The Impact of Social Prescribing on Health and Well-being



6
th
November, 2019
Mark Griffiths and Lucy Duncanson
Social prescribing link worker
intervention for health and
well-being










Enabling primary care
professionals to refer people
to a range of local, non-
clinical services using a
holistic approach, supporting
individuals to take control of
their own health.
What is social prescribing?
King’s Fund: Social Prescribing: coming of age
‘..what for many has seemed like
common sense and beneficial is increasingly now scientifically proven and gaining traction
in the medical world..’
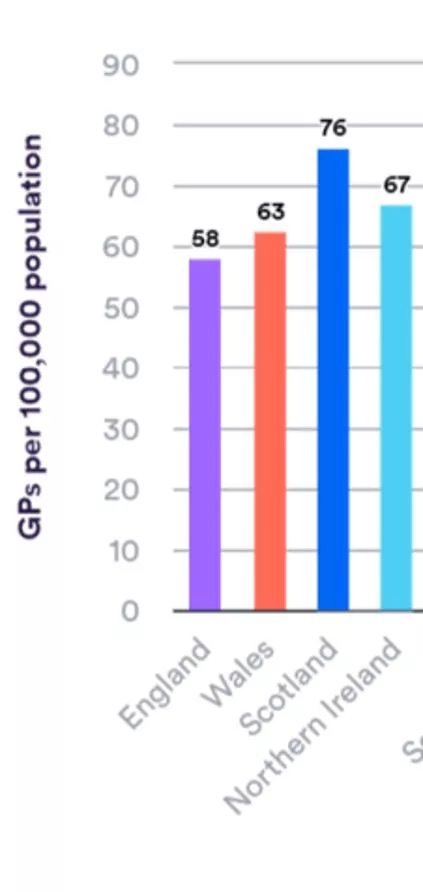
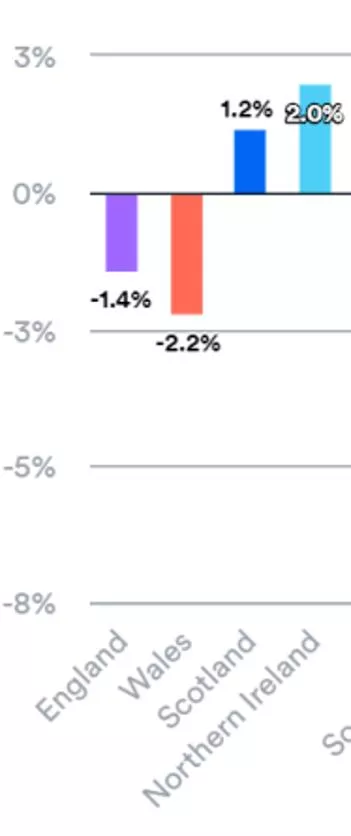
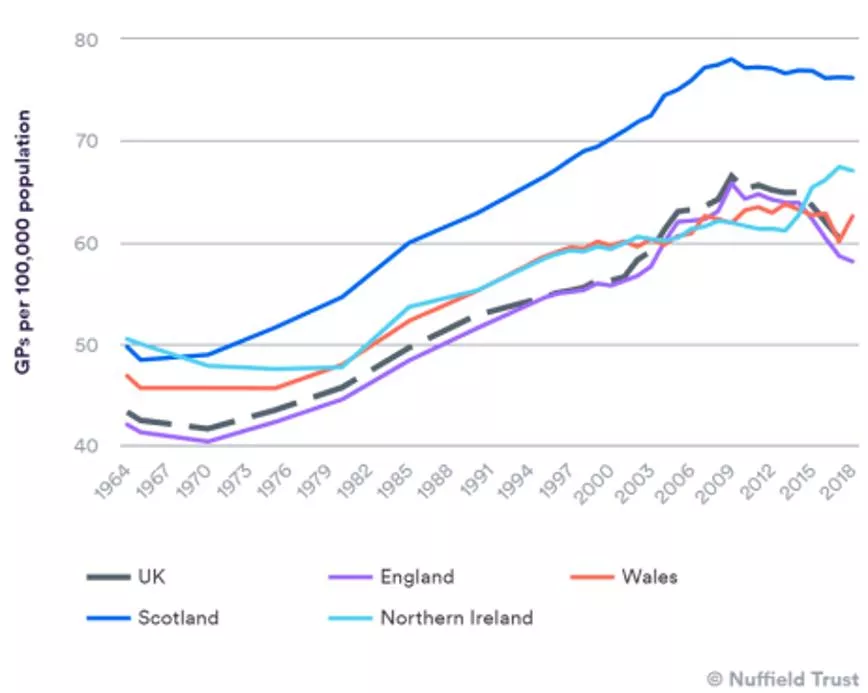
Is the number of GPs falling across the UK?
