Improving Colorectal Cancer Referrals Using FIT Pathway


F
I
T
<
1
0
P
a
t
h
w
a
y
W
e
b
i
n
a
r
w
i
t
h
A
m
e
l
i
a
R
a
n
d
l
e
,
S
W
A
G
C
l
i
n
i
c
a
l
D
i
r
e
c
t
o
r
,
a
n
d
L
o
u
i
s
e
H
u
n
t
,
C
o
n
s
u
l
t
a
n
t
C
o
l
o
r
e
c
t
a
l
S
u
r
g
e
o
n
,
S
o
m
e
r
s
e
t
F
o
u
n
d
a
t
i
o
n
T
r
u
s
t
09.09.2020
A
g
e
n
d
a
G
l
o
s
s
a
r
y
•
FIT – Faecal Immunochemical Test
•
Negative FIT – FIT result <10
•
Positive FIT – FIT result >10
•
2ww – Suspected cancer referral under two-week-wait rule
R
a
t
i
o
n
a
l
e
The availability of colonoscopy has been significantly reduced by the Coronavirus Pandemic.
•
The maximum possible capacity for inpatient and critical care has been freed up, and preparations made to
respond to large numbers of inpatients requiring respiratory support.
•
To reduce the risk of coronavirus transmission during endoscopy special procedures are necessary. These
reduce the number of tests than can be done in a single session.
•
The current advice from the British Society of Gastroenterology (BSG) for endoscopy services, is to
investigate only urgent cases.
•
Colorectal teams are using Faecal Immunohistochemical Testing (FIT) to help prioritise referrals.
There has been a reduction in the number of referrals for suspected colorectal cancer:
•
Patients practicing social distancing in accordance with government guidance have not been engaging with
health services for fear of burdening the NHS, or of contracting the virus.
•
Overlap of symptoms of coronavirus in patients with symptoms of suspected cancer may delay diagnosis.
Trusts in SWAG are preparing to manage the backlog of patients whose investigations have been delayed,
alongside an additional increase in primary referrals as services return to normal.
T
h
e
P
r
o
b
l
e
m
•
There is widespread agreement in the use of FIT as a tool to triage colorectal 2 week-wait
referrals.
•
The national guidance is that patients with negative FIT should be held on a waiting list and
offered a colonoscopy at a later date.
•
Increasing clinical opinion is that these patients can be safely reassured and given ‘safety-
netting’ advice
•
A small number of patients with negative FIT will later be diagnosed with colorectal cancer (From
evidence range of figures from 1:200 to1:1000)
•
Reassuring patients with a negative FIT without referral, will allow patients with higher risk
symptoms to be assessed and treated more quickly as more colorectal team time will be
available.
B
e
f
o
r
e
C
O
V
I
D
-
1
9
,
a
l
l
p
a
t
i
e
n
t
s
r
e
p
r
e
s
e
n
t
e
d
b
y
a
r
e
d
b
o
x
w
e
r
e
o
f
f
e
r
e
d
a
c
o
l
o
n
o
s
c
o
p
y
N
a
t
i
o
n
a
l
C
O
V
I
D
-
1
9
P
a
t
h
w
a
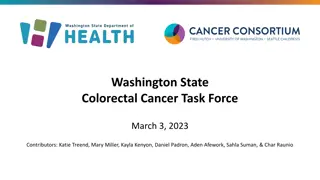
y
Patients in the orange box below will be offered a FIT, and if negative, held on a list awaiting further tests.
Patients in the red boxes are treated as before.
P
a
t
i
e
n
t
s
w
i
t
h
F
I
T
<
1
0
a
r
e
‘
s
a
f
e
t
y
-
n
e
t
t
e
d
’
o
n
a
p
a
t
i
e
n
t
t
r
a
c
k
i
n
g
l
i
s
t
u
n
t
i
l
i
n
v
e
s
t
i
g
a
t
i
o
n
s
c
a
n
b
e
c
o
m
p
l
e
t
e
d
Low risk patients are those with NG12-specified symptoms and a FIT <10µg/g.
