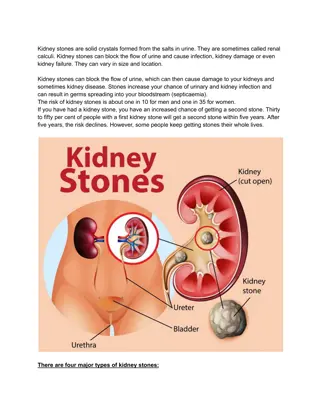
Understanding Nutrition for Stage 4 and Stage 5 Chronic Kidney Disease
June 2023
A Care Manager’s Guide to
A Care Manager’s Guide to
Understanding Nutrition and Stage 4
Understanding Nutrition and Stage 4
and Stage 5 Chronic Kidney Disease
and Stage 5 Chronic Kidney Disease
Karen
Greathou
se, RD,
CTCD
Renal Nutrition Specialist, University of Michigan
Kidney Transplant Program, Past National Chair
National Kidney Foundation Council of Renal
Nutrition
K
a
r
e
n
G
r
e
a
t
h
o
u
s
e
B
y
t
h
e
e
n
d
o
f
t
o
d
a
y
’
s
s
e
s
s
i
o
n
,
y
o
u
w
i
l
l
b
e
a
b
l
e
t
o
:
•
Explain the benefits of following an eating pattern that
helps manage kidney disease in combination with
diabetes, cardiovascular disease, and hypertension
•
Increase your confidence when it comes to supporting the
use of this eating pattern with patients
•
Provide updates to current recommendations for the
kidney diet and explain how the diet is tailored based on
individual labs
•
Understand how the kidney diet has evolved in the past 10
years
AB
is a
66
yo male
(height = 5’5”, weight = 200 lbs, BMI 33.16 kg/m
2
)
with a PMH
of hypertension, type 2 diabetes,
obesity, arthritis
, and GERD. He
presents to clinic today with the lab findings shown below. He is very
concerned about his
worsening kidney function, and he is now
experiencing symptoms of gout.
Medication List
Ibuprofen 600 mg as needed
Lisinopril 40 mg daily
Basaglar 20 units daily
Trulicity 3 mg weekly
Aspirin 81 mg daily
Rosuvastatin 10 mg daily
H
o
w
d
o
e
s
t
h
e
K
i
d
n
e
y
D
i
e
t
c
h
a
n
g
e
a
s
K
i
d
n
e
y
F
u
n
c
t
i
o
n
D
e
c
l
i
n
e
s
?
The kidney diet is individualized based on lab
values. There is no one kidney diet for
everyone. The Registered Dietitian will sit down
with each client and do an individual diet recall.
Elevations in potassium can be result of
constipation, elevated blood sugar, medications,
and diet.
R
e
n
a
l
N
u
t
r
i
t
i
o
n
M
y
t
h
N
u
m
b
e
r
1
:
W
h
o
l
e
g
r
a
i
n
s
a
n
d
d
r
i
e
d
b
e
a
n
s
h
a
v
e
t
o
o
m
u
c
h
p
h
o
s
p
h
o
r
o
u
s
While whole grains, nuts, seeds and beans do
contain phosphorus, only about 50% of this
phosphorus is absorbed, compared to 80-
100% of phosphorus in meat, fish, poultry,
dairy and phosphorus additives in processed
foods. KDOQI Guidelines recommend
considering phosphorus bioavailability.
This Photo
by Unknown author is licensed under
CC BY-SA
.
This Photo
by Unknown author is licensed under
CC BY-SA
.
R
e
n
a
l
M
y
t
h
N
u
m
b
e
r
2
:
P
e
o
p
l
e
w
i
t
h
C
K
D
n
e
e
d
a
l
o
w
p
o
t
a
s
s
i
u
m
d
i
e
t
•
The 2020 KDOQI guidelines
recommend that only
people who have high
serum potassium restrict
dietary potassium. A high
potassium diet can help
with blood pressure control.
R
e
n
a
l
N
u
t
r
i
t
i
o
n
M
y
t
h
N
u
m
b
e
r
3
:
F
r
u
i
t
s
a
n
d
v
e
g
e
t
a
b
l
e
s
s
h
o
u
l
d
b
e
l
i
m
i
t
e
d
•
Even for people who need to limit potassium, care should be
taken to include plenty of fruits and vegetables. Plant foods
can help improve acidosis by correcting acid base balance.
They can also decrease symptoms of gout. Dietary patterns
rich in fruits and vegetables are associated with a slower
progression and incidence of CKD.