Changes in number of GPs between 2016-2018; level of GP
staffing, 2018
•
Standardise social prescribing
•
Increase awareness of the benefits
•
Build and promote the evidence base
•
Share best practice
•
Look at funding models
•
Create partnerships
•
Develop training and accreditation
The National Academy for Social Prescribing will:
•
Government will
support all local health and care systems to
implement social prescribing connector schemes across the
whole country
, supporting the aim to have a universal national offer
available in GP practices. It will also take steps to
improve and
share knowledge on effective social prescribing services
.
In
addition, the Department of Health and Social Care, NHS England and
the Department for Work and Pensions will commit to testing methods
that will
improve how a range of other organisations
(such as
community pharmacies, social workers, community nurses and
jobcentres)
refer into existing social prescribing services
.
National Loneliness Strategy
Mental Health and Well-being
• Prioritise mental health
treatment, support, prevention and
de-escalation, including
a pilot
Social Prescription scheme
and
increase access to talking therapies
Social Prescribing in Wales:
Theme: Healthy and active Wales
•
£1,351,066 of funding to deliver two
projects
•
Mind Cymru: co-produce a link
worker model for adults at risk of
poor mental health in Taf Ely, South
Powys and North Denbighshire
•
British Red Cross: test two models
for patients with mental health
problems and are frequent attenders
of GP or ambulance services in
Pembrokeshire and Caerphilly.
•
Primary question:
to what extent does the role of the link worker
effect recruitment into, and retention in community-based social
prescribing services.
•
Secondary objectives: report health and well-being measures as an
indicator of our population
Research proposal
Objectives:
•
Recruit 20 patients in the North Ceredigion GP clusters (7 GP
practices, c. 47k population)
Methodology
•
Recruit 20 patients in the North Ceredigion GP clusters (7 GP
practices, c. 47k population)
•
Participants interviewed by LW, complete Warwick-Edinburgh
Mental Well-being Scale (WEMWBS)
Methodology
•
A validated 14 item questionnaire
•
Likert scale 1-5 (cumulative score 14-70)
•
Available in English and Welsh
•
UK adult population norm c. score of 51
Warwick-Edinburgh Mental Well-being
Scale (WEMWBS)
•
Recruit 20 patients in the North Ceredigion GP clusters (7 GP
practices, c. 47k population)
•
Participants interviewed by LW, complete WEMWBS
•
Participants receive a health and well-being assessment
Stature, mass - BMI
Resting Blood Pressure
Heart rate
•
Participants agree a “social prescription” to follow for 3 months,
‘
meeting’
monthly with the link worker (LW) to discuss progress
•
Repeat all health assessments after 3 month intervention
•
Participation in a focus group meeting to discuss SP and LW role
Methodology
The ‘social prescription’
Project plan
•
17 referrals - I met with 13 participants
for up to 2hrs, Co-wrote a ‘prescription’
of what they wanted to do.
•
Participants can tell you anything.
Support for link workers is vital –
supervision sessions.
Initial Meeting With Participants
Issues included:
suicide attempts, serious miscarriage
of justice, domestic violence,
loneliness, anxiety, hording, rejection,
post traumatic stress, harmful drinking,
isolation, depression,
bereavement
There were many unnecessary barriers to people
joining groups. Many referrals had to be chased up.
There was a lot of inaccurate information online and
during telephone conversations.
Participants were
not kept informed or were unaware of when activities
were starting or how long waiting lists were. Follow
up is essential, and in some cases it took many months
for the participants to be invited to join the activity.
