Understanding Tuberculosis of the Skin: Clinical Aspects, Diagnosis, and Treatment
This comprehensive guide explores the different types of tuberculosis affecting the skin, including localized and generalized forms, as well as tuberculide. It covers clinical features, diagnostic methods like the tuberculin test, and treatment recommendations for conditions such as lupus vulgaris. The article also addresses important aspects of leprosy, its clinical spectrum, necessary investigations, and adverse reactions to anti-leprotic agents.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
CHRONIC BACTERIAL SKIN INFECTIONS
1- the student need know the various clinical aspects of TB of the skin & complications & how to treat 2-to know about the spectrum of leprosy ,the clinical features of each pole of the spectrum & necessary investigations required for the diagnosis 3- to learn more about the recommendations for treatment of leprosy & the expected adverse reaction of the anti-leprotic agents
types 1- localized: a- lupus vulgaris b- primary inoculation TB( TB chancre) c- tuberculosis verrucosa cutis ( warty TB) d- scrofuloderma e- oroficialTB
2- generalized: a- miliaryTB b-TB abscess c- lichen scrofulosorum 3- tuberculide: a- erythema induratum b- papulonecrotic tuberculide
Tuberculine test Intradermal injection of 0.1 ml of PPD ( purified protein derivative) & read after 48 hours looking for erythema & induration: -more than 10 mm: strong +ve 5-10 mm: moderately +ve less than 5 mm : weak +ve no reaction : -ve
Lupus vulgaris It is commonest type, affect mainly children & elderly, mainly seen on the face . The infection arises from distant focus, either by hematogenous or lymphatic spread in patient with high immunity against TB bacilli
Clinical features Asymptomatic red-brown nodules which coalesce to form well-demarcated plaque. Diascopy examination: apple jelly nodules. It is slowly progressive lesions takes sometimes years to develop & if not treated it will ulcerate & lead to scarring &deformities like ectropian of eyelids & destruction of the nose & rarely sq. cell carcinoma
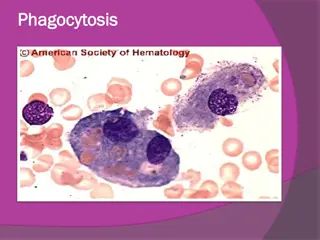
Diagnosis Histopathology: epitheloid cell granuloma: epitheloid cell & Langhan s giant cells surrounded by lymphocytes without necrosis. Zeil- Nelson stain for AFB is usually negative
treatment Antituberculous drugs course for 9 months: First 2 months: ethambutol + INH + rifampicin Next 7 months: INH+ rifampicin
Tuberculous chancre Caused by direct inoculation of TB bacilli into the skin from infected materials in patient with no immunity against TB (Tuberculine test is negative). It started as painless papule then enlarged to nodule which turn into painless ulceration with regional LN enlargement. Eventually heal spontaneously with scarring.
Warty TB result from direct inoculation of TB bacilli into the skin in patient with high immunity against TB bacilli. The source of infection is infected materials. physicians, pathologist & anatomist are at risk who handle infected cadavers ( called anatomist wart) Clinically appear as hyperkeratotic crusted warty plaque mainly on hands & feet
scrofuloderma Result from direct extension of TB bacilli from underlying tuberculous focus such as LN, bone or joint. The skin overlying TB focus is swollen with fluctuation & pus discharging lead to painless ulceration & heal with ugly scar
tuberculide Skin diseases related to TB as a result of hypersensitivity reaction to TB bacilli. The primary TB infection is not in the skin but elsewhere & skin biopsy show no bacilli. There are 2 types:
1-Erythema induratum( Bazin disease) Deep seated nodules on posterior aspect of the lower legs with ulceration. They are seen exclusively in middle age women.
2- papulonecrotic tuberculid Multiple necrotic papules & nodules seen mainly in lower limbs. both respond to anti-TB drugs
Leprosy ( Hansen`s disease) Chronic infection caused by Mycobacterium leprae: AFB, can not grow on artificial media but can be cultivated in animals like Armadillo & foot pad of mice. The micro-organism require low temperature. Transmission: infected air born droplet. The bacilli pass through nasal mucosa to reach blood stream & then to target organs ( peripheral nerves & skin)
Fade of infection Indeterminate leprosy: hypopigmented macule or patch, ill-defined border, on cold exposed area. The lesion is dry, anhidrotic ( no sweating), anesthetic or hyposthetic. It may disappear without any squale or lead to one of the determinate type of leprosy depending on the state of immunity
Spectrum of leprosy 1- lepromatous(L L) : patient with low immunity & large no. of bacilli . multibacillary 2-Tuberculoid (TL) : high immunity & few or no bacilli paucibacillary 3- Borderline(B B): in between 2 poles, include (BL & BT ), immunologically unstable
Lepramine test Intra-dermal injection of 0.1 ml of dead M.lepra & read after 48 hrs & after 4 wks( biopsy). It is not diagnostic test but used to assess the state of immunity against M.lepre: +ve in normal person & TL -ve in LL & BL weak +ve in BT
Tuberculoid leprosy Because of high immunity , there is mainly skin & nerve involvement. Skin lesions: they are one or few, on exposed cold areas, macules or patches, hypopigmented, loss of sensation, anhidrotic, loss of hair with slightly raised border, nerve adjacent to the lesions is thickened. Large peripheral nerve could be involved like median n.Ulner n. & area innervated by that nerve shows features of neuropathy( sensory or motor )
Lepromatous leprosy Because of no immunity, there is dissemination of the infection. Skin lesionsare multiple, bilateral, symmetrical, macules, papules & nodules. In the face, the lines of skin become deeper as the skin thickened ( leonine facies)
Nerve involvement : is usually late leading to peripheral neuropathy with loss of sensation in gloves & stocks, ulceration of digits. Other features:lymphadenopathy, hepatosplenomegaly, keratitis , orchitis
diagnosis 1-clinical feature 2-skin biopsy: TL: multiple tuberculoidgranuloma no bacilli , ZN stain negative LL: diffuse granuloma consist of foamy macrophages with large no. of bacilli in their cytoplasm, ZN stain positive.
3- slit-skin smear : A small skin incision is made; the site is then scraped to obtain tissue fluid from which a smear is made and examined after Ziehl- Neelsen staining. Specimens are usually obtained from both earlobes and two other active lesions.
4- PCR: M. leprae DNA detected by this technique makes the diagnosis of early Paucibacillary leprosy and identifies M. leprae after therapy
Treatment 1-LL: Dapsone100mg / d + rifampicin 600 mg once/ month + clofazimine 50 mg/ d at least for 2 years. 2-TL: Dapsone 100 mg/d + rifampicin 600 mg once/ month for 1 year
Lepra reactions Type l : Cell mediated immunity, occur in TL & BT . the existing lesions become more inflamed painful & tender associated with loss of nerve function. Treat: aspirin & prednisolone 30-60 mg/d
Type ll(erythema nodosum leprosum) Immune complex HSR, seen in LL, development of new lesions, multiple painful nodules with or without ulceration, widespread, associated with fever, lymphadenopathy, arthropathy Treatment: aspirin , predisolone thalidomide 100-400mg/ d
















")