Understanding Dementia: A Comprehensive Overview for Healthcare Providers

Age Friendly Primary Care: a Partnership
between OneWorld and UNMC’s Geriatrics
Workforce Enhancement Program
•
This program is supported by the Health
Resources and Services Administration (HRSA)
of the U.S. Department of Health and Human
Services (HHS) as part of an award totaling
749,926.00 with 0% financed with non-
governmental sources. The contents are those
of the author(s) and do not necessarily
represent the official views of, nor an
endorsement, by HRSA, HHS, or the U.S.
Government. For more information, please visit
HRSA.gov.
O
b
j
e
c
t
i
v
e
s
:
•
Understand essential elements of history in the diagnosis and
differential diagnosis of dementia.
•
Describe how members of the
interprofessional team
work together
in evaluation and management of dementia.
•
Recognize dementia as a
geriatric syndrome
with different factors
contributing SOME of which can either be improved or where we
can go to help patients compensate.
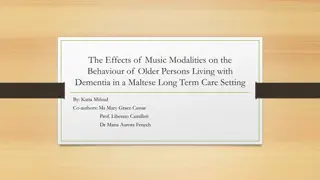
DEMENTIA:
History
Physical and
Social Networks
Etiology
Pathogenesis
Presenting
Symptoms
Disease
Geriatric
Syndrome
KNOWN
KNOWN
KNOWN,
but
variable
presentation
Factor 1
Factor3
Factor 2
Factor4
Interacting
Interacting
Interacting
Interacting
Single
Manifestation
DEMENTIA
•
The most common
cause of disability in
later life
•
A focus for providers
of health care to
older adults
Dementia
•
D
e
f
i
n
i
t
i
o
n
:
A
s
y
n
d
r
o
m
e
o
f
a
c
q
u
i
r
e
d
i
m
p
a
i
r
m
e
n
t
o
f
m
e
m
o
r
y
a
n
d
o
t
h
e
r
c
o
g
n
i
t
i
v
e
d
o
m
a
i
n
s
s
u
f
f
i
c
i
e
n
t
t
o
a
f
f
e
c
t
d
a
i
l
y
l
i
f
e
•
E
t
i
o
l
o
g
y
:
A
n
y
d
i
s
o
r
d
e
r
c
a
u
s
i
n
g
d
a
m
a
g
e
t
o
b
r
a
i
n
s
y
s
t
e
m
s
i
n
v
o
l
v
e
d
i
n
m
e
m
o
r
y
.
A
l
z
h
e
i
m
e
r
’
s
d
i
s
e
a
s
e
i
s
t
h
e
m
o
s
t
c
o
m
m
o
n
c
a
u
s
e
i
n
l
a
t
e
r
l
i
f
e
An umbrella term there are many causes
.
AD
AD
Vascular
Vascular
Lewy BD
Lewy BD
Other
Other
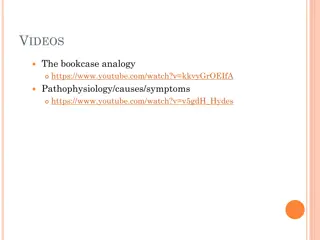
Dementia
:
Evaluation
•
History
/physical
•
Neurologic
•
Medications
•
Mood
•
Abilities
•
Social
Diagnostic Pathway
Alzheimer’s Ds.
History
Physical Exam
Neurological Exam
Not AD
Not AD
Not AD
HISTORY OF SYMPTOMS
•
From a
caregiver or
someone close
to the patient
The Dementia Evaluation
History
•
Collateral Source
•
Onset, Course, Progression, Risk Factors
•
Characteristic Course of Alzheimer’s
Disease
HISTORY OF SYMPTOMS
•
What were the
first symptoms?
•
How have things
changed?
•
Is this typical
for AD?
We use a semi-structured interview done by
social work and they also describe the social
network, caregivers and who needs help
TYPICAL SYMPTOMS OF
ALZHEIMER’S DISEASE
Functional loss in reverse order to
which skills were gained
Dementia Diagnostic Pathway
Alzheimer’s Ds.
History
Physical Exam
Neurological Exam
Not AD
Not AD
Not AD
Geriatric Exam: not only the
patient!!
Examine the environment
Sutton’s Law
:
•
“Gee, Willy, why do you rob banks?
“BECAUSE
THAT’S
WHERE THE
MONEY IS”
G
e
r
i
a
t
r
i
c
i
a
n
’
s
L
a
w
:
Go for the MEDS
Because that’s where the money is
Inspect the Drug Bag
•
Three or more drugs increase
the likelihood of an adverse
effect or drug interaction
Drugs and Dementia
•
Many drugs make patients worse,
e.g.