A
l
l
p
a
t
i
e
n
t
s
p
l
a
c
e
d
o
n
t
r
a
c
k
i
n
g
l
i
s
t
s
s
h
o
u
l
d
h
a
v
e
a
v
i
r
t
u
a
l
c
o
n
s
u
l
t
a
t
i
o
n
t
o
p
r
o
v
i
d
e
i
n
f
o
r
m
a
t
i
o
n
a
n
d
r
e
a
s
s
u
r
a
n
c
e
.
T
h
e
y
s
h
o
u
l
d
b
e
g
i
v
e
n
a
d
v
i
c
e
o
n
w
h
a
t
t
o
d
o
i
f
t
h
e
i
r
s
y
m
p
t
o
m
s
p
r
o
g
r
e
s
s
.
While many patients with a FIT <10 will not require endoscopy, patients should not be discharged from the 2WW
pathway on the basis of a FIT test alone, except in existing FIT pioneer service evaluation sites that were piloting the
use of FIT before the COVID-19 outbreak.
1
,
0
0
0
F
I
T
T
e
s
t
s
1,000 FIT tests
•
925 appropriately reassured without colonoscopy
•
52 prioritised for investigation and cancer ruled out
•
18 prioritised for investigation and diagnosed with
cancer
•
1-5 potential delayed cancer diagnosis
S
W
A
G
C
a
n
c
e
r
A
l
l
i
a
n
c
e
p
r
o
p
o
s
e
d
c
o
l
o
r
e
c
t
a
l
c
a
n
c
e
r
p
a
t
h
w
a
y
,
d
u
r
i
n
g
C
O
V
I
D
r
e
c
o
v
e
r
y
p
h
a
s
e
Primary Care Clinical Assessment
Remote assessment with face to face for physical exam, rectal examination (PR) abdominal examination
Bloods: Full Blood Count , Ferritin, Urea and Electrolytes, Liver Function Tests, C-reactive Protein
If reassessing after negative FIT and ongoing NG12 symptoms, repeat FIT after 6 weeks
If ongoing symptoms and negative FIT x 2 advice and guidance
60+ change
in bowel
habit
•
50+ unexplained
rectal bleeding
•
60+ IDA rectal
mass
•
40+ unexplained
weight loss and
abdominal pain
•
Abdominal mass
•
<50 rectal bleeding
and abdominal pain
•
Weight loss or iron
deficiency anaemia
Symptoms
not
meeting
2WW or
NSS RDS
criteria
Symptoms
resolved
Reassurance
and safety
netting
GP diagnosis
and
management
with Advice
and
Guidance or
routine
referral
FIT
NSS RDS
available?
NSS
RDS
Suspected
cancer (2WW)
referral
FIT
GP reassess
positive
negative
positive
negative
Yes
No
Key:
Purple:
existing pathway
Red:
existing 2WW referral
Green:
proposed new
pathway
Colorectal Advice and
Guidance
2 x FIT negative and
ongoing symptoms
D
i
s
c
u
s
s
i
o
n
S
u
m
m
a
r
y
•
Proposals seem ‘doable’ with the reassurance of they’re in the system
•
It’s correct and proper that GPs address the emerging problem of a limited
resource versus high demand
Conversations with GPs to establish they are happy to take on ‘extra’ workload
Also shared conversations GPs/Clinicians/Patients – aim is to limit the anxiety of
those ‘on hold.’ Don’t mind waiting but open-ended waiting not acceptable.
Importance of clarity on what the next step is and when it will take place.
•
Trying to establish a moral/clinical pathway
•
Clinicians want to be pragmatic and move away from current NICE guidance
•
Exploring this with CA allows People/Patient view which is overall support for why clinicians have
taken this course
•
Request for feedback ‘after the event’
•
Noted that from the SWCS Council meeting 29/09/18 that the various scale sensitivity of FIT
Tests is always improving as a diagnostic so already a very good indicator of patient point on a
pathway.
Recording of session: (From 4.30 min to 46.30 min)
https://web.microsoftstream.com/video/082e19b1-ebf0-444b-9160-9425d0a650e0
C
o
l
o
r
e
c
t
a
l
c
a
n
c
e
r
•
Colorectal cancer (CRC) is the fourth most common cancer diagnosis in the UK and
the second most common cause of cancer‐related death
•
In 2016, over 260,000 patients with lower abdominal symptoms were investigated
following an urgent GP referral for suspected cancer.
•
The majority of these patients were referred to colonoscopy or CT colonoscopy but
only about 3-4% of them will have cancer.