R
e
n
a
l
N
u
t
r
i
t
o
n
M
y
t
h
N
u
m
b
e
r
4
:
T
h
e
r
e
i
s
a
s
i
n
g
l
e
r
e
n
a
l
d
i
e
t
f
o
r
e
v
e
r
y
o
n
e
•
CKD nutrition is different for
everyone! A healthy eating
pattern is based on each
person's labs, past medical
history, nutrition status and
current eating habits.
•
A Registered Dietitian is the
best person to help patients
understand what is right for
them to eat.
This Photo
by Unknown author is licensed under
CC BY
.
K
D
I
G
O
2
0
2
0
C
l
i
n
i
c
a
l
P
r
a
c
t
i
c
e
G
u
i
d
e
l
i
n
e
s
N
u
t
r
i
t
i
o
n
R
e
c
o
m
m
e
n
d
a
t
i
o
n
s
f
o
r
C
K
D
P
a
t
i
e
n
t
s
w
i
t
h
D
i
a
b
e
t
e
s
•
Nutrition Intake
•
Encourage a balanced, healthy diet that is high in vegetables, fruits, whole
grains fiber, legumes, plant-based proteins, unsaturated fats, and nuts
•
Limit processed meats, refined carbohydrates, and sweetened beverages
•
Limit sodium to less than 2000 mg daily
•
Recommend protein to .8 g/kg IBW
•
Glycemic Monitoring
•
Recommended monitoring (CGM may be useful)
•
Reliability of A1C decreases with declining kidney function
•
Glycemic Targets should be individualized ranging from less
than 6.5 to less than 8.0
W
h
a
t
a
b
o
u
t
P
r
o
t
e
i
n
?
•
Large amounts of protein may harm kidney function
by increasing waste products and causing the kidneys
to work harder during stage 3, 4, and 5 not on dialysis
•
Not getting enough protein can cause malnutrition
and muscle wasting, causing increased risk for illness
and infections
•
Eating protein frequently through day stabilizes blood
sugar and increases its absorption
•
Plant protein is easiest for kidney to filter; poultry
and fish are easier on the kidney than red meat
•
One or two vegetarian meals a week can benefit both
kidneys and diabetes and have a comparable amount
of potassium and phosphorous
•
Protein is needed to build muscle, heal from injury or
surgery, and fight infection
P
r
o
t
e
i
n
R
e
q
u
i
r
e
m
e
n
t
s
f
o
r
D
i
a
b
e
t
i
c
s
w
i
t
h
C
K
D
CKD stages 4 and 5 not yet on dialysis
•
42-65 grams or 6-9 ounces of high-quality
animal or plant protein
•
1 ounce protein = 7 grams protein
Dialysis patients have increased protein needs
•
Hemodialysis (HD) patients
need 70 to 90
grams or 10 to 13 ounces protein daily of
high-quality animal or plant protein
•
Peritoneal Dialysis(PD) patients
have higher
protein needs than HD and need 80 to 100
grams or 11 to 14 ounces daily of high-quality
animal or plant protein
W
h
a
t
a
b
o
u
t
P
o
t
a
s
s
i
u
m
?
•
Research demonstrates that plant-based foods have less
effect on potassium then animal and processed foods
•
Potassium has important role in nerve and muscle function,
including heart
•
As the GFR decreases, the kidneys do not adequately filter
out potassium, which could cause potassium to build up in
the blood and be dangerous
•
Elevated blood sugars can cause elevations in potassium
•
Cooking methods can increase or decrease potassium
levels
•
Should not stop eating vegetables and fruit to control
potassium levels
•
Not all patients need to restrict/limit potassium
•
Potassium typically limited to 2000 mg daily when
potassium lab values on upper end of acceptable
•
Dietary intake is not only cause of hyperkalemia
o
Constipation
o
Medications
o
Poorly managed diabetes
N
o
t
A
l
l
P
o
t
a
s
s
i
u
m
F
o
o
d
s
a
r
e
t
h
e
S
a
m
e
Potassium from these foods
Potassium from these foods
W
h
a
t
a
b
o
u
t
P
h
o
s
p
h
o
r
o
u
s
?
•
Phosphorus is a mineral that helps keep bones and blood vessels healthy
and muscles working properly
•
High phosphorous levels can cause itching, joint pain, and calcification
•
It is found naturally in foods rich in protein, whole grains, dairy, beans and
lentils
•
It is often added to foods and drinks as a preservative – called phosphorus
additives
•
100%of phosphorous in additives are absorbed, but only 67% of naturally
occurring phosphorous is absorbed
o
Whole grains are better option than white bread
•
Pills are often prescribed to act as a magnet to absorb phosphorous in the
gut and eliminate it in the poop
W
h
a
t
a
b
o
u
t
F
l
u
i
d
?
