A Journey to Reduce Missed Abusive Head Trauma: From Index Case to Cluster Randomized Trial
Abusive head trauma (AHT) is a significant cause of trauma-related death and disability in young children. The journey to address missed cases of AHT began with the index case in 1995, leading to a cluster randomized trial aiming to improve recognition and prevention. The consequences of missed AHT cases include reinjury, medical complications, and even death. Early recognition is crucial to preventing further harm. Research funding from various sources has supported efforts to reduce missed diagnoses and improve outcomes in AHT cases.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
From Index Case to Cluster Randomized Trial: A Journey to Reduce Missed Abusive Head Trauma Kent P. Hymel, MD Professor of Pediatrics, Penn State College of Medicine Child Abuse Pediatrician, Penn State Health Children s Hospital For the Pediatric Brain injury Research Network (PediBIRN) Investigators
Disclosures Consultant/ Speakers bureaus No Disclosures Research funding This research has been supported by Dartmouth-Hitchcock Medical Center, a private family foundation, The Gerber Foundation, Penn State Children s Hospital, and the Child Maltreatment Solutions Network at Penn State University. Funding to support our cluster randomized trial was provided by NICHD (grant number P50HD089922). Stock ownership/Corporate boards-employment No Disclosures Off-label uses No Disclosures
Background Abusive head trauma (AHT) is the leading cause of traumatic death and disability in early childhood. The estimated annual incidence of AHT is 20-30 cases per 100,000 children <2 years of age. Unfortunately, physicians continue to miss this diagnosis, putting patients at risk for repetitive abuse and even death.
The index case In March 1995, Dr. Carole Jenny examined a 14-month-old boy who had sustained AHT 4 months previously. Over the next 4 months, the child had been seen by 7 physicians and had undergone 2 cranial imaging studies. At each visit, the diagnosis of AHT was not recognized. When Dr. Jenny examined him, he had multiple old and new fractures and healing brain injuries.
Background Dr. Jenny s experience with this patient triggered an immediate plan to study missed cases of AHT. Our subsequent, single institutional study found that AHT was missed in 54 (31%) of 173 patients when they first presented for medical evaluation of symptoms ultimately attributable to their AHT.
Background Of the 54 patients with missed or unrecognized AHT 15 (28%) were reinjured after their missed diagnosis, 22 (41%) experienced medical complications related to the missed diagnosis, and 5 (9%) died. 4 of the 5 deaths among patients with unrecognized AHT might have been prevented by earlier recognition of their abuse.
Background In a more recent multicenter study published in 2016, Letson and colleagues reported that More than 10 years after our single institutional study, we were still missing 31% of cases.
Presentation objectives To tell the story of our sustained research effort to reduce cases of missed or unrecognized abusive head trauma (AHT) To review evidence-based approaches to medical screening and diagnosis To describe and demonstrate the steps required to develop a clinical prediction or decision rule (CPR or CDR) To present the results of a cluster randomized trial of a CDR designed to function as an effective AHT screening tool
Evidence-based approaches to medical diagnosis and screening
Evidence-based diagnosis and screening evidence-based medicine acknowledges that intuition, unsystematic clinical experience, and pathophysiologic rationale are insufficient grounds for clinical decision making, and it stresses the examination of evidence from clinical research. Dr. Guyatt and the other members of the original Evidence- based Medicine working group
Evidence-based diagnosis and screening For simple and/or common conditions, diagnosis results from pattern recognition. For more challenging or less familiar conditions, when pattern recognition fails, clinicians use a probabilistic approach for medical diagnosis.
Probabilistic diagnostic reasoning We conduct an initial clinical assessment, generate a list of potential diagnoses, and The pre probability The pre- -test probability test estimate the probability associated with each diagnosis. Thereafter, we conduct one or more diagnostic investigations (e.g., we might capture additional history, complete a more focused physical examination, order laboratory tests, or complete radiological studies). Finally, we interpret the results of these diagnostic investigations to The post- -test probability The post probability test increase or decrease the diagnostic probabilities, until we are sufficiently confident in our diagnosis that we initiate appropriate treatment.
Evidence-based diagnosis and screening In the absence of any other patient-specific information, disease prevalence in the population is a reasonable estimate of pre-test probability. Probability of Diagnosis Pre-test probability Pre-test probability Pre-test probability Treatment threshold ? ? Test ? ? 100% 0% threshold Probability below test threshold. Diagnosis effectively excluded. No testing warranted. Probability between test and treatment threshold. Diagnosis neither confirmed or excluded. Further testing warranted. Probability above treatment threshold. Diagnosis effectively confirmed. No further testing required. Treatment commences.