•
The introduction of the 2‐week‐wait (2WW) pathway in 2000 has had limited
beneficial impact on clinical outcomes for CRC
•
The CRC 2WW pathway consumes huge diagnostic capacity at great cost, and
pressure continues to grow
•
FIT has been shown to outperform traditional referral criteria
•
Combining FIT with referral criteria and anaemia could potentially minimize the
risk of missed diagnosis but also identify high‐risk groups most likely to benefit
from rapid investigation
S
t
u
d
i
e
s
f
r
o
m
t
h
e
U
K
•
Godber et al Clin Chem Lab Med 2016; 54(4): 595–602
•
Scottish study using FIT at a 10µg/g threshold
•
Sensitivity for colorectal cancer -> 100% and specificity -> 80.2%
•
PPV -> 26.3% and NPV -> 100%
•
Widlak et al Aliment Pharmacol Ther 2017; 45: 354–363
•
English study
•
Sensitivity -> 84% and specificity -> 93%
•
NPV -> 99%
E
a
r
l
y
c
l
i
n
i
c
a
l
o
u
t
c
o
m
e
s
o
f
a
r
a
p
i
d
c
o
l
o
r
e
c
t
a
l
c
a
n
c
e
r
d
i
a
g
n
o
s
i
s
p
a
t
h
w
a
y
u
s
i
n
g
f
a
e
c
a
l
i
m
m
u
n
o
c
h
e
m
i
c
a
l
t
e
s
t
i
n
g
i
n
N
o
t
t
i
n
g
h
a
m
•
C. Chapman, C. Thomas, J. Morling, A. Tangri, S. Oliver, J. A. Simpson,D. J. Humes and A. Banerjea
•
Colorectal Disease Dec 2019
22, 679–688
•
The CRC detection rate in 531 patients investigated after a FIT result of < 4.0 lg Hb/g faeces was 0.2%.
•
In 899 investigated patients, a FIT result with a threshold of 4.0 lg Hb/g faeces had sensitivity 97.2% (85.5–
99.9% CI), specificity 61.4% (58.1 –64.7% CI), negative predictive value 99.8% (98.7–100.0% CI) and
positive predictive value 9.5% (8.7–10.4% CI)
W
h
a
t
i
s
F
I
T
?
•
Quantitative Faecal Immunochemical Test is a test to detect hidden or ‘occult’
blood in stool samples.
•
U
n
l
i
k
e
o
l
d
e
r
F
O
B
t
e
s
t
s
,
F
I
T
u
s
e
s
a
n
t
i
b
o
d
i
e
s
t
h
a
t
s
p
e
c
i
f
i
c
a
l
l
y
r
e
c
o
g
n
i
s
e
h
u
m
a
n
h
a
e
m
o
g
l
o
b
i
n
a
n
d
s
o
t
h
e
r
e
i
s
n
o
n
e
e
d
f
o
r
p
a
t
i
e
n
t
s
t
o
u
n
d
e
r
g
o
d
i
e
t
a
r
y
r
e
s
t
r
i
c
t
i
o
n
p
r
i
o
r
t
o
u
s
i
n
g
t
h
e
t
e
s
t
.
•
As it is antibody based, FIT is a more sensitive and specific test than the guaiac
test.
•
This reduces the chances of false positives.
•
The quantitative threshold for the Bowel Cancer Screening Programme qFIT is
much higher than that used in our ‘Symptomatic qFIT’ testing, so a recent
‘normal’ or ‘negative’ from the screening programme should not be relied on by
GPs for reassurance.
