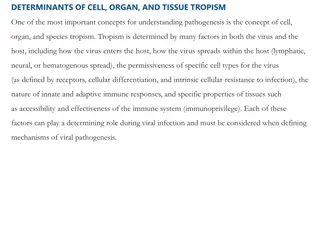
Understanding Peptic Ulcer Disease and Dyspepsia: Causes and Pathogenesis
Peptic ulcer disease and dyspepsia are common gastrointestinal conditions. Dyspepsia presents with upper abdominal pain and may or may not be associated with peptic ulcers. The most prevalent causes of dyspepsia include non-ulcer dyspepsia, GERD, and peptic ulcers. Peptic ulcers account for a significant portion of dyspepsia cases, characterized by discontinuities in the gastric or duodenal mucosa due to gastric juice acidity. Pathogenesis involves Helicobacter pylori infection in most cases, leading to inflammatory reactions and ulcer formation. NSAIDs can also contribute to ulcer formation through different mechanisms. Risk factors for NSAID ulcers include age, previous ulceration, high NSAID doses, and concomitant medication use. Understanding these conditions and their pathogenesis is crucial for effective management and prevention strategies.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Peptic Ulcer Disease Peptic Ulcer Disease
Dyspepsia Dyspepsia Persistent or recurrent pain or discomfort centered in the upper abdomen. Not all patients with dyspepsia have peptic ulcer. The most common causes of dyspepsia are -non-ulcer or functional dyspepsia, -GORD and -peptic ulcer
Peptic ulcer disease Peptic ulcer disease Peptic ulcer accounts for 10 15% of dyspepsia. The term peptic ulcer describes a discontinuity in the entire thickness of the gastric or duodenal mucosa that persists as a result of acid and pepsin in the gastric juice.
Pathogenesis Pathogenesis Those associated with Helicobacter pylori (95% PU, 80% DU) Helicobacter pylori (95% PU, 80% DU) Those associated with NSAIDs dyspepsia, 4% PU). NSAIDs and aspirin (20%
pathophysiology associated with infection involves: 1. 1. production of vacuolating pathophysiology associated with H. pylori infection involves: production of cytotoxin vacuolating cytotoxins which activate the inflammatory cascade H. pylori cytotoxin- -associated gene A ( cytotoxins which activate the inflammatory cascade associated gene A (CagA CagA) ) proteins and proteins and 2. 2. enzymes produced by UREASE enzymes produced by H. pylori UREASE, , haemolysins H. pylori may cause tissue damage include: haemolysins, neuraminidase and may cause tissue damage include: , neuraminidase and fucosidase fucosidase. . 3. 3. gastrin homeostasis hypergastrinaemia gastrin homeostasis is also altered resulting in hypergastrinaemia leads to an increased parietal cell mass is also altered resulting in Long leads to an increased parietal cell mass Long- -standing standing 4. 4. All these cause inflammation and ulcer formation. All these cause inflammation and ulcer formation.
Pathogenesis of NSAI drugs I. Superficial erosions and haemorrhages, II. Silent ulcers detected at endoscopy and III. Ulcers causing clinical symptoms and complications.
Box12.1 Box12.1- -Risk factors for NSAID ulcers Risk factors for NSAID ulcers Age greater than 65 years Previous peptic ulceration/bleeding High dose of NSAID or more than one NSAID (including aspirin). Short Concomitant corticosteroid or anticoagulant use Cardiovascular disease Age greater than 65 years Previous peptic ulceration/bleeding High dose of NSAID or more than one NSAID (including aspirin). Short- -term history of NSAID use Concomitant corticosteroid or anticoagulant use Cardiovascular disease term history of NSAID use
Clinical manifestations Clinical manifestations the symptoms of peptic ulcer disease overlap with duodenal ulcer, gastric ulcer or functional dyspepsia. 1. 1. Upper Upper abdominal abdominal pain pain related related to to food food----- ----- duodenal duodenal ulcer ulcer. . 2. 2. Upper Upper abdominal abdominal pain pain relieved relieved with with food food ------ ------gastric gastric ulcer ulcer. . 3. 3. Anorexia, Anorexia, weight weight loss, loss, nausea nausea and and vomiting, vomiting, heartburn heartburn. . 4. 4. Complications previous deficiency Complications of of peptic previous deficiency anaemia peptic ulcer symptoms pyloric stenosis ulcer disease symptoms---- stenosis and disease may ----haemorrhage and perforation may occur haemorrhage, , perforation. . occur with with or or without chronic without iron dyspeptic anaemia, , pyloric dyspeptic chronic iron- -
Patient assessment Patient assessment Reflux-like dyspepsia Heartburn plus dyspepsia Acid regurgitation plus dyspepsia Ulcer-like dyspepsia Localised epigastric pain Pain when hungry Pain relieved by food Pain relieved by antacids or acid- reducing drugs Pain that wakens the patient from sleep Pain with remission and relapses Dysmotility-like dyspepsia Upper abdominal discomfort (pain not dominant) Early satiety Postprandial fullness Nausea Retching or vomiting Bloating in the upper abdomen (no visible distension) Upper abdominal discomfort often aggravated by food Unspecified dyspepsia
Fig. 12.4 (A) Decision algorithm for Fig. 12.4 (A) Decision algorithm for management of uninvestigated dyspepsia. management of uninvestigated dyspepsia. Fig. 12.4, (B) Decision algorithm for Fig. 12.4, (B) Decision algorithm for management of non management of non- -ulcer dyspepsia. ulcer dyspepsia.
Investigations Investigations Endoscopy Endoscopy Radiology ( Radiology (Double-contrast barium) H. pylori H. pylori detection detection
Alarm features need endoscope Alarm features need endoscope Dysphagia Pain on swallowing Unintentional weight loss Gastro-intestinal bleeding or anaemia Persistent vomiting On NSAIDs or warfarin
Endoscopy Endoscopy
H. pylori H. pylori detection detection 1. 1. Serological tests to detect antibodies, 2. 2. [ [13 3. 3. Stool antigen tests. 4. 4. Invasive tests requiring gastric include urease tests, histology and culture. Serological tests to detect antibodies, C] urea breath tests. Stool antigen tests. Invasive tests requiring gastric antral include urease tests, histology and culture. 13C] urea breath tests. antral biopsies biopsies
Urea Breath Test
Uncomplicated peptic ulcer disease Uncomplicated peptic ulcer disease H. pylori eradication Triple therapy consists of: OCA: omeprazole 20 mg, clarithromycin 500 mg and amoxicillin 1 g or OCM: omeprazole 20 mg, clarithromycin 250 mg and metronidazole 400 mg. See fig 12.5 A, B
Patients with persistent symptoms after eradication may need: H. pylori This should be carried out no sooner than 4 weeks after. Patients with persistent symptoms after eradication may need: H. pylori status rechecked. status rechecked. If the patient is H. pylori If eradication causes of dyspepsia should be considered. H. pylori positive positive, an alternative eradication regimen. eradication was successful but symptoms persist, GERD or other
Complications of peptic ulcer disease Complications of peptic ulcer disease Bleeding peptic ulcer (endoscopic haemostatic therapy+ PPI) Pyloric stenosis
Prophylaxis of NSAID ulceration Prophylaxis of NSAID ulceration NSAIDs should be avoided of gastro-intestinal toxicity Box12.1 NSAID should be stopped patients with chronic rheumatological conditions and need NSAID avoided in patients who are at risk Box12.1 stopped if dyspepsia develops.
co-therapy with acid-suppressing agents or a synthetic prostaglandin analogue, or substitution of a selective COX-2 inhibitor for a non-selective NSAID
Ulcer- -healing drugs Proton pump inhibitors H2-receptor antagonists Bismuth chelate Sucralfate Antacids Ulcer healing drugs










 Decision algorithm for")