•
Managing salt intake and blood glucose will
decrease thirst and help prevent gaining excess
fluids
•
Anything that melts or pours counts as fluid, you
can not pour salad, vegetables and fruit, so they
do not count as fluid!
•
Fluid needs are different for people with CKD
•
Stages 3, 4, and early stage 5 usually require
64 oz. of fluid to keep kidney hydrated*
•
Dialysis patients typically need 40 ounces of
fluid plus what they urinate out
•
HD patients should not gain more than 5% of
their bodyweight between treatments
(including weekend)
•
PD patients often do not have to restrict fluid
* May differ if history of CHF
W
h
a
t
a
b
o
u
t
S
o
d
i
u
m
?
•
Helps keep fluids balanced in the body
•
When kidneys are not working well, extra sodium
and fluid build up in the body
o
swollen ankles
o
puffiness
o
rise in blood pressure
o
shortness of breath
o
sometimes fluid around your heart and lung
•
Sodium increases thirst and can cause excessive
•
Interdialytic weight gain in hemodialysis patients
•
Aim for less than 2400 mg sodium per day
o
500-700 mg per meal
o
400 mg for snacks
Diabetes and Kidney Disease
•
Diabetes often appears better managed when a person has kidney
disease
•
Insulin in body today will still be here tomorrow
•
Appetite often decreased with kidney disease
•
A1C is not as accurate marker of glucose control
•
Anemia is common and affects accuracy of A1C
•
Glucose Monitoring is better indicator of diabetes management
•
Managing blood sugars can maintain kidney function
•
Hypoglycemia is common, especially with Type 2 Diabetes
•
Hemoglobin A1C
combined with
home glucose monitoring
remains the
mainstay for assessing glycemic control in diabetics with renal disease
G
l
u
c
o
s
e
/
I
n
s
u
l
i
n
H
o
m
e
o
s
t
a
s
i
s
•
Decreased adiponectin concentrations are seen in CKD
and may contribute to the insulin resistance
•
Recent data suggest that alterations in body
metabolism with CKD may alter adipose tissue patterns
that are consistent with a more pro-inflammatory and
insulin-resistant state
•
Erythropoietin deficiency may contribute to insulin
resistance
•
Increased insulin resistance may contribute to
increased risk of cardiovascular disease in patients with
CKD
•
Low Vitamin D leads to decreased insulin production
and results in muscle breakdown
C
o
m
b
i
n
i
n
g
K
i
d
n
e
y
D
i
e
t
w
i
t
h
t
h
e
D
i
a
b
e
t
i
c
D
i
e
t
•
Focus on similarities, not differences
•
Provide guidelines for assistance
•
Stress need to eat 3 balanced meals at regular
times
•
Renal practice group has some good handouts with
diabetic renal material
•
NKF recently updated diabetic kidney material on
their website
B
a
l
a
n
c
e
m
a
t
t
e
r
s
Slow
and
steady.
Fat,
fiber
and
protein
slow
the
break down
of
food
in
the
stomach,
slowing
the
rise
in
blood
sugar.
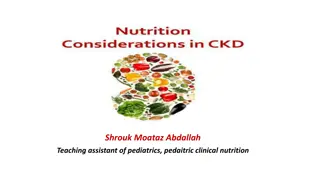
Mouth
Breakfast
Acai Berry Bowl
Calories 192
Carbs (g) 28
Potassium (mg) 349
Phosphorus (mg) 140
Sodium (mg) 82
Fiber (g) 7
Sample Meals
DaVita.com
Lunch
Peanut Butter Sandwich lunch box
Dinner
Easy Chicken and Pasta Dinner
Calories 456
Carbs (g) 50
Potassium (mg) 489
Phosphorus (mg) 322
Sodium (mg) 510
Fiber (g) 8
Calories 400
Carbs (g) 45
Potassium (mg) 455
Phosphorus (mg) 270
Sodium (mg) 328
Total | Calories 1,048 | Potassium 1,293 mg | Sodium 920 mg I Phosphorous 732 mg
Lifestyle Changes Can Improve Diabetes
Management
•
Eating 3 balanced meals at regular times
•
Meals should contain 45 to 60 grams of
carbohydrates
•
150 to 300 minutes of weekly physical activity
•
Eating 5 servings vegetables/fruit daily
Less potassium absorbed from plants than animal foods
Prevents constipation and helps maintain potassium in target
range
Aids weight loss
AB
has been a lawyer for many
years, and he finally made
partner last year. He was
referred to the dietitian and
started making the following
changes. He has been trying
not to skip lunch and is trying
to limit restaurant eating to 3
times a week. He is checking
his blood sugar 3 times a week
and wonders if he can stop
checking since A1C has
improved and diabetes
medications are being
reduced. He is eating 3 times
daily most days. He expressed
interest in increasing physical
activity. He is working hard to
increase intake of caffeine free
beverages.
