Overview of Stomach Surgery and Treatment Options

Surgery of the stomach and
duodenum.

The stomach
•
The stomach is a dilated part of the alimentary canal
between the esophagus and the small intestine.
•
It is a muscular sac.
•
It is a J-shaped
•
It occupies the left upper quadrant, epigastric, and
umbilical regions, and much of it lies under cover of
the ribs.
•
Stomach located at level of T10 and L3 vertebral.
•
Position of the stomach varies with body habitués.
The stomach
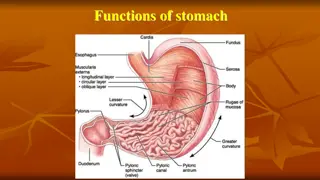
The stomach is divided into four
regions:
1.
The
cardia
, which surrounds the
opening of the esophagus into
the stomach.
2.
The
fundus of stomach
, which is
the area above the level of the
cardial orifice.
3.
The
body of stomach
, which is
the largest region of the
stomach.
4.
The
pyloric part
, which is
divided into the
pyloric antrum
and
pyloric canal
and is the
distal end of the stomach.
The stomach
Sphincters
T
e
cardiac sphincter (lower esophagus sphincter)
closes
off the top end of the stomach.
The
pyloric sphincter
closes off the bottom
Other features of the stomach include:
•
The
greater curvature
, which is a point of attachment
for the gastrosplenic ligament and the greater
omentum
•
The
lesser curvature
, which is a point of attachment
for the lesser omentum.
Surgical treatment
•
Stomach
Benign gastric Diseases
•
Stomach Malign gastric Diseases
Peptic ulcer disease
•
Indications for Surgery vs Conservative Management
•
Generally, 5% of bleeding ulcers require operative
management at some point. The following are
indications for urgent surgery:
•
Failure to achieve hemostasis endoscopically
•
Perforation
•
Recurrent bleeding despite endoscopic attempts at
achieving hemostasis
With respect the third indication, many clinicians
advocate surgery after two failed endoscopic attemps
Surgery therapy of PUD
•
Surgery is indicated for bleeding, perforation, gastric
outlet obstruction, intractability, and suspicion of
malignancy.
•
The ulcer must be excised.
•
The recurrence rate following surgical treatment for
gastric ulcer is extremely low.
•
Distal gastrectomy (approximately 50%) with excision
of the ulcer is the appropriate therapy (I, II, III).
•
Restoration of continuity is done by using one of these
3 options:
•
Bilroth I, Bilroth II and Roux en Y gastroenterostomy.
(learn the procedures).
Peptic ulcer perforation
•
Anamnesis, severe initial pain, tachycardia,
symptomatology:
1, severe initial pain(2-4h)
2, relative patient feel better(2-6h)
3, peritonitis sign
•
E: HCl,insufficiently mucosal protect, h.pylori
Peptic Ulcer (G+D, esophagus, GEA, Meckel diverticulum.)
Perforation - 0,5% people with peptic ulcer
10x more men than women.
Perforation is usually on front site of stomach, on rear wall
is tendency to penetrate and bleeding
•
S +DG: 80% of patients have positiv history of
ulcer, sudden pain in epigastrium,nausea,
vomiting, hematemesis, preventing to
movement, severe pain is reaction – chemical
irritation of peritoneum ( gastric acid,
pancreatic,bile…) , tachycardia,.defense,
percusion pain, leucocytosis…
X-ray ( pneumoperitoneum- may not be
detective in20-30%, particulary in duodenal
perforation)
Treatment: covered perforation- conservative
(parenteral nutrition,nasogastric intupation,
compres, antagonist H2 Rc., PPI, antacid) ,
Surgery intervention
Surgical Treatment
Surgical Treatment
Roux-en-Y Anastomosis
Total Gastrectomy
Duodenal ulcer
Pyloroplasty
Hiatus hernia
•
A
hiatus hernia
is a type of hernia in
which abdominal organs (typically the stomach
slip through the diaphragm into the middle
compartment of the chest.
•
This may result in g
a
stroesophageal reflux
disease
(GERD) or laryngop
H
aryngeal reflux (LPR) with
symptoms such as a taste of acid in the back of
the mouth or heartburn Other symptoms may
include trouble swallowing and ches
t
pains. Complications may include iron deficienc
y
anemia, volvulus, or bowel obstruction.
Roux-en-Y Gastric Bypass,
•
Selection of patients for bariatric procedures is based on
evidenced-based guidelines.
Patients must have failed dietary therapy and
have a body
mass index (BMI) greater than 40 kg/m2 without associated
medical conditions or a BMI greater than 35 kg/m2 with
associated medical
condition(s). In addition, practical
considerations for the patient to be a
candidate for the
procedure include psychiatric stability, a motivated
attitude,
and comprehension of the nature of the
procedure and the changes ineating that will follow the
procedure.
GASTROSTOMY – STAMM, WITZEL, AND
JANEWAY PROCEDURES
•
Gastrostomy
is the creation of an artificial
external opening into the stomach for nutritional
support
.
•
Gastrostomy is considered in the presence of
obstruction of the esophagus, but is most
frequently employed as a palliative procedure in
carcinoma of the esophagus or as the preliminary
step in the treatment of the cause of the
obstruction. The type of gastrostomy depends
upon whether the opening is to be temporary or
permanent.
