Understanding Varicose Veins: Causes, Symptoms, and Treatment Options

Varicose veins are dilated and tortuous veins affecting a significant percentage of the adult population. Dr. Mohammed J. Jameel provides valuable insights into the causes, clinical features, diagnostic methods such as duplex ultrasound imaging, and treatment options including injection sclerotherapy and surgical interventions for varicose veins. Understanding the predisposing factors, inheritance patterns, and management strategies can help individuals suffering from varicose veins make informed decisions about their health.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Vascular Surgery Dr.Mohammed J. Jameel FIBMS.Th.CVS.Senior Lecturer. Department of Surgery, College of Medicine, Al-Mustansiriyah University, Baghdad, Iarq.
Lec Lec : : 3 3 Venous System: Varicose Veins: - defined as tortuous dilated veins which affect 5% of adult population. M > F but most Pt.s seek for Rx. Are F. there is +ve family history for inheritance through FOXC2 gene. V.V develops due to defect in connective tissue and smooth muscles in vein wall leading to secondary incompetence in the valves , other predisposing factors are: - 1.DVT 2.Pregnancy 3.Pelvic tumors 4.Age 5.Weight and Hight- heavy weight and tall pts. are more liable. 6.Diet: Low fiber diet leads to chronic constipation which V.Vs 7.side - left > right 8.Occupation with long standing period.
Clinical Features :- 1. Ache in the vein after prolonged standing. 2. Ankle swelling , itching , bleeding , superficial thrombophlibitis, ulceration. 3.Tortous dilated veins in the subcutaneous tissue 4. varicosities in the thigh are indicative of long SV incompetence while varicosities on the back of the leg are suggestive of short SV incompetance 5. Cough thrill a vibration can be felt by gentle palpation through the fingers over sapheno-femoral junction while the pt. is coughing caused by turbulent backflow with in the varicosity. 6. Tourniquet test when tourniquet is applied round the upper thigh after elevation of the limb and emptying of the veins can control all lower limb varicosities indicating sapheno-femoral junction incompetence , release of tourniquet leads to rapid refill of varicosities confirm the Dx. Greater SV varicosity represent 80% of cases.Test for Lessor SV. By tourniquet placed below Knee to test Sapheno-popliteal junction incompetence.
Duplex u/s imaging the probe of Duplex scanner contains multiple emitting and receiving crystals , this allow the vein to be seen as a black void in subcutaneous and deep tissues. Directional flow can be seen as a coulor image super-imposed on grey scale image of the vessel , visible venous flow can be seen when augmented by calf squeeze , the duplex image allow the vein to be traced to its termination while compression and relaxation can demonstrate the presence of retrograde flow( reflux). Mx indication for intervention / 1.cosmotic appearance esp. for female. 2.Reccurent episode of bleeding. 3.development of skin changes. a.if varicose vein is secondary to DVT or elderly Pt. who doesnot not seek surgery Rx. done By use of below Knee Class 2 Elastic compression stockings with Ankle pressuer 30mm Hg decrease to 15 mm Hg at knee level.
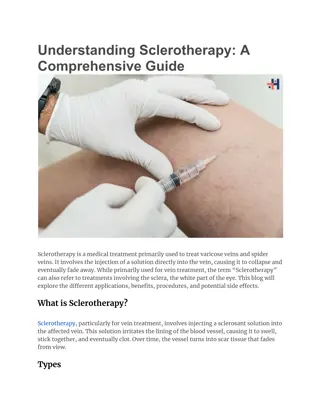
b. Injection seclerotherapy using Sodium Tetredecyl Sulphate is injected directly into the superficial veins to destroy the lipid memberane of endothelial cells which will shed leading to fibrosis and obliteration of vein with local compression on injected veins , it is useful for minor varicosities and recurrent cases in calf and lower leg. c. Surgery done by ligation of the communication point i.e sapheno-femoral or Saphenopopliteal junctions and remove the major part of incompetent trunk using Babcocks intraluminal stripper then small tributaries are removed individually by making minor cut downs and avulse them out from under the skin.