N
u
t
r
i
t
i
o
n
Q
u
e
s
t
i
o
n
#
1
Your Patient AB asks about the increase in
potassium, which of the following should you not
do?
1.
Tell him to limit high potassium fruits/vegetables
2.
Ask if he is having regular bowel movements
3.
Ask what his sugars have been like when he is
testing at home
N
u
t
r
i
t
i
o
n
Q
u
e
s
t
i
o
n
#
2
AB’s A1C has improved from 8.0 to 6.5, which of the
following should you not do?
1.
Congratulate him on his improvement, and tell
him better blood sugar management can slow
progression ok kidney disease
2.
Tell him he no longer needs to check his blood
sugar
3.
Encourage him to continue to eat balanced
meals, balanced meal should contain complex
carbohydrate, lean protein(plant protein, poultry
or fish), and vegetables.
N
u
t
r
i
t
i
o
n
Q
u
e
s
t
i
o
n
#
3
Dialysis patients should never consume potatoes,
tomatoes, bananas, dried beans, whole-grains, and
nuts.
1.
True
2.
False
W
h
a
t
a
r
e
t
h
e
s
p
e
c
i
f
i
c
r
e
c
o
m
m
e
n
d
a
t
i
o
n
s
f
o
r
A
B
?
•
Reinforce no restriction on phosphorus
•
lab values in range
•
Moderate protein, more plant-based options
•
Daily recommendation of 60 – 70g per day
•
Absorb less potassium from plant based protein than animal protein
•
Encourage intake every 4/5 hours and congratulate him on not skipping meals
•
Encourage plate method to encourage balanced eating and increase intake of
vegetables/fruit to increase loss of phosphorous, potassium, and fluids in stool.
•
Encourage him to read labels for potassium additives, carbohydrates, and
sodium
•
Encourage limiting sodium to 2000 mg daily or 600 mg per meal
•
Encourage regular monitoring of blood sugar at home.
•
Encourage 64 ounces of water daily
•
Encourage 150 minutes physical activity weekly. May break into 10 minute
intervals
.
K
e
y
n
u
t
r
i
t
i
o
n
c
o
m
p
o
n
e
n
t
s
f
o
r
p
r
e
s
e
r
v
i
n
g
k
i
d
n
e
y
h
e
a
l
t
h
•
Eat an
adequate
amount of protein
•
Limit salt intake to help keep blood pressure under
control
•
Maintain potassium within recommended range
•
Maintain phosphorus within recommended range
•
Well managed blood sugars
•
Take in amount of fluid as directed by kidney team
When is it best to bring in an RD?
•
Complex nutritional needs
•
Example = CKD + Diabetes
•
Should consider nutrition referral
when GFR drops below 50.
•
Detailed nutrition questions
•
Patient interest/request
Does my patient quality to see an RD?
Medicare Guidelines for Medical Nutrition Therapy (MNT)
Referred by medical provider
Diagnosed with diabetes, renal disease or had kidney transplant within last 36
months
Delivered services by Registered Dietitian Nutritionist
Patient pays $0 – Part B deductible and coinsurance don’t apply
Frequency – 3 hours the first year, 2 hours subsequent years
Private Insurances often following Medicare guidelines, but vary
Patient may need to call insurance to check their coverage
H
o
w
d
o
I
f
i
n
d
a
n
R
D
q
u
a
l
i
f
i
e
d
t
o
h
e
l
p
?