Roux-en-Y Gastric Bypass
Gastric Sleeve Resection (Vertical Sleeve
Gastrectomy)
The stomach plays a crucial role in digestion and is divided into four regions - cardia, fundus, body, and pyloric part. Understanding the anatomy of the stomach is essential for surgical interventions, including treatment for benign and malignant gastric diseases like peptic ulcer disease. Surgical indications for peptic ulcer disease may include bleeding, perforation, and intractability. Surgical therapy for peptic ulcers involves excision of the ulcer, with distal gastrectomy being a common procedure. This overview provides valuable insight into stomach surgery and the management of various gastric conditions.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Surgery of the stomach and duodenum.
The stomach The stomach is a dilated part of the alimentary canal between the esophagus and the small intestine. It is a muscular sac. It is a J-shaped It occupies the left upper quadrant, epigastric, and umbilical regions, and much of it lies under cover of the ribs. Stomach located at level of T10 and L3 vertebral. Position of the stomach varies with body habitu s.
The stomach The stomach is divided into four regions: 1. The cardia, which surrounds the opening of the esophagus into the stomach. 2. The fundus of stomach, which is the area above the level of the cardial orifice. 3. The body of stomach, which is the largest region of the stomach. 4. The pyloric part, which is divided into the pyloric antrum and pyloric canal and is the distal end of the stomach.
The stomach Sphincters Te cardiac sphincter (lower esophagus sphincter) closes off the top end of the stomach. The pyloric sphincter closes off the bottom Other features of the stomach include: The greater curvature, which is a point of attachment for the gastrosplenic ligament and the greater omentum The lesser curvature, which is a point of attachment for the lesser omentum.
Surgical treatment Stomach Benign gastric Diseases Stomach Malign gastric Diseases
Peptic ulcer disease Indications for Surgery vs Conservative Management Generally, 5% of bleeding ulcers require operative management at some point. The following are indications for urgent surgery: Failure to achieve hemostasis endoscopically Perforation Recurrent bleeding despite endoscopic attempts at achieving hemostasis With respect the third indication, many clinicians advocate surgery after two failed endoscopic attemps
Surgery therapy of PUD Surgery is indicated for bleeding, perforation, gastric outlet obstruction, intractability, and suspicion of malignancy. The ulcer must be excised. The recurrence rate following surgical treatment for gastric ulcer is extremely low. Distal gastrectomy (approximately 50%) with excision of the ulcer is the appropriate therapy (I, II, III). Restoration of continuity is done by using one of these 3 options: Bilroth I, Bilroth II and Roux en Y gastroenterostomy. (learn the procedures).
Peptic ulcer perforation Anamnesis, severe initial pain, tachycardia, symptomatology: 1, severe initial pain(2-4h) 2, relative patient feel better(2-6h) 3, peritonitis sign E: HCl,insufficiently mucosal protect, h.pylori Peptic Ulcer (G+D, esophagus, GEA, Meckel diverticulum.) Perforation - 0,5% people with peptic ulcer 10x more men than women. Perforation is usually on front site of stomach, on rear wall is tendency to penetrate and bleeding
S +DG: 80% of patients have positiv history of ulcer, sudden pain in epigastrium,nausea, vomiting, hematemesis, preventing to movement, severe pain is reaction chemical irritation of peritoneum ( gastric acid, pancreatic,bile ) , tachycardia,.defense, percusion pain, leucocytosis X-ray ( pneumoperitoneum- may not be detective in20-30%, particulary in duodenal perforation) Treatment: covered perforation- conservative (parenteral nutrition,nasogastric intupation, compres, antagonist H2 Rc., PPI, antacid) , Surgery intervention
Hiatus hernia A hiatus hernia is a type of hernia in which abdominal organs (typically the stomach slip through the diaphragm into the middle compartment of the chest. This may result in gastroesophageal reflux disease (GERD) or laryngopHaryngeal reflux (LPR) with symptoms such as a taste of acid in the back of the mouth or heartburn Other symptoms may include trouble swallowing and chest pains. Complications may include iron deficiency anemia, volvulus, or bowel obstruction.
Roux-en-Y Gastric Bypass, Selection of patients for bariatric procedures is based on evidenced-based guidelines. Patients must have failed dietary therapy and have a body mass index (BMI) greater than 40 kg/m2 without associated medical conditions or a BMI greater than 35 kg/m2 with associated medical condition(s). In addition, practical considerations for the patient to be a candidate for the procedure include psychiatric stability, a motivated attitude, and comprehension of the nature of the procedure and the changes ineating that will follow the procedure.
GASTROSTOMY STAMM, WITZEL, AND JANEWAY PROCEDURES Gastrostomy is the creation of an artificial external opening into the stomach for nutritional support. Gastrostomy is considered in the presence of obstruction of the esophagus, but is most frequently employed as a palliative procedure in carcinoma of the esophagus or as the preliminary step in the treatment of the cause of the obstruction. The type of gastrostomy depends upon whether the opening is to be temporary or permanent.
Gastric Sleeve Resection (Vertical Sleeve Gastrectomy)