Evidence-based diagnosis and screening Some clinical findings or results, when positive, shift probability upward greatly, but change it little when negative. Other findings are more useful when negative, because some negative findings virtually exclude the diagnosis, whereas the positive finding increases probability only slightly.
Evidence-based diagnosis and screening What two specific qualities of a clinical finding or test best describe its effect on the probability of a diagnosis? Sensitivity and Specificity
Evidence-based diagnosis and screening Condition Present A C A+C Condition Present Condition Absent B D B+D Condition Absent TOTALS A+B C+D A+B+C+D TOTALS Finding present Finding absent TOTALS Sensitivity is defined as the proportion of patients with the condition who have the clinical finding [SENS=(A)/(A+C)]. A finding (or test) with high sensitivity is useful to help exclude a diagnosis when negative, because a highly sensitive test will render few results that are falsely negative.
Evidence-based diagnosis and screening Condition Present A C A+C Condition Present Condition Absent B D B+D Condition Absent TOTALS A+B C+D A+B+C+D TOTALS Finding present Finding absent TOTALS Specificity is defined as the proportion of patients without the condition who don t have the clinical finding [SPEC=(D)/(B+D)]. A finding (or test) with high specificity is useful to help confirm a diagnosis when positive, because a highly specific test will render few results that are falsely positive.
Evidence-based diagnosis and screening Highly sensitive findings or tests make good screening tests. Highly specific findings or tests make good confirmatory tests.
Evidence-based diagnosis and screening A likelihood ratio (LR) incorporates both sensitivity and specificity to describe the overall discriminatory power of a clinical finding. The positive likelihood ratio [SENS/(1-SPEC)] describes changes in the probability of a diagnosis if the clinical finding is present. The negative likelihood ratio [(1-SENS)/SPEC] describes changes in the probability of a diagnosis if the clinical finding is absent.
Evidence-based diagnosis and screening The advantage of likelihood ratios is how simply they can be used to estimate the post-test probability of a diagnosis. For example LRs of 2, 5 and 10 increase probability approximately 15%, 30% and 45%, respectively; and LRs of 0.5, 0.2, and 0.1 decreaseprobability approximately 15%, 30% and 45%, respectively.
How do we calculate post-test probabilities using likelihood ratios? Conduct Clinical Research We apply Bayes theorem. Calculate Disease Prevalence Measure the Sensitivity and Specificity of Specific Findings and Tests Pre-test Probability Likelihood Ratio Post-test Odds Pre-test Odds X = Post-test Probability
Evidence-based diagnosis and screening Probability of Diagnosis Probability of Diagnosis As illustrated by this example, initial estimation of pre-test probability effects the need for additional testing. LR- LR+ Finding absent or test negative Finding present or test positive Treatment threshold Test 100% 0% threshold Pre-test probability Post-test probability below test threshold. Diagnosis effectively excluded. No further testing warranted. Post-test probability below treatment threshold. Diagnosis remains unconfirmed. Further testing warranted.
Clinical prediction and decision rules A clinical prediction rule (CPR) is an evidence-based tool that measures and then combines the predictive contributions of multiple clinical findings or test results to estimate or predict the probability of a diagnosis, prognosis or response to therapy for an individual patient.
Clinical prediction and decision rules A CPR that is used to direct a specific, difficult, clinical decision is frequently referred to as a clinical decision rule (CDR). To clarify the distinction Clinical prediction rules are developed to inform a specific, difficult, clinical decision. They typically provide an estimate of probability. Clinical decision rules are developed to direct a specific, difficult, clinical decision. They usually recommend or direct a specific clinical action.
Clinical prediction and decision rules If your primary reason for developing a CPR is to avoid over- diagnosis, then develop a rule with maximum diagnostic specificity to help confirm the diagnosis, when positive.
Clinical prediction and decision rules LR+ LR+ LR+ Positive or Present Treatment threshold 100% 0% Pre-test probability What combination of discriminating and reliable findings or tests will predictably increase probability above the treatment threshold, when positive or present?
Clinical prediction and decision rules If your primary reason for developing a CPR is to avoid under- diagnosis, then develop a rule with maximum diagnostic sensitivity to help miss fewer cases, and to help exclude the diagnosis, when negative.
Clinical prediction and decision rules LR- LR- LR- Negative or Absent Test 100% 0% threshold Pre-test probability What combination of discriminating, reliable and sensitive findings or tests will predictably decrease probability below the test threshold, when negative or absent?
Can we develop a clinical prediction or decision rule for AHT?
A clinical prediction rule for AHT? Probability of Diagnosis Pre-test probability Pre-test probability Pre-test probability Abuse suspicion threshold Abuse exclusion threshold Treatment threshold Test 100% 0% threshold Probability below the abuse exclusion threshold. Abuse reasonably excluded. Abuse evaluation highly likely to be negative. Probability between the abuse exclusion and suspicion thresholds. Apply the rule! Pre-test probability above the abuse suspicion threshold. CPS referral indicated.
A clinical prediction rule for AHT? Probability of Diagnosis To cast a sufficiently wide net, we hoped to develop a CDR that would direct physicians to conduct thorough abuse evaluations on all patients who present with any 1 or more of its predictor variables. LR- LR- LR- LR- 100% 0% What combination of discriminating, reliable and sensitive findings available at or near the time of hospital admission will predictably decrease the probability of abuse to the lowest level possible, when negative or absent? Abuse exclusion threshold
The pediatric brain injury research network (PediBIRN) was born
PediBIRNs overall research goals To derive, validate, implement, and disseminate an effective clinical decision rule (CDR) for pediatric AHT that Is simple and reliable Can be applied at or near the time of hospital admission Will function as an effective AHT screening test Is highly sensitive, to help clinicians miss fewer cases and exclude AHT, when negative Can facilitate calculation of evidence-based, patient-specific estimates of the probability of abuse Can inform or direct clinicians early decisions to either launch or to forgo an evaluation for abuse Reduces cases of missed AHT.
PediBIRNs overall research goals By established convention, the development of any clinical prediction or decision rule proceeds in 3 sequential phases The creation or derivation of the rule The testing or validation of the rule s performance The implementation of the rule in active clinical settings to assess its actual impact on relevant clinical outcomes the impact analysis Each phase requires a multicenter study.
Our derivation study Focusing exclusively on the PICU setting, we Conducted a prospective, strictly observational, multicenter, cross-sectional study across 14 U.S. academic medical centers; Captured extensive data regarding 209 acutely head injured children <3 years admitted for intensive care (excluding victims of MVAs and patients with pre-existing CNS abnormalities); and Applied a priori definitional criteria to sort patients into comparative groups of abusive (AHT) vs. other head trauma (non- AHT).
Our derivation study Next, from a list of 45 candidate variables, we Identified 13 early variables available at or near the time of PICU admission that were both discriminating (P <.05) and reliable (Kappa >0.6); and Calculated each variable s predictive qualities (i.e., sensitivity, specificity, LRs). Finally, we Applied recursive partitioning, and Identified four candidate clusters of these early, discriminating and reliable variables that alone or in combination demonstrated high sensitivity (>92%) to detect AHT in PICU settings.
Our derivation study Ultimately, we decided that a 4-variable CDR demonstrated the optimal qualities that define an effective screening tool, including High sensitivity Low false negatives High true negatives Simplicity High inter-rater reliability Acceptability to physicians
The PediBIRN-4 decision rule for AHT To minimize missed cases, every acutely head-injured infant or young child hospitalized for intensive care who presents with one or more of these 4 predictor variables should be considered to be at higher risk and thoroughly evaluated for abuse. Any clinically-significant respiratory compromise at the scene of injury, during transport, in the ED, or prior to admission Any bruising involving the child s ear(s), neck or torso Any subdural hemorrhage(s) or fluid collection(s) that are bilateral OR involve the interhemispheric space Any complex skull fracture(s) [NOTE: The PediBIRN-4 makes no recommendations regarding abuse evaluations in the remaining lower risk patients.]
The Four Bs Stated more simply, we were going to ask physicians to look for specific abnormalities in Breathing Bruising Bleeding Bone And to complete thorough evaluations for abuse if any one or more of these findings were present.