Sedatives, anxiolytics, anticholinergics,
H2-blockers, centrally acting
antihypertensives (
clonidine, alpha-methyl
dopa
) antiarhythmics, beta blockers, digoxin,
sinemet, selegeline.
•
Don’t forget herbals and OTCs
•
Check all for
CNS
S.E.s
•
Try a “
Drug Holiday
”
Alcohol and Dementia
n
Volume of
Volume of
distribution for
distribution for
ETOH
ETOH
with age
with age
n
No more than one/day
No more than one/day
after age 65; stop all if
after age 65; stop all if
cognition impaired
cognition impaired
The Dementia Evaluation
Laboratory
•
B-12, Folate, TSH
•
Chem profile, UA, ?O
2
sat
•
CBC
•
Other as indicated –most often drug levels
The Dementia Evaluation
Radiology & Other
•
Head CT, ? Head MRI
•
Chest X-ray
•
EKG, EEG
T
h
i
n
g
s
t
h
a
t
C
a
u
s
e
t
h
e
B
r
a
i
n
t
o
F
a
i
l
(
w
h
e
t
h
e
r
o
r
n
o
t
a
n
u
n
d
e
r
l
y
i
n
g
d
e
m
e
n
t
i
a
i
s
p
r
e
s
e
n
t
)
•
Drugs
•
Emotional Illness (including depression)
•
Metabolic/endocrine disorders
•
Eye/ear/environment
•
Nutritional/neurological
•
Tumors/trauma
•
Infection
•
Alcoholism/anemia/ atherosclerosis
D
E
M
E
N
T
I
A
Caregiver Support: core services offered by
the Alzheimer’s Association
•
Information and Referral
•
Care Consultation
•
Safety Services
•
Early-Stage Engagement Programs
•
Support Groups
•
Monthly Educational Programs
•
Brain Health Awareness
•
Clinical Trials
N
-
6
4
8
M
e
d
i
c
a
l
C
e
r
t
i
f
i
c
a
t
i
o
n
f
o
r
D
i
s
a
b
i
l
i
t
y
E
x
c
e
p
t
i
o
n
t
o
t
h
e
E
n
g
l
i
s
h
&
c
i
v
i
c
s
t
e
s
t
r
e
q
u
i
r
e
m
e
n
t
s
f
o
r
n
a
t
u
r
a
l
i
z
a
t
i
o
n
b
e
c
a
u
s
e
o
f
p
h
y
s
i
c
a
l
d
i
s
a
b
i
l
i
t
y
o
r
m
e
n
t
a
l
i
m
p
a
i
r
m
e
n
t
•
History of cognitive disability: use AD-8 to document a decline in
function during adult life
•
Cognitive measure: Short Blessed or low-literacy MOCA
•
ICD 10 for presumed diagnosis
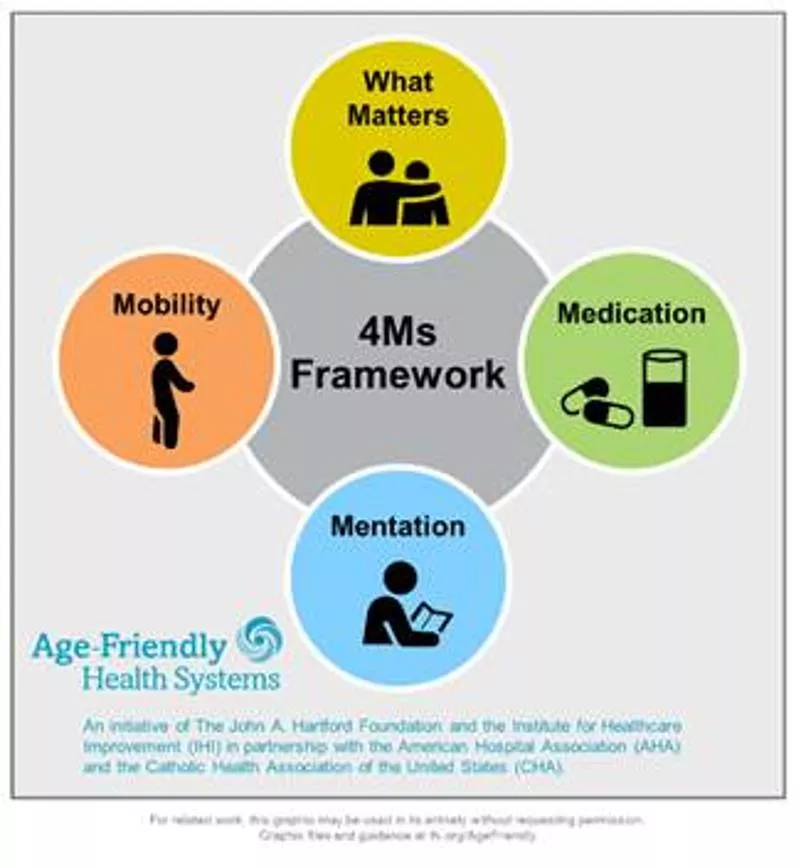
This program delves into the essential elements of diagnosing and managing dementia, emphasizing the interprofessional teamwork required for effective evaluation. Explore the varied factors contributing to dementia and discover ways to improve patient outcomes.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Age Friendly Primary Care: a Partnership between OneWorld and UNMC s Geriatrics Workforce Enhancement Program
This program is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of an award totaling 749,926.00 with 0% financed with non- governmental sources. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the U.S. Government. For more information, please visit HRSA.gov.