•
Significantly Reduced harmful drinking
•
Increased walking
•
Quit smoking for 3 weeks
•
Joined a woodland group
•
Found out about housing options in town
•
Motivated to volunteer as hospital radio DJ
•
Registered as a carer, on waiting list for respite
•
Received disability adaptations in the bathroom
•
Joined Foodwise for Life course
•
Receiving post traumatic stress counselling
•
Re joined cardiac rehabilitation
•
Got a blue badge to help parking
•
Started exercise referral
•
Told something I haven't told anyone before
•
Since meeting you things have gone from nowhere to
top of the hill. I’m living in hope at the moment.
•
I don’t mix well with people. I was craving a social life.
•
Given priority on social housing waiting list
•
Helped me focus.. You look at the whole person
•
Just talking and being listened to made the difference
Impact of engagement - What difference did it make in people’s lives
What wouldn’t have happened without the support of the social prescribing link
worker
•
Lack of awareness of groups on offer
•
Participants require motivational support to link in with a new
activity
•
The role of a group leader in welcoming new members and
helping them feel included is vital. This role should be paid.
•
Referral follow up is essential. Many took months for the
participants to be invited to join the activity
•
Inaccurate information online and given during telephone
conversations.
Community Groups & Referrals
•
It was a challenge - texting was best.
•
Each call gave me extra work – despite the fact I was encouraging
participants to find their own solutions.
Keeping in touch
I was labouring under the
misapprehension that no
one gave a damn, but now
I know there are people
out there that really care.
That first chat
made a big
difference
What Worked Well
Working knowledge and relationship with primary care
Motivational Interviewing and Mental Health First Aid training
G
ood local knowledge of groups and services locally.
Written
‘social prescription’
One referral leading to others.
What Didn’t
Participants didn't really join groups. They were mainly referred into services.
No referrals were received from Tregaron or Aberaeron GP surgeries.
Five participants showed a keen interest in volunteering. Only
one followed this through.
Challenges
One participant joined a group which they really enjoyed, but felt lonelier afterwards.
Most conversations with the participant resulted in more work for
me
People answering the phone.
Waiting lists and being kept informed of services
“It is really hard to navigate ‘the
system’ of life when you have had
knockbacks, are lonely, or have
been bereaved.
There is no magic one size fits all
solution.”
Social Prescribing Link Worker
•
A co-produced ‘social prescription’ was useful
•
Link worker helped motivate participants, identify actions, navigate
bureaucracy & ensure referrals were acted on.
•
During follow up people are saying they haven’t done anything. They
are not recognising / valuing the changes they have made.
•
Paid, trained members of community groups are needed to welcome
and support new members.
•
Cannot make people conform and fit in boxes and be expected to join
a group for the sake of it. Life is not that simple.
Reflections
•
No difference between baseline and at
3 months (37.9 – 38.5)
•
Wide variance
•
Range:
(Baseline) = 16–62
after intervention = 14-65)
Results
WEMWBS
•
No difference between baseline and
at 3 months
•
Ranges
o
Weight: 66.6-158.6kg
o
BMI: 27.0-47.1 kg/m
2
Results
Weight and BMI
•
No difference between baseline and at 3 months
Results
Blood pressure and heart rate
Perception of LW:
•
Added value of local knowledge &
ability to
harass
local community
service providers
•
LW as a therapeutic intervention
(positivity and approachability)
•
Identification of most appropriate
activities and facilitate participation
•
Participant’s desire to please the LW
Focus Group
Primary Objective: extent to which the link worker effects
recruitment into and retention in social prescribing services?
“Lucy knew an awful lot about what was
going on …without having to look
everything up... She seemed to know
everyone and everything”
“It would be helpful for someone to
accompany you, to go with you. To help
break the ice and put your foot through
the door”
“I knew what I didn’t want to do before
project. It was just nice to have
someone to speak to. Lucy is lovely.”
Meetings:
•
Location/flexibility of LW meetings impacts participants in a rural
community.
•
Participants wanted more contact with LW and goal setting
•
LW showing personal interest
Resourcing:
More funding for LW role
Focus Group
Primary Objective: extent to which the link worker effects
recruitment into and retention in social prescribing services?