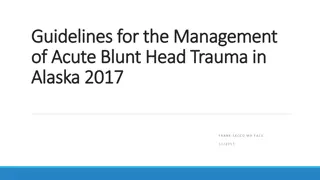
Our derivation study (N=209) 1.0 0.9 0.8 Defining abuse 0.7 Using original criteria 0.6 Using physicians' final diagnoses 0.5 As a positive partial or complete abuse evaluation 0.4 0.3 0.2 0.1 0.0 SENS SPEC NPV LR- NPTP False Negatives True Negatives
Our validation study Applying precisely the same inclusion/exclusion criteria and methods, in a new, larger, population of young, acutely head-injured infants and young children, hospitalized for intensive care across 14 PICU sites, the PediBIRN-4 CDR demonstrated AHT screening performance that was equal to or higher than its screening performance in our completed derivation study.
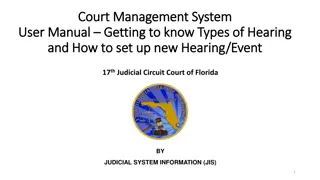
Our validation study (N=291) 1.0 0.9 0.8 0.7 Using original criteria 0.6 Using physicians' final diagnoses 0.5 As a positive partial or complete abuse evaluation 0.4 0.3 0.2 0.1 0.0 SENS SPEC NPV LR- NPTP False Negatives True Negatives
Applied as a prediction tool Applied as a prediction tool, rather than decision rule The PediBIRN-4 s evidence-based, patient-specific estimates of abuse probability Correlate positively and strongly with the overall diagnostic yield of patients completed skeletal surveys and retinal examinations.
Applied as a prediction tool (N=500) Variables in the AHT CPR Present on Admission Abusive Head Trauma 8 Nonabusive Head Trauma 2 Estimated Probability of Abuse 80% Unique Patient Subpopulation 1 A B C D (n) 10 + + + + 37 3 93% 2 + + + - 40 1 0 100% 3 + + - + 1 10 2 83% 4 + + - - 12 9 15 38% 5 + - + + 24 49 15 77% 6 + - + - 64 1 17 6% 7 + - - + 18 8 14 36% 8 + - - - 22 5 0 100% 9 - + + + 5 17 3 85% 10 - + + - 20 3 3 50% 11 - + - + 6 7 4 64% 12 - + - - 11 3 10 23% 13 - - + + 13 45 23 66% 14 - - + - 68 7 58 11% 15 - - - + 65 210 169 55% (1 through 15) 379 9 112 7% 16 - - - - 121
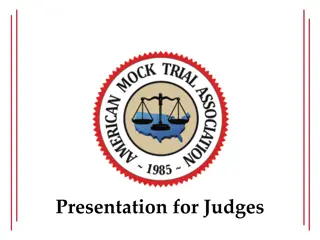
Applied as a prediction tool (N=500) 100% 90% 80% Overall Diagnostic Yields 70% 60% 50% 40% 30% 20% (Pearson sR=0.946) 10% 0% 0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 Estimates of Abuse Probability 16 subpopulations (Pearson's R=0.708) 5 subpopulations (Pearson's R=0.996)
Background If applied accurately and consistently, the PediBIRN-4 CDR should perform with 96% sensitivity. Though promising, some physicians will reject the CDR s application as an AHT screening tool and/or its recommendations. Thus, the CDR s actual clinical impact will be less than its potential impact.
Trial objective To apply the rigor of a cluster randomized trial to assess the PediBIRN-4 decision rule s actual impact on missed AHT when applied in active PICU settings.
Participants Trial participants were Eight PICUs in U.S. academic medical centers, divided into 2 clusters (4 intervention, 4 control), Their licensed and credentialed PICU and child abuse pediatric (CAP) physicians, and Their consecutive, acutely head-injured patients under 3 years of age admitted for intensive care. [NOTE: Victims of motor vehicle accidents and patients with preexisting intracranial abnormalities were excluded.]
Randomization and stratification Participating PICUs were drawn from prior PediBIRN studies and matched into 4 pairs based on projected patient volumes. A senior biostatistician randomized 1 PICU from each pair to the intervention arm. Randomization sequences were concealed from a second biostatistician responsible for analysis.
Implementation strategies (4 intervention sites) Initial online training Monthly booster training emails (x32) Coordinator prompts to physicians to apply the rule Decision rule badge cards Access to an AHT probability calculator Progress reports (every 6 months x4) comparing AHT evaluation practices and provider engagement across the 4 intervention sites Local information sharing sessions (every 6 months x4) to discuss local barriers to decision rule acceptance and utilization.







































")

")

")
")




")