•
i.e. >120 for BCSP vs >10 for the 2WW pathway
T
a
u
n
t
o
n
E
x
p
e
r
i
e
n
c
e
d
u
r
i
n
g
C
O
V
I
D
•
Lockdown 23 March 2020
•
Some restrictions lifted 1 June 2020
•
Normally 40-50 referrals per week
•
Dropped to about 17-20 per week
•
Unable to investigate ALL but most urgent (usually inpatients)- only plain CT, no
scopes
C
O
V
I
D
2
W
W
R
e
f
e
r
r
a
l
s
•
Database 16/03/20 – 01/06/20
•
282 referrals
•
11 cancers (4%)(8 had FIT , All >50; range 55->400)
•
223 investigated and discharged
•
10 other cancers (prostate, pancreas, CLL, ovary)
•
7 colitis
•
31 declined investigation/ deferred until AFTER
C
O
V
I
D
2
W
W
R
e
f
e
r
r
a
l
s
E
n
d
o
s
c
o
p
y
&
R
a
d
i
o
l
o
g
y
W
a
i
t
i
n
g
L
i
s
t
•
Around 600 FIT tests sent out
•
Stratified patients for investigation in order of priority
>400
100-400
>100
>10
<10
P
a
t
h
w
a
y
I
s
s
u
e
s
•
Reduced capacity for investigation
•
97% do NOT have CRC
•
Endoscopy working at 75% capacity (from ZERO in April)
•
Radiology working at about 60% (from 10% in April)
•
Reduced Outpatient capacity (F2F)
•
Significant backlog
Q
u
e
s
t
i
o
n
s
?
The FIT Pathway for suspected colorectal cancer aims to optimize referrals amidst reduced endoscopy availability due to the pandemic. By utilizing the Faecal Immunochemical Test (FIT) to triage patients, it allows for the prioritization of urgent cases, reducing the number of unnecessary colonoscopies and ensuring timely treatment for high-risk individuals. This strategy addresses the challenges posed by the current healthcare landscape, where balancing urgent care needs with limited resources is crucial for effective patient management and outcomes.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
FIT <10 Pathway Webinar with Amelia Randle, SWAG Clinical Director, and Louise Hunt, Consultant Colorectal Surgeon, Somerset Foundation Trust 09.09.2020
Agenda Agenda Item Welcome and Introduction Dr Amelia Randle, Clinical Director, SWAG Cancer Alliance The FIT <10 Pathway for Suspected Colorectal Cancer Dr Amelia Randle, Clinical Director, SWAG Cancer Alliance 2ww Colorectal cancer and qFIT Louise Hunt, Somerset NHS Foundation Trust Discussion and Q&A Opportunity AOB
Glossary FIT Faecal Immunochemical Test Negative FIT FIT result <10 Positive FIT FIT result >10 2ww Suspected cancer referral under two-week-wait rule
Rationale The availability of colonoscopy has been significantly reduced by the Coronavirus Pandemic. The maximum possible capacity for inpatient and critical care has been freed up, and preparations made to respond to large numbers of inpatients requiring respiratory support. To reduce the risk of coronavirus transmission during endoscopy special procedures are necessary. These reduce the number of tests than can be done in a single session. The current advice from the British Society of Gastroenterology (BSG) for endoscopy services, is to investigate only urgent cases. Colorectal teams are using Faecal Immunohistochemical Testing (FIT) to help prioritise referrals. There has been a reduction in the number of referrals for suspected colorectal cancer: Patients practicing social distancing in accordance with government guidance have not been engaging with health services for fear of burdening the NHS, or of contracting the virus. Overlap of symptoms of coronavirus in patients with symptoms of suspected cancer may delay diagnosis. Trusts in SWAG are preparing to manage the backlog of patients whose investigations have been delayed, alongside an additional increase in primary referrals as services return to normal.
The Problem There is widespread agreement in the use of FIT as a tool to triage colorectal 2 week-wait referrals. The national guidance is that patients with negative FIT should be held on a waiting list and offered a colonoscopy at a later date. Increasing clinical opinion is that these patients can be safely reassured and given safety- netting advice A small number of patients with negative FIT will later be diagnosed with colorectal cancer (From evidence range of figures from 1:200 to1:1000) Reassuring patients with a negative FIT without referral, will allow patients with higher risk symptoms to be assessed and treated more quickly as more colorectal team time will be available.
Before COVID-19, all patients represented by a red box were offered a colonoscopy Abdominal mass Rectal mass Rectal Bleeding and 1 other symptom1 Abdominal pain and weight loss FIT >10 Rectal bleeding Change in bowel habit Iron deficiency anaemia Age <40 40-50 50-60 60+
National COVID-19 Pathway Patients in the orange box below will be offered a FIT, and if negative, held on a list awaiting further tests. Patients in the red boxes are treated as before. Abdominal mass Rectal mass Rectal Bleeding and 1 other symptom1 Abdominal pain and weight loss FIT >10 Rectal bleeding Change in bowel habit Iron deficiency anaemia Age <40 40-50 50-60 60+ Patients with FIT <10 are safety-netted on a patient tracking list until investigations can be completed Low risk patients are those with NG12-specified symptoms and a FIT <10 g/g. All patients placed on tracking lists should have a virtual consultation to provide information and reassurance. They should be given advice on what to do if their symptoms progress. While many patients with a FIT <10 will not require endoscopy, patients should not be discharged from the 2WW pathway on the basis of a FIT test alone, except in existing FIT pioneer service evaluation sites that were piloting the use of FIT before the COVID-19 outbreak.