D.V.T :- is the formation of semisolid coagulum with in the flowing blood in the venous system , it carries high risk of Pulmonary Embolism and Sudden death. Etiology - 1. Change in vessel wall ( endothelial damge). 2. Stasis leads to decrease blood flow through the vein. 3. increase blood viscosity Risk factors for DVT- 1. Pt. factors a. age b.obesity c.varicosity d.immobility g.high dose Estrogene Rx h.previous DVT. 2. Disease or surgery- a.Trauma or surgery esp. pelvic , hip. b. Malignancy eps. Pelvic or abdominal. C. Heart failure d. Recent MI e. Lower limb paralysis f. infection e.pregnancy f.puerperium
Pathology :- the thrombus usually develop in the soleal veins of calf initially as platelet aggregate then fibrin and red cells form a mesh until the lumen of the vein occludes , the thrombus extend up to next large vein branch and may break off and pass through the large veins of lower limb and IVC and through the right side of the heart and embolise to the pulmonary arteries of the lung as P.E. , this may totally occlude perfusion to all or part of one or both lungs leading to acute right side heart failure with sudden collapse and death.
Dx : 1. Pain and Swelling in the calf of one lower limb . 2. pt. may present from start with ss of P.E e.g Dyspnea , haemoptysis , pleuretic chest pain. O/E 1. Mild pitting edema of ankle 2. Dilated superficial veins. 3. stiff calf 4.Low grade fever. 5. Tenderness over the course of deep veins. P.E- 1.cyanosis 2. Dyspnea 3.fixed splitting of 2ndheart sound 4.pleural rub. DVT Dx confirmed by Duplex U/S imaging which shows filling defects in the flow and lack of compressibility. P.E Dx confirmed by CT scan of Chest which shows filling defect in the pulmonary arteries. DDx of DVT is :-1.ruptuerd backers cyst 2.calf muscle hematoma 3. thrombosed popliteal aneurysm 4.arterial ischemia.
Prophylaxis:- pt. who are being admitted for surgery are classified to Low , moderate and high risk group. 1.Low risk pt.- are young with minor illness who will undergo opt. which last 30 min or less. 2. Moderate risk pt. - age >40 yr. or have debilitating illness and will undergo major surgery. 3. High risk pt. age >40 yr , have serious medical illness e.g CVA or MI , undergo major surgery with previous Hx of thromboembolism or malignant disease. Prophylactic methods which can be used are as following 1.good post-opt I.V hydration is simple method as the pt. will stay fasting for about 8 hours pre-opt together with internal body response which increase blood coagulability post-opt. and the inability of pt. to drink oral fluid in immediate post-opt. period all this will increase blood viscosity and make the pt highly susceptible to develop thromboembolism , therefore ; good I.V fluid Mx is very important and it breaks the vicious circle of stasis and increase blood viscosity
2.encourage the pt. to move his or her feet in the bed aginst some resistance this will make the calf muscles to contract and squeeze the blood from the venous sinusoids preventing clot formation 3. for pt.s who cannot move post-opt. e.g limb fracture we can use graduated elastic compression stockings and external pneumatic compression devices 4.Low-molecular weight heparin can be given subcutaneously 50 mg/Kg body Wt. as single or in 2 divided doses Rx start with Heparin I.V infusion 1000U/hr. together with oral Warfarine for 1stthree days then heparin stopped and Pt. kept on warfarine whose dose adjusted according to PT , INR ratio which must be between 2-3 , the pt must be kept in bed with minimum movement for 1 Wk to prevent clot detachment since the clot inside the vein is loosely adherent to vein wall in the 1stwk and easily can detach and cause pulmonary Embolism. P.E requires 1. Thrombolytic Rx 2.Cardiac support 3.I.V fluid 4. Pulmonary EmbolectomyThrough Median Sternotomy and Cardiopulmonary bypass.