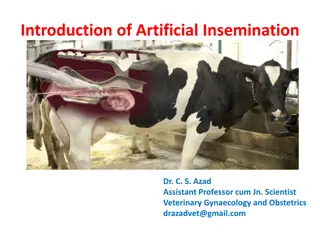
Understanding Artificial Insemination and New Technologies for Fertility

Assisted Reproductive Technology (ART) offers various methods like artificial insemination using husband's semen (AIH) or donor sperm (AID), split ejaculate method, and more to help couples facing infertility. These technologies aim to address factors like male infertility, anatomical defects, and genetic disorders, providing options such as intra-uterine insemination (IUI) and sperm intra-fallopian transfer (SIFT). Considerations such as sperm quality, storage, and regulatory standards play crucial roles in these processes.
- Artificial Insemination
- Fertility Treatment
- Assisted Reproductive Technology
- Male Infertility
- Sperm Donation

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Assissted Reproductive Technology (ART) Artificial insemination (AI) Male infertility factors Inject the sperm directly in the female reproductive tract (why) Artificial insemination is intra-vaginal or intra- cervical injection/transfer facilitate fertilization of semen to
AIH: Artificial insemination using husbands semen AID: Artificial insemination using donor s semen IUI: Intra-uterine insemination SIFT: Sperm intra-fallopian transfer DIPI: Direct intra-peritonial insemination
Artificial Insemination using husbands Semen (AIH) Oligospermia Anatomical defects in male reproductive system Centrifugation-concentration of sperms in the semen Accumulation using deep freeze storage
Split Ejaculate Method During ejaculation the semen comes in two or three fractions The first half ejaculate contains spermatozoa; also the sperm quality in terms of motility and morphology is better than the one ejaculated in later half Substances such as kalikrein, arginine or albumin improve motility of sperms in the split ejaculate Cleaning of ejaculate to obtain large number of live and motile sperms majority of
Artificial insemination using donors semen (AID) Husband asthenospermic or severely oligospermic Donor sperms- sperm banks Collection, storage by freezing the sperms from anonymous donors Strict guidelines and regulatory standards for donor selection, cryopreservation and semen banking Confidentiality Testing of semen for any microbiological contamination Azoospermic or nacrospermic or
Artificial Insemination by Donor Sperm AID Many women use donor insemination procedure If male partner s sperm is of poor quality or quantity Some men with genetic disorders may choose AID so they don t pass on genetic disorders to their children Using a sperm donor is also a choice for single women or lesbian couples Before proceeding with donor sperm and the artificial insemination procedure, doctor may encourage to speak to a counselor about any anxieties or concerns. sperm with the artificial
Procedure of Ovarian hyper- stimulation The stimulation is to correct subtle cycle disorders, to increase the number of available oocytes for fertilization and to improve the timing of insemination aim of controlled ovarian hyper-
Procedure of Ovarian hyper- stimulation The two most frequently used drugs are clomiphene citrate and gonadotropins Clomiphene citrate receptors of the hypothalamus This altered feedback information causes the hypothalamus to make and release more gonadotropin releasing hormone (GnRH) This in turn causes the pituitary to make and release more FSH and LH blocks the estrogen
Gonadotropins The gonadotropins Follicle Stimulating Hormone (FSH) and Luteinizing Hormone (LH) are released under the control of gonadotropin-releasing hormone (GnRH) produced in the hypothalamus. FSH maturation granulosa cells of ovarian follicles directly affects follicles the production stimulating and the of by LH stimulates the thecal cells to produce testosterone (and indirectly estradiol)
Gonadotropins LH surge is obligatory for the rupture of the dominant follicle The first FSH preparation used in fertility practice was extracted from (human menopausal gonadotropin, hMG) postmenopausal urine In the 1990s, recombinant DNA technology led to the development and clinical introduction of human recombinant FSH (rFSH).
Monitoring, Timing, and/or Induction of Ovulation In IUI cycles with ovarian hyperstimulation the follicular growth is sonography, since uncontrolled multifollicular growth may lead to (high order) multiple pregnancies always monitored by For the detection of ovulation, either LH-surge tests can be used or ovulation can be induced by human chorionic gonadotropin (hCG).
Intra-uterine Insemination Most insemination It makes the trip shorter for the sperm and gets around any obstructions The sperms escape the unreceptive cervical mucus common method of artificial
IUI The success of IUI is based on three steps Firstly, semen is processed, so that spermatozoa are concentrated in a small volume and the number of motile sperms is increased at the site of fertilization Secondly, the insemination takes place directly, bypassing the possibly hostile cervical mucus and bringing the semen in closer proximity of the oocyte Thirdly, optimizing the timing by monitoring or inducing ovulation All these steps increase the probability of conception, especially in the case of compromised semen parameters motile
Preparing the Sperm In special washing and processing procedure After a semen sample is obtained, the sperm are washed and concentrated A semen sample is washed in the lab to separate the sperms from the seminal fluid During this washing and processing phase, potentially toxic chemicals are removed, along with a seminal plasma that surrounds each sperm cell IUI the sperm sample undergoes a
Under normal circumstances, sperm must pass through the cervical mucus to reach the uterus, a process that limits uterine entrance to only the healthiest sperm and prevents dead sperm, debris, and seminal fluid from getting in Due to the presence of prostaglandins and microbes in the seminal fluid, semen cannot be placed directly into the uterus without the potential of inducing painful cramping and infection During sperm preparation seminal fluids, nonmotile cells, and debris are removed, sperm can be placed directly into the uterus
Besides removing prostaglandins, processing semen samples prior to IUI has other advantages Sperm from semen samples can be concentrated and reduced to a volume that is consistent with what the uterine cavity can hold Decapacitation factors present in the semen are removed, increasing the sperm s fertilization ability Processing semen samples can also select for fractions of sperm with the best motility and improve overall motility The prepared sample of sperm can be placed in preparation media known to support sperm capacitation and survival
Basic Wash The basic wash is the simplest and least expensive sperm preparation to perform. It is able to concentrate the sperm into a workable volume for insemination, removing the seminal fluid with its associated decapacitation factors and prostaglandins Besides its simplicity, the advantage of a basic wash is that essentially all of the sperm in the ejaculate will be recovered This concentration of motile sperm. It is also beneficial for cryopreserved samples, or other fragile samples that would benefit from reduced processing and increased recovery is especially useful for samples with a low
Basic Wash The disadvantage of a basic wash is that it concentrates all of the live sperm, dead sperm, white blood cells, red blood cells and seminal debris together. As a result, the healthy sperm are exposed to higher levels of reactive oxygen species (ROS), which function and negatively affect fertilization can decrease sperm Therefore, the basic wash is not recommended for regular samples when there are a lot of cellular contaminants or dead cells present
Density Gradient Preparation The density gradient preparation consists of filtering sperm by centrifugal force through either one or multiple concentrated silane-coated silica particles layers of increasingly Typically, semen is placed directly on top of the density gradient layers. During centrifugation, the most motile sperm pass through the different layers, making a soft pellet at the bottom. The seminal fluids, dead or nonmotile sperm, and cellular debris are held up at the interfaces between the layers
Density Gradient Preparation The sperm that have successfully pelleted at the bottom can then be recovered, washed to remove the density gradient media, and used for IUI. The ability to select for a population of clean, motile sperm makes it very useful for samples with a lot of dead sperm, round cells, or debris Unless it is necessary to remove WBCs, it is not advisable to use density gradient preparations for samples with low concentrations of progressively motile sperm, as recovery may be limited
Preparation of Cryopreserved Sperm Patient Samples In many cryopreserved chemotherapy or military duty, or for other personal reasons. instances, sperm patients that choose stored to prior use to was As cryopreserved sperm are less robust than those in fresh samples, extra precaution should be taken when they are prepared Generally, cryopreserved samples should not be subjected to more than a single wash in sperm wash media
Preparation of Cryopreserved Sperm The centrifugation time should also be reduced to 6 8 min Patients should be educated that cryopreserved samples will have reduced compared to the fresh state of the sample before freezing sperm motility Depending on the circumstances and the number of frozen vials a patient has stored, a plan should be made to thaw a sufficient number of vials to give the patients a reasonable chance of achieving pregnancy.
Preparation of Cryopreserved Sperm Donor Samples Many patients now choose to take advantage of the easy access to sperm donor profiles provided by the Internet and order donor sperm from sperm banks across the country The sperm samples are typically shipped just prior to their anticipated use If the sample is not going to be used right away, measures should be taken to place it in a more permanent storage container
Preparation of Cryopreserved Sperm Most sperm banks are now providing donor samples that are prewashed. Under these circumstances, all that is necessary is to thaw the vial, check a drop of the warmed sample to confirm if it meets the sperm bank s standards, and load it into the insemination syringe If the sample was not washed prior to freezing, it will be necessary to wash the sample using the simple wash procedure, shortened to 6 8 min of centrifugation, prior to intrauterine insemination
The IUI procedure is performed around the time of ovulation, typically about 24-36 hours after the surge in LH hormone that indicates ovulation will occur soon A catheter directly into the uterus is used to insert the sperm This process maximizes the number of sperm cells that are placed in the uterus, thus increasing the possibility of conception
Modalities of Insemination IUI is commonly performed between 36 and 42 h after a positive LH surge test IUI 33 or 39h after the administration of hCG resulted in the same pregnancy results, and therefore the timing of the insemination may depend on local convenience of the hospital Insemination has to be performed only once per cycle A 10-min interval of bed rest after IUI has a positive effect on the pregnancy
Intra-tubal insemination Intra-tubal insemination (ITI) involves injection of washed sperm into the fallopian tube, although this procedure is no longer generally regarded as having any beneficial effect compared with IUI ITI is different from gamete intra-fallopian transfer, where both eggs and sperm are mixed outside the woman's body and then immediately inserted into the fallopian tube where fertilization takes place.
Direct intraperitoneal insemination (DIPI) The sperms are injected into the lower abdomen through a surgical hole or incision, with the intention of letting them find the oocyte at the ovary or after entering the genital tract through the ostium of the fallopian tube
Intra-uterine Tuboperitoneal Insemination (IUTPI) Intrauterine insemination injection of washed sperm into both the uterus and fallopian tubes The cervix is then clamped to prevent leakage to the vagina The sperms are mixed to create a volume of 10 ml, sufficient to fill the uterine cavity pass through the interstitial part of the tubes and the ampulla, the peritoneal cavity and the Pouch of Douglas tuboperitoneal (IUTPI) involves finally reaching
Intra-uterine Tuboperitoneal Insemination (IUTPI) IUTPI can be useful in unexplained infertility, mild or moderate male infertility, and mild or moderate endometriosis In non-tubal sub fertility, fallopian tube sperm perfusion may be the preferred technique over intrauterine insemination