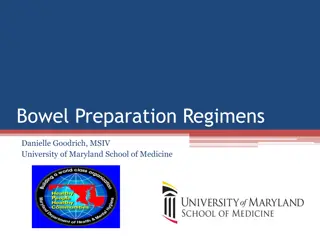
1,000 FIT Tests 1,000 FIT tests Cancer No Cancer total 925 appropriately reassured without colonoscopy 52 prioritised for investigation and cancer ruled out 18 prioritised for investigation and diagnosed with cancer 1-5 potential delayed cancer diagnosis FIT >10 18 52 70 FIT <10 1-5 925 930
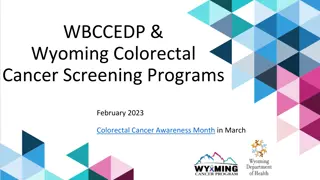
SWAG Cancer Alliance proposed colorectal cancer pathway, during COVID recovery phase
Primary Care Clinical Assessment Remote assessment with face to face for physical exam, rectal examination (PR) abdominal examination Bloods: Full Blood Count , Ferritin, Urea and Electrolytes, Liver Function Tests, C-reactive Protein If reassessing after negative FIT and ongoing NG12 symptoms, repeat FIT after 6 weeks If ongoing symptoms and negative FIT x 2 advice and guidance 50+ unexplained rectal bleeding 60+ IDA rectal mass 60+ change in bowel habit 40+ unexplained weight loss and abdominal pain Abdominal mass <50 rectal bleeding and abdominal pain Weight loss or iron deficiency anaemia Symptoms not meeting 2WW or NSS RDS criteria Symptoms resolved Reassurance and safety netting GP reassess Suspected cancer (2WW) referral GP diagnosis and management with Advice and Guidance or routine referral positive negative positive FIT FIT negative Key: NSS RDS available? Purple: existing pathway Red: existing 2WW referral Green: proposed new pathway No Yes 2 x FIT negative and ongoing symptoms Colorectal Advice and Guidance NSS RDS
Discussion Summary Proposals seem doable with the reassurance of they re in the system It s correct and proper that GPs address the emerging problem of a limited resource versus high demand Conversations with GPs to establish they are happy to take on extra workload Also shared conversations GPs/Clinicians/Patients aim is to limit the anxiety of those on hold. Don t mind waiting but open-ended waiting not acceptable. Importance of clarity on what the next step is and when it will take place. Trying to establish a moral/clinical pathway
Clinicians want to be pragmatic and move away from current NICE guidance Exploring this with CA allows People/Patient view which is overall support for why clinicians have taken this course Request for feedback after the event Noted that from the SWCS Council meeting 29/09/18 that the various scale sensitivity of FIT Tests is always improving as a diagnostic so already a very good indicator of patient point on a pathway. Recording of session: (From 4.30 min to 46.30 min) https://web.microsoftstream.com/video/082e19b1-ebf0-444b-9160-9425d0a650e0
Colorectal cancer Colorectal cancer (CRC) is the fourth most common cancer diagnosis in the UK and the second most common cause of cancer related death In 2016, over 260,000 patients with lower abdominal symptoms were investigated following an urgent GP referral for suspected cancer.