“I met Lucy in the Doctors. I wasn’t able to
get up here. Which made it easy for me.
Getting up here is not that easy. We met at
GP’s which was great.”
“I thought she was very helpful and
positive. Then we had to write
down our own goals. I wanted to
please – which I could follow
through with it.”
“Text was helpful- from Lucy the
day before to remind of
appointment. I thought the
project was over and that Lucy
had forgotten about me, and then
I heard from Lucy”
“More Link Workers…”
“hard for one Link Worker to do job for
seventeen participants. That’s a lot of
work….”
“That’s where your money needs to go.”
•
No differences in the physical and mental indicators of health –
weight, BMI, BP, resting HR and WEMWBS
•
Demonstrated feasibility to collect these data
•
Difficulties with getting participants into SP activities/schemes
•
Engagement with healthcare professionals could be improved
•
More research needed into recruitment and retention in mid-Wales
•
Repeat and recruit specific patient population e.g. frequent attenders
•
Longer intervention period
Conclusions
•
Social prescribing as a concept is not well understood by the public.
Better promotion of social prescribing and how to access services
•
Integrating infrastructure e.g. single point of access IT system linking
relevant databases with an up to date directory of services.
•
scope out what is essential / desirable training for the LW role.
•
Clinical/professional supervision outside of line management and
structured peer-support sessions to help manage workload and
patient demands.
Recommendations
•
Sustainability of social care services/community activities.
Resourcing and accurate information about services and activities
to ensure timely engagement and maintain individual’s motivation
•
Active LW engagement with GPs, social prescribing scheme
providers and each other to help understand patient trends, service
capacity/capability and promote engagement
•
A randomised control trial to determine if social prescribing can
deliver a return on investment.
Recommendations II
Mark Griffiths, PHW
(
mark.griffiths5@wales.nhs.uk
)
Laura Evans, PHW
(
laura.evans16@wales.nhs.uk
)
Lucy Duncanson, PHW
(
lucy.Duncanson@wales.nhs.uk
)
Anna Prytherch, RHCW
(
Anna.L.Prytherch@wales.nhs.uk
)
Rhys Thatcher WARU, AU
(
ryt@aber.ac.uk
)
Ceri Smith, PHW
(
ceri.smith3@wales.nhs.uk
)
Meet the team
Thank you
•
Lucy could mention…
o
principal research question ie to what extent does the role of the link worker effect
engagement with and adherence to community-based social prescribing services
o
Recruitment at which surgeries / or how many of the 7 surgeries were able to support,
speed of recruitment etc
o
How many retained, how many lost
o
Experiences of participants in attending meetings, follow ups,
o
Attitudes toward social prescribing, willingness to participate
o
Lessons learned
o
Pin board on next slide
LW Lucy… introducing
Lucy’s slide set…
•
Short, online survey (13 questions)
•
Shared with staff in Ceredigion GP
cluster
•
3 follow ups
•
1 response
•
Indicative of time pressures within
primary care
GP, Practice Manager and Health Professional Survey
Social Prescribing
Paperwork-a-plenty
•
17 referrals
•
I met with each of the 13 participants
for up to 2hrs, Co-wrote a ‘prescription’
of what they wanted to do.
•
Missed appointments: 19.
•
Participants can tell you anything.
Support for link workers is vital –
supervision sessions.
Initial Meeting With Participants
Independent
walking
NHS post
traumatic
stress
counselling
Woodland
activities
Groups,
activities &
services
•
Lack of awareness of groups on offer
•
Participants require motivational support to link in with a new
activity
•
The role of a group leader in welcoming new members and
helping them feel included is vital. This role should be paid.
•
Referral follow up is essential. Many took months for the
participants to be invited to join the activity
•
Inaccurate information online and given during telephone
conversations.
Community Groups & Referrals
•
It was a challenge - texting was best.
•
Each call gave me extra work – balance between them taking
responsibility and retaining control
Keeping in touch
I was labouring under the
misapprehension that no
one gave a damn, but now
I know there are people
out there that really care.
That first chat
made a big
difference
•
Link worker helped motivate participants, identify actions, navigate
bureaucracy & ensure referrals were acted on.
•
During follow up people are saying they haven’t done anything. They
are not recognising / valuing the changes they have made.
•
Cannot make people conform and fit in boxes and be expected to join
a group for the sake of it. Life is not that simple.
Reflections
Ppsif 2018-19
Feasibility study – mid-Wales – PPSIF 2018/19 FY
Study with PHW, RHCW, WARU-AU,
Social prescribing involves enabling primary care professionals to refer individuals to local non-clinical services, promoting a holistic approach to health management. This practice has gained recognition for its effectiveness in empowering individuals to take control of their own well-being. Initiatives like the National Academy for Social Prescribing and the National Loneliness Strategy aim to standardize and promote the benefits of social prescribing across the UK, emphasizing partnerships, evidence-based practices, and funding models. In Wales, efforts are being made to prioritize mental health support through schemes like Social Prescription to enhance overall mental health and well-being.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Social prescribing link worker intervention for health and well-being Mark Griffiths and Lucy Duncanson 6thNovember, 2019
What is social prescribing? Enabling primary care professionals to refer people to a range of local, non- clinical services using a holistic approach, supporting individuals to take control of their own health. King s Fund: Social Prescribing: coming of age ..what for many has seemed like common sense and beneficial is increasingly now scientifically proven and gaining traction in the medical world..
Is the number of GPs falling across the UK? Changes in number of GPs between 2016-2018; level of GP staffing, 2018
The National Academy for Social Prescribing will: Standardise social prescribing Increase awareness of the benefits Build and promote the evidence base Share best practice Look at funding models Create partnerships Develop training and accreditation
National Loneliness Strategy Government will support all local health and care systems to implement social prescribing connector schemes across the whole country, supporting the aim to have a universal national offer available in GP practices. It will also take steps to improve and share knowledge on effective social prescribing services. In addition, the Department of Health and Social Care, NHS England and the Department for Work and Pensions will commit to testing methods that will improve how a range of other organisations (such as community pharmacies, social workers, community nurses and jobcentres) refer into existing social prescribing services.
Social Prescribing in Wales: Theme: Healthy and active Wales Mental Health and Well-being Prioritise mental health treatment, support, prevention and de-escalation, including a pilot Social Prescription scheme and increase access to talking therapies
1,351,066 of funding to deliver two projects Mind Cymru: co-produce a link worker model for adults at risk of poor mental health in Taf Ely, South Powys and North Denbighshire British Red Cross: test two models for patients with mental health problems and are frequent attenders of GP or ambulance services in Pembrokeshire and Caerphilly.
Research proposal Objectives: Primary question: to what extent does the role of the link worker effect recruitment into, and retention in community-based social prescribing services. Secondary objectives: report health and well-being measures as an indicator of our population
Methodology Recruit 20 patients in the North Ceredigion GP clusters (7 GP practices, c. 47k population)
Methodology Recruit 20 patients in the North Ceredigion GP clusters (7 GP practices, c. 47k population) Participants interviewed by LW, complete Warwick-Edinburgh Mental Well-being Scale (WEMWBS)
Warwick-Edinburgh Mental Well-being Scale (WEMWBS) A validated 14 item questionnaire Likert scale 1-5 (cumulative score 14-70) Available in English and Welsh UK adult population norm c. score of 51
Methodology Recruit 20 patients in the North Ceredigion GP clusters (7 GP practices, c. 47k population) Participants interviewed by LW, complete WEMWBS Participants receive a health and well-being assessment Stature, mass - BMI Resting Blood Pressure Heart rate Participants agree a social prescription to follow for 3 months, meeting monthly with the link worker (LW) to discuss progress Repeat all health assessments after 3 month intervention Participation in a focus group meeting to discuss SP and LW role
Project plan w/c 2018 ACTIVITY May June July August September October November December 21 28 4 11 18 25 2 9 16 23 30 6 13 20 27 3 10 17 24 1 8 15 22 29 5 12 19 26 3 10 17 Preparatory work Networking Linking with GPs Development of resources Participant Engagement GP referrals Link Worker engaged with participants Active Research Initial Health / Wellbeing Assessments of participants Link Worker diary / lessons learnt log Final Health / Wellbeing Assessments GP online survey Focus group research
Initial Meeting With Participants 17 referrals 17 referrals - I met with 13 participants for up to 2hrs, Co-wrote a prescription of what they wanted to do. Participants can tell you anything. Support for link workers is vital supervision sessions. 13 Initial meeting 4 not available 1 withdrew 12 followed up Issues included: suicide attempts, serious miscarriage of justice, domestic violence, loneliness, anxiety, hording, rejection, post traumatic stress, harmful drinking, isolation, depression, bereavement 11 final meeting & measurements 1 not wanting final measurements
There were many unnecessary barriers to people joining groups. Many referrals had to be chased up. There was a lot of inaccurate information online and during telephone conversations.Participants were not kept informed or were unaware of when activities were starting or how long waiting lists were. Follow up is essential, and in some cases it took many months for the participants to be invited to join the activity.
Impact of engagement - What difference did it make in peoples lives What wouldn t have happened without the support of the social prescribing link worker Re joined cardiac rehabilitation Significantly Reduced harmful drinking Got a blue badge to help parking Increased walking Started exercise referral Quit smoking for 3 weeks Told something I haven't told anyone before Joined a woodland group Since meeting you things have gone from nowhere to top of the hill. I m living in hope at the moment. Found out about housing options in town Motivated to volunteer as hospital radio DJ I don t mix well with people. I was craving a social life. Registered as a carer, on waiting list for respite Given priority on social housing waiting list Received disability adaptations in the bathroom Helped me focus.. You look at the whole person Joined Foodwise for Life course Just talking and being listened to made the difference Receiving post traumatic stress counselling
Community Groups & Referrals Lack of awareness of groups on offer Participants require motivational support to link in with a new activity The role of a group leader in welcoming new members and helping them feel included is vital. This role should be paid. Referral follow up is essential. Many took months for the participants to be invited to join the activity Inaccurate information online and given during telephone conversations.
Keeping in touch It was a challenge - texting was best. Each call gave me extra work despite the fact I was encouraging participants to find their own solutions. I was labouring under the misapprehension that no one gave a damn, but now I know there are people out there that really care. That first chat made a big difference
What Worked Well Working knowledge and relationship with primary care Motivational Interviewing and Mental Health First Aid training Good local knowledge of groups and services locally. Written social prescription One referral leading to others. What Didn t Participants didn't really join groups. They were mainly referred into services. No referrals were received from Tregaron or Aberaeron GP surgeries. Five participants showed a keen interest in volunteering. Only one followed this through. It is really hard to navigate the system of life when you have had knockbacks, are lonely, or have been bereaved. There is no magic one size fits all solution. Social Prescribing Link Worker Challenges One participant joined a group which they really enjoyed, but felt lonelier afterwards. Most conversations with the participant resulted in more work for me People answering the phone. Waiting lists and being kept informed of services
Reflections A co-produced social prescription was useful Link worker helped motivate participants, identify actions, navigate bureaucracy & ensure referrals were acted on. During follow up people are saying they haven t done anything. They are not recognising / valuing the changes they have made. Paid, trained members of community groups are needed to welcome and support new members. Cannot make people conform and fit in boxes and be expected to join a group for the sake of it. Life is not that simple.
Results WEMWBS 60.0 No difference between baseline and at 3 months (37.9 38.5) Wide variance Range: (Baseline) = 16 62 after intervention = 14-65) 37.9 38.5 50.0 40.0 WEMWBS 30.0 20.0 10.0 0.0 Baseline 3 months
Results Weight and BMI No difference between baseline and at 3 months Ranges o Weight: 66.6-158.6kg o BMI: 27.0-47.1 kg/m2
Results Blood pressure and heart rate No difference between baseline and at 3 months
Lucy knew an awful lot about what was going on without having to look everything up... She seemed to know everyone and everything Focus Group Primary Objective: extent to which the link worker effects recruitment into and retention in social prescribing services? Perception of LW: Added value of local knowledge & ability to harass local community service providers LW as a therapeutic intervention (positivity and approachability) Identification of most appropriate activities and facilitate participation Participant s desire to please the LW It would be helpful for someone to accompany you, to go with you. To help break the ice and put your foot through the door I knew what I didn t want to do before project. It was just nice to have someone to speak to. Lucy is lovely.
Focus Group Primary Objective: extent to which the link worker effects recruitment into and retention in social prescribing services? More Link Workers I met Lucy in the Doctors. I wasn t able to get up here. Which made it easy for me. Getting up here is not that easy. We met at GP s which was great. down our own goals. I wanted to please which I could follow through with it. had forgotten about me, and then I heard from Lucy seventeen participants. That s a lot of work . I thought she was very helpful and positive. Then we had to write day before to remind of appointment. I thought the project was over and that Lucy Text was helpful- from Lucy the Meetings: Location/flexibility of LW meetings impacts participants in a rural community. Participants wanted more contact with LW and goal setting LW showing personal interest hard for one Link Worker to do job for That s where your money needs to go. Resourcing: More funding for LW role
Conclusions No differences in the physical and mental indicators of health weight, BMI, BP, resting HR and WEMWBS Demonstrated feasibility to collect these data Difficulties with getting participants into SP activities/schemes Engagement with healthcare professionals could be improved More research needed into recruitment and retention in mid-Wales Repeat and recruit specific patient population e.g. frequent attenders Longer intervention period
Recommendations Social prescribing as a concept is not well understood by the public. Better promotion of social prescribing and how to access services Integrating infrastructure e.g. single point of access IT system linking relevant databases with an up to date directory of services. scope out what is essential / desirable training for the LW role. Clinical/professional supervision outside of line management and structured peer-support sessions to help manage workload and patient demands.
Recommendations II Sustainability of social care services/community activities. Resourcing and accurate information about services and activities to ensure timely engagement and maintain individual s motivation Active LW engagement with GPs, social prescribing scheme providers and each other to help understand patient trends, service capacity/capability and promote engagement A randomised control trial to determine if social prescribing can deliver a return on investment.
Meet the team Mark Griffiths, PHW (mark.griffiths5@wales.nhs.uk) Laura Evans, PHW (laura.evans16@wales.nhs.uk) Lucy Duncanson, PHW (lucy.Duncanson@wales.nhs.uk) Anna Prytherch, RHCW (Anna.L.Prytherch@wales.nhs.uk) Rhys Thatcher WARU, AU (ryt@aber.ac.uk) Ceri Smith, PHW (ceri.smith3@wales.nhs.uk)
LW Lucy introducing Lucy s slide set Lucy could mention o principal research question ie to what extent does the role of the link worker effect engagement with and adherence to community-based social prescribing services o Recruitment at which surgeries / or how many of the 7 surgeries were able to support, speed of recruitment etc o How many retained, how many lost o Experiences of participants in attending meetings, follow ups, o Attitudes toward social prescribing, willingness to participate o Lessons learned o Pin board on next slide
GP, Practice Manager and Health Professional Survey Social Prescribing Short, online survey (13 questions) Shared with staff in Ceredigion GP cluster 3 follow ups 1 response Indicative of time pressures within primary care
Initial Meeting With Participants 17 referrals 17 referrals I met with each of the 13 participants for up to 2hrs, Co-wrote a prescription of what they wanted to do. Missed appointments: 19. Participants can tell you anything. Support for link workers is vital supervision sessions. 13 Initial meeting 4 not available 1 withdrew 12 followed up 11 final meeting & measurements 1 not wanting final measurements
Groups, activities & services
Community Groups & Referrals Lack of awareness of groups on offer Participants require motivational support to link in with a new activity The role of a group leader in welcoming new members and helping them feel included is vital. This role should be paid. Referral follow up is essential. Many took months for the participants to be invited to join the activity Inaccurate information online and given during telephone conversations.
Keeping in touch It was a challenge - texting was best. Each call gave me extra work balance between them taking responsibility and retaining control I was labouring under the misapprehension that no one gave a damn, but now I know there are people out there that really care. That first chat made a big difference
Reflections Link worker helped motivate participants, identify actions, navigate bureaucracy & ensure referrals were acted on. During follow up people are saying they haven t done anything. They are not recognising / valuing the changes they have made. Cannot make people conform and fit in boxes and be expected to join a group for the sake of it. Life is not that simple.