Objectives: Objectives: Understand essential elements of history in the diagnosis and differential diagnosis of dementia. Describe how members of the interprofessional team work together in evaluation and management of dementia. Recognize dementia as a geriatric syndrome with different factors contributing SOME of which can either be improved or where we can go to help patients compensate.
DEMENTIA: History Physical and Social Networks
EtiologyPathogenesisPresenting Disease KNOWN KNOWN Symptoms KNOWN, but variable presentation Factor 1 Interacting Geriatric Syndrome Factor 2 Interacting Single Manifestation Factor3 Interacting Factor4 Interacting
DEMENTIA The most common cause of disability in later life A focus for providers of health care to older adults
Dementia Definition: A syndrome of acquired impairment of memory and other cognitive domains sufficient to affect daily life Etiology: Any disorder causing damage to brain systems involved in memory. Alzheimer s disease is the most common cause in later life
DEMENTIA AD Lewy BDOther Vascular An umbrella term there are many causes.
Dementia: Evaluation History/physical Neurologic Medications Mood Abilities Social
Diagnostic Pathway History Not AD Not AD Physical Exam Neurological Exam Not AD Alzheimer s Ds.
HISTORY OF SYMPTOMS From a caregiver or someone close to the patient
The Dementia Evaluation History Collateral Source Onset, Course, Progression, Risk Factors Characteristic Course of Alzheimer s Disease
HISTORY OF SYMPTOMS What were the first symptoms? How have things changed? Is this typical for AD? We use a semi-structured interview done by social work and they also describe the social network, caregivers and who needs help
TYPICAL SYMPTOMS OF ALZHEIMER S DISEASE Functional loss in reverse order to which skills were gained
Dementia Diagnostic Pathway History Not AD Not AD Physical Exam Neurological Exam Not AD Alzheimer s Ds.
Geriatric Exam: not only the patient!! Examine the environment
Suttons Law: Gee, Willy, why do you rob banks? BECAUSE THAT S WHERE THE MONEY IS
Geriatricians Law: Geriatrician s Law: Go for the MEDS Because that s where the money is
Inspect the Drug Bag Three or more drugs increase the likelihood of an adverse effect or drug interaction
Drugs and Dementia Many drugs make patients worse, e.g. Sedatives, anxiolytics, anticholinergics, H2-blockers, centrally acting antihypertensives (clonidine, alpha-methyl dopa) antiarhythmics, beta blockers, digoxin, sinemet, selegeline. Don t forget herbals and OTCs Check all for CNS S.E.s Try a Drug Holiday
Alcohol and Dementia Volume of distribution for ETOH with age No more than one/day after age 65; stop all if cognition impaired
The Dementia Evaluation Laboratory B-12, Folate, TSH Chem profile, UA, ?O2 sat CBC Other as indicated most often drug levels
The Dementia Evaluation Radiology & Other Head CT, ? Head MRI Chest X-ray EKG, EEG
Things that Cause the Brain to Fail Things that Cause the Brain to Fail (whether or not an underlying dementia is present) (whether or not an underlying dementia is present) D E M E N T I A Drugs Emotional Illness (including depression) Metabolic/endocrine disorders Eye/ear/environment Nutritional/neurological Tumors/trauma Infection Alcoholism/anemia/ atherosclerosis
Caregiver Support: core services offered by the Alzheimer s Association Information and Referral Care Consultation Safety Services Early-Stage Engagement Programs Support Groups Monthly Educational Programs Brain Health Awareness Clinical Trials
N N- -648 648 Medical Certification for Disability Exception to the English & civics test requirements for naturalization because of physical disability or mental impairment History of cognitive disability: use AD-8 to document a decline in function during adult life Cognitive measure: Short Blessed or low-literacy MOCA ICD 10 for presumed diagnosis