The majority of these patients were referred to colonoscopy or CT colonoscopy but only about 3-4% of them will have cancer. The introduction of the 2 week wait (2WW) pathway in 2000 has had limited beneficial impact on clinical outcomes for CRC
The CRC 2WW pathway consumes huge diagnostic capacity at great cost, and pressure continues to grow FIT has been shown to outperform traditional referral criteria Combining FIT with referral criteria and anaemia could potentially minimize the risk of missed diagnosis but also identify high risk groups most likely to benefit from rapid investigation
Studies from the UK Godber et al Clin Chem Lab Med 2016; 54(4): 595 602 Scottish study using FIT at a 10 g/g threshold Sensitivity for colorectal cancer -> 100% and specificity -> 80.2% PPV -> 26.3% and NPV -> 100% Widlak et al Aliment Pharmacol Ther 2017; 45: 354 363 English study Sensitivity -> 84% and specificity -> 93% NPV -> 99%
Early clinical outcomes of a rapid colorectal cancer diagnosis pathway using faecal immunochemical testing in Nottingham C. Chapman, C. Thomas, J. Morling, A. Tangri, S. Oliver, J. A. Simpson,D. J. Humes and A. Banerjea Colorectal Disease Dec 2019 22, 679 688 The CRC detection rate in 531 patients investigated after a FIT result of < 4.0 lg Hb/g faeces was 0.2%. In 899 investigated patients, a FIT result with a threshold of 4.0 lg Hb/g faeces had sensitivity 97.2% (85.5 99.9% CI), specificity 61.4% (58.1 64.7% CI), negative predictive value 99.8% (98.7 100.0% CI) and positive predictive value 9.5% (8.7 10.4% CI)
What is FIT? Quantitative Faecal Immunochemical Test is a test to detect hidden or occult blood in stool samples. Unlike older FOB tests, FIT uses antibodies that specifically recognise human haemoglobin and so there is no need for patients to undergo dietary restriction prior to using the test. As it is antibody based, FIT is a more sensitive and specific test than the guaiac test. This reduces the chances of false positives.
The quantitative threshold for the Bowel Cancer Screening Programme qFIT is much higher than that used in our Symptomatic qFIT testing, so a recent normal or negative from the screening programme should not be relied on by GPs for reassurance. i.e. >120 for BCSP vs >10 for the 2WW pathway
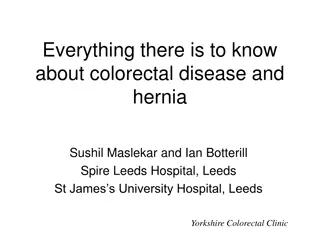
Lockdown 23 March 2020 Some restrictions lifted 1 June 2020 Normally 40-50 referrals per week Dropped to about 17-20 per week Unable to investigate ALL but most urgent (usually inpatients)- only plain CT, no scopes
Colorectal Referrals 80 70 60 50 40 30 20 10 0 w/c 23/09.19 w/c 31.12.18 w/c 14.01.19 w/c 28.01.19 w/c 11.02.19 w/c 25.02.19 w/c 11.03.19 w/c 25.03.19 w/c 08.04.19 w/c 22.04.19 w/c 06.05.19 w/c 20.05.19 w/c 03.06.19 w/c 17.06.19 w/c 01.07.19 w/c 15.07.19 w/c 29.07.19 w/c 12.08.19 w/c 26.08.19 w/c 09.09.19 w/c 07.10.19 w/c 21.10.19 w/c 04.11.19 w/c 18.11.19 w/c 02.12.19 w/c 16.12.19 w/c 30.12.19 w/c 13.01.20 w/c 27.01.20 w/c 10.02.20 w/c 24.02.20 w/c 09.03.20 w/c 23.03.19 w/c 06.04.20 w/c 20.04.20 w/c 04.05.20 w/c 18.05.20 w/c 01.06.20 w/c 15.06.20 w/c 29.06.20 w/c 13.07.20 w/c 27.07.20 w/c 10.08.20 w/c 24.08.20
COVID 2WW Referrals Database 16/03/20 01/06/20 282 referrals 11 cancers (4%)(8 had FIT , All >50; range 55->400) 223 investigated and discharged 10 other cancers (prostate, pancreas, CLL, ovary) 7 colitis 31 declined investigation/ deferred until AFTER
COVID 2WW Referrals Referrals CRC other cancer colitis discharged
Endoscopy & Radiology Waiting List Around 600 FIT tests sent out Stratified patients for investigation in order of priority >400 100-400 >100 >10 <10
Pathway Issues Reduced capacity for investigation 97% do NOT have CRC Endoscopy working at 75% capacity (from ZERO in April) Radiology working at about 60% (from 10% in April) Reduced Outpatient capacity (F2F) Significant backlog