Find a Nutrition Expert (eatright.org)
Check with your local hospital system
Call insurance company
Ask other doctors/healthcare professionals
R
e
s
o
u
r
c
e
s
•
Nutrition | National Kidney Foundation
•
DASH Eating Plan | NHLBI, NIH
•
The DASH Diet for Healthy Weight Loss, Lower Blood
Pressure and Cholesterol
•
Diet Review: DASH | The Nutrition Source | Harvard
T.H. Chan School of Public Health
•
Understanding the DASH diet: MedlinePlus Medical
Encyclopedia
•
Cooking Matters
•
PATH | Chronic Disease Self-Management | NKFM
•
Home | Diabetes Prevention Program
(readysetprevent.org)
MICMT Resources
https://micmt-cares.org/
35
MICMT Contact: https://micmt-cares.org/contact
D
i
s
c
l
a
i
m
e
r
Each physician organization and/or practice is solely
responsible for all medical care and services
delivered to its patients and all decisions related to
such medical care and services. Neither MICMT or
the Regents of the University of Michigan shall be
responsible for any delivery of medical care or other
services to any patient, or any decisions, acts or
omissions of persons in connection with the delivery
of medical care or other services to any patient.

A comprehensive guide for care managers to understand the importance of nutrition in managing kidney disease and its impact on patients with diabetes, cardiovascular disease, and hypertension. Covers current recommendations, individualized diets based on lab values, and the evolution of kidney diets over the past 10 years.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
A Care Managers Guide to Understanding Nutrition and Stage 4 and Stage 5 Chronic Kidney Disease June 2023
Karen Greathouse Karen Greathouse Karen Greathou se, RD, CTCD Renal Nutrition Specialist, University of Michigan Kidney Transplant Program, Past National Chair National Kidney Foundation Council of Renal Nutrition 2
By the end of todays session, you will be able to: By the end of today s session, you will be able to: Explain the benefits of following an eating pattern that helps manage kidney disease in combination with diabetes, cardiovascular disease, and hypertension Increase your confidence when it comes to supporting the use of this eating pattern with patients Provide updates to current recommendations for the kidney diet and explain how the diet is tailored based on individual labs Understand how the kidney diet has evolved in the past 10 years 3
AB is a 66 yo male (height = 55, weight = 200 lbs, BMI 33.16 kg/m2) with a PMH of hypertension, type 2 diabetes, obesity, arthritis, and GERD. He presents to clinic today with the lab findings shown below. He is very concerned about his worsening kidney function, and he is now experiencing symptoms of gout. Latest Reference Range & Units Sodium 136 - 146 mmol/L 137 Medication List Potassium 3.5 - 5.1 mmol/L 5.2 Ibuprofen 600 mg as needed Lisinopril 40 mg daily Basaglar 20 units daily Trulicity 3 mg weekly Aspirin 81 mg daily Rosuvastatin 10 mg daily Chloride 98 - 108 mmol/L 102 CO2 Urea Nitrogen Creatinine 20 - 31 mmol/L 8 - 20 mg/dL 0.70 - 1.30 mg/dL 19 58 (H) 4.0(H) Glucose Calcium 70 - 180 mg/dL 8.6 - 10.3 mg/dL 180 8.1 (L) Phosphorus 2.7 - 4.6 mg/dL .4.5 HbA1c Diabetes > or = 6.5% >=60 mL/min/1.73m2 8.0 eGFR, Creatinine-based formula (CKD-EPI 2021) 20(L) 4
How does the Kidney Diet change as How does the Kidney Diet change as Kidney Function Declines? Kidney Function Declines? The kidney diet is individualized based on lab values. There is no one kidney diet for everyone. The Registered Dietitian will sit down with each client and do an individual diet recall. Elevations in potassium can be result of constipation, elevated blood sugar, medications, and diet. 5
Renal Nutrition Myth Renal Nutrition Myth Number 1: Whole Number 1: Whole grains and dried grains and dried beans have too beans have too much phosphorous much phosphorous This Photo by Unknown author is licensed under CC BY-SA. While whole grains, nuts, seeds and beans do contain phosphorus, only about 50% of this phosphorus is absorbed, compared to 80- 100% of phosphorus in meat, fish, poultry, dairy and phosphorus additives in processed foods. KDOQI Guidelines recommend considering phosphorus bioavailability. 6 This Photo by Unknown author is licensed under CC BY-SA.
Renal Myth Number Renal Myth Number 2: People with CKD 2: People with CKD need a low need a low potassium diet potassium diet The 2020 KDOQI guidelines recommend that only people who have high serum potassium restrict dietary potassium. A high potassium diet can help with blood pressure control. 7
Renal Nutrition Renal Nutrition Myth Number 3: Myth Number 3: Fruits and Fruits and vegetables vegetables should be limited should be limited Even for people who need to limit potassium, care should be taken to include plenty of fruits and vegetables. Plant foods can help improve acidosis by correcting acid base balance. They can also decrease symptoms of gout. Dietary patterns rich in fruits and vegetables are associated with a slower progression and incidence of CKD. 8
Renal Nutriton Myth Renal Nutriton Myