Understanding Opioid Use Disorder and Treatment Options
This presentation delves into the complexities of Opioid Use Disorder (OUD), discussing its impact on the neuroendocrine system, treatment options, including Medications for Opioid Use Disorder (MOUD), and special populations. The objective is to connect endogenous mechanisms to clinical observations, view OUD as a disease state, and explore various treatment methods along with their adverse effects and contraindications. Insights into the effects on dopamine and norepinephrine systems are provided, aiding in comprehending the significance of addressing OUD. Key slides highlight pertinent information from past studies, reinforcing the urgency of understanding and managing OUD effectively.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Opioid Use Disorder and Treatment Farinaz Khan, Paul Romo, MD
Disclosure None
Outline Opioids and the Neuroendocrine system Misuse and Addiction Treatment Special Populations- forensics
Objective By the end of this didactic, you will be able to: Connect endogenous mechanisms to clinical observations Understand OUD as a disease state Discuss treatment options for MOUD including adverse effects and contraindications.
Opioid effects on DA and NE systems Peptide families: endorphin, enkephalin, dynorphins Receptors: Mu, Delta, Kappa Mu most robust for clinically active opioids Exogenous opioids impact the same system(s) Down stream effects on dopamine (DA) and Norepinephrine (NE)
LC area (anxiety, activation)
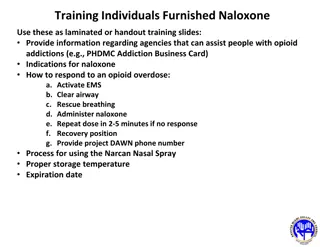
LC area (anxiety, activation) NALXONE RESCUE KIT
Past Year Initiates for Specific Illicit Drugs among Persons Aged 12 or Older: 2007 Numbers (in Thousands) 2,500 2,147 2,090 2,000 1,500 1,232 906 1,000 781 775 642 554 500 270 198 106 0 Marijuana Cocaine Inhalants Sedatives Pain Relievers Tranquilizers Ecstasy Stimulants LSD Heroin
People Aged 12 or Older with a Past Year Substance Use Disorder (SUD): 2018 FFR1.42 Rx = prescription. Note: The estimated numbers of people with substance use disorders are not mutually exclusive because people could have use disorders for more than one substance.
ADDICTION AS A DISEASE MODEL
ASAM Definition of Addiction A primary, chronic disease of brain reward, motivation, memory and related circuitry. Dysfunction in these circuits leads to characteristic biological, psychological, social, and spiritual manifestations. This is reflected in an individual pathologically pursuing reward and/or relief by substance use and other behaviors. http://www.asam.org/DefinitionofAddiction-LongVersion.html
Opioid use D/O DSMV Moderate 4-5 Mild 2-3 Severe >6 Remission Early 3-12mo, Sustained >12mo Specifiers: maintenance therapy or controlled environment Note: withdrawal and tolerance
SUD Criteria Substance is often taken in larger amounts or over a longer period than was intended. There is a persistent desire or unsuccessful efforts to cut down or control use. A great deal of time is spent in activities necessary to obtain, use, or recover from its effects. Craving, or a strong desire or urge to use substance. Recurrent substance use resulting in a failure to fulfill major role obligations at work, school, or home. Withdrawal Tolerance
SUD Criteria Continued substance use despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the effects of the substance. Important social, occupational, or recreational activities are given up or reduced because of substance use. Recurrent substance use in situations in which it is physically hazardous. Substance use is continued despite knowledge of having a persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by the substance.
Opioid Use D/O Treatment Behavioral interventions have poor outcomes Controlled environment Medication assisted detoxification poor outcomes N.A. These forms of treatment or lack of, have higher associated risk or relapse, OD, recidivism, crime, infection, death (Bart, 2012)
Opioid Withdrawal Nausea Vomiting Abdominal cramping Diarrhea Muscle aches Runny nose Sweating Tachycardia Increased tearing Insomnia Yawning Dilated pupils Goose bumps Agitation Anxiety
Opioid W/D vs Influenza Opioid w/d Influenza Nausea/ Vomiting Abdominal cramping Diarrhea Muscle aches Runny nose Sweating Increased tearing Insomnia Yawning Dilated pupils Goose bumps Agitation Anxiety Vomiting Diarrhea Muscle or body aches Runny or stuffy nose Fever* or feeling feverish/chills Cough Sore throat Headaches Fatigue (tiredness)
Opioid W/D kick kit NSAIDS Clonidine Muscle relaxant Antiemetic Imodium
Maintenance Medications FDA approved for long term treatment: Methadone (MTD)-opioid agonist Buprenorphine (BUP)-partial agonist Naltrexone (NTX)-opioid antagonist Office based and clinic based
MAT as Detox Agent >90% of patients relapse within 2 months of taper 95% of methadone patients will relapse within 1 year after d/c Nosyk, 2013, Weiss, 2011
Adverse Effects and Contraindications Hepatic-Hepatitis and Decreased Function (monitor LFTS) Cardiac- QTC prolongation CNS-sedative effects or paradoxical effects GI- constipation and secondary morbidity
Side Effects and Contraindications Drug-Drug interactions (i.e. benzodiazepines) QTC prolongation (i.e. antihistamines, antidepressants, antibiotics, antifungals) Inhibition (i.e. Seroquel) Induction (i.e. Dilantin)
Switching Classes of FDA approved treatments Naltrexone Buprenorphine Methadone (reduced efficacy initially) No risk of precipitating withdrawal
Switching Classes of FDA approved treatments Methadone Buprenorphine Naltrexone Risk of precipitating withdrawal Wash out period is longer for bup and methadone
Special Populations Adolescents Geriatrics Pregnant Women LBGTQ Forensics
Addiction and Crime US has highest incarceration rate Costly 1.7 trillion (Anderson, 2011) 1/100 adults may be incarcerated in life time, higher for minorities (Warren, 2008)
SUD and crime highly correlated 50% cases (Nunn 2009) Nearly 1/4 of inmates in DOC report heroin use (Karberg 2016) OUD correlated with other poor outcomes such as HIV transmission, crime, recidivism, opioid toxicities and deaths (Rudd 2016) Risk of OD 13x greater for parolees within first 2 weeks after release In England, risk documented 29x higher than those without OUD (Binswanger, 2013, (Merrall, 2010)
Intervention Points Contact with EMS services including Law Enforcement Drug Court Pretrial Services
Intervention Points Intra system programs and treatment Release and post incarceration services UNM Jail Diversion Services, JDS
Treatment MOUDs reduce drug use and criminality (Perry 2014) MOUDs reduce post release drug use and crime (Schwartz 2017) Benefits extend out 12months following release after incarceration according to RCT (Kinlock 2009) Despite data, MOUDs are rarely implemented in the criminal justice system
Other treatment modalities Naloxone rescue kit distribution upon d/c Naltrexone and Vivitrol Suboxone 12 step groups Individual and Group Counseling ATP, mimics an IOP
Outline Opioids and the Neuroendocrine system Misuse and Addiction Treatment Special Populations- forensics









")
")
")






























")
")