stopped taking PrEP, I would probably say, like six months ago?
________________________________ Retention stories (3, 4) 33-year-old White MSM, expressed two common reasons for discontinuation: I stopped, because, I guess, two reasons. One is that I got into sort of a long-term relationship, so it was like less... the value wasn t there. And then, the second was just I was always hesitant to stay on PrEP, because [I] just worried about putting like chemicals, drugs into my body...I didn t want to be taking something long-term that I didn t have to. But for the period up until when I quit, I like just weighed it, and it made sense for me to be on it. Data to Real Life
________________________________ Retention stories(3, 4) A 55-year-old Latinx MSM who subsequently seroconverted cited side effects as a reason for discontinuation: lots of upset stomach and horrible headaches and kind of feel[ing] weak at some point. So, I talked to my doctor and both we decided to get out of the PrEP, because it didn t work that well for me.... He suffered from depression, which he believed led him to pursue many sexual partners, but the stigma he had experienced around talking about mental illness and about HIV made it difficult for him to seek help. When you [are gay and] came from places like Mexico. It s like the entire world is against you. I m ...asking people, how many of the Latinos really [are] taking or trust this pill. Data to Real Life
________________________________ Data to Real Life Retention stories(3, 4) Patients who were using PrEP regularly often found that sudden life changes made it difficult to prioritize taking PrEP. As one 26-year-old White male in a sero-different relationship noted: Well, so I lost my housing, and so in the midst of all that, there s just not going to doctor appointments...I was not really taking care of myself.
________________________________ Retention stories(3, 4) Providers recognized the challenge of taking a pill every day as a preventive measure. One clinician said: And [the patient] said, Why would I take a pill every day for something I don t have? And younger patients in particular, I think, who now see HIV as not this deadly disease, but just like a chronic disease, are like I would just be taking a pill if I had that. Nonetheless, providers relied primarily on their patients to reach out to them with specific concerns. Most providers reported not being aware that their patients had modified or stopped their PrEP regimens until several months later. Data to Real Life
________________________________ Retention stories(3, 4) Providers were largely aware of the complications of staying on PrEP in a context of unstable housing, substance use, and/or mental health problems. As one clinician described it: They have to check all of their meds in when they go to the shelter [T]presents a certain kind of barrier, but you know, it s more that people s stuff is lost or stolen if they re out on the streets... [Of] course, substance use and how that affects sort of sense of time and... taking a pill may or may not fall in their priorities, and then underlying mental health stuff. So, those are big things that come into play that sometimes interfere with starting PrEP or staying on PrEP. Data to Real Life
________________________________ Retention stories (3, 4) Changes in insurance status were another major cause of disruptions or changes in PrEP persistence. One 27-year-old Latinx MSM had to change to a large health maintenance organization (HMO), increasing his deductible to $400: And then my insurance changed. So, then that s when my PrEP usage changed, because I was an everyday, 12:00-on- the-dot person with it. But when my insurance changed, I m like, Okay, this is a bit different now. Now, how am I going to get this? One participant described his frustration after spending hours on the phone with insurance companies who ultimately gave him the wrong information. Data to Real Life
________________________________ Data to Real Life Retention stories (3, 4) An experienced PrEP navigator found the system inefficient and challenging: So, yeah, there are days where I end up spending half the day like fighting with an insurance company...[I]t s difficult when you support that many patients, but then also knowing that [insurance] could make or break... a patient s success on PrEP.
_________________________________ Data to Real Life Retention stories(3, 4) Some people expressed difficulty of attending scheduled appointments and the need to be at work or in school during clinic hours. Drop-in appointments or extended hours were mentioned as an important component for PrEP care by multiple participants. As one 22-year-old Black MSM stated: [T]he times that I am free, they re closed. And the times they re open, I m not free I ll go to school, and basically I m in training from 8:30 to 3:30 - that s without homework and stuff like that. By the time I get to [the youth clinic], [it s] closed.
_________________________________ Retention stories (3, 4) Some participants experienced stigma in pharmacies when filling their prescriptions. One explained: So then, dealing with pharmacies. There s this whole other layer of frustration, dealing with straight people who don t know what PrEP is. Another trans woman was going to be denied her PrEP because the pharmacist misidentified her as a ciswoman, and the insurance company did not see that as a sufficient PrEP indication. She had to explain to the pharmacist that she was a transwoman and that she qualified for PrEP. Data to Real Life
_______________________________ Data to Real Life Seroconversions (3, 4) Some participants reported that emphasis on needing to use PrEP because of "risk behavior" could be stigmatizing. One participant in particular felt motivated to try to change his sexual behavior rather than continuing to take PrEP. When he learned he had contracted HIV, he expressed regret at stopping PrEP: I talked to my doctor and we both decided to get off of PrEP because it didn t work that well for me [due to concerns about how he was perceived by his community]. But my behavior didn t just stop right there.
_______________________________ Data to Real Life Seroconversions (6) 18/1297 (1.4%) seroconverted after initiating PrEP at SF City Clinic 2 were still enrolled in PrEP care 7 had been lost to follow- Race/ethnicity 7 white (39%) 6 Latino (33%) 3 black (16%) 2 Asian (11%) Mean age 29 up 9 had stopped PrEP Median time to HIV diagnosis from discharge date = 190 days
_________________________________ Data to Real Life Seroconversion themes (6) Cost, coverage, and other logistics Problems with patient assistance program Insurance gap or change Too busy Difficulty picking up meds at pharmacy Change (or desired change) in sexual behavior In relationship with HIV- negative partner Didn t think at risk Trying to stop substance use and decrease sexual activity Trying to have fewer partners
PrEP Navigation: Core Competencies
_________________________________ Data to Real Life NO TIME/TOO BUSY DID NOT KNOW HOW TO GET PrEP DID NOT HAVE ACCESS TO A PREP PROVIDER INSURED, BUT STILL TOO EXPENSIVE MORE SERIOUS LIFE PROBLEMS CONCERNED ABOUT ADHERENCE DO NOT HAVE A DOCTOR CONCERNED ABOUT RISK COMPENSATION DO NOT KNOW ENOUGH ABOUT IT WOULD NOT SAY/JUST DOES NOT WANT IT MISTRUST OF DRUG COMPANY PRIVACY CONCERNS ONLY ONE PARTNER DENIED SERVICE BY PROVIDER ONLY HAVE ORAL SEX STIGMA CONCERNED ABOUT EFFICACY
_________________________________ * Diffen.com
Equality Equity _________________________________ Health equity is achieved when everyone has an equal chance to be healthy regardless of their background. This includes a person s race, ethnicity, income, gender, religion, sexual identity, and disability.* Q: How does the concept of sexual health equity relate to PrEP access and retention in your community? * The Community Guide: The Guide to Community Preventive Services. Community Preventive Services Task Force.
________________________________ Why We re Here Envision your role in ending the HIV epidemic.
PrEP Retention __________________________ Questions? Comments? Thank you! Robert Wilder Blue California Prevention and Training Center (415) 637-5050 / Robert.Blue@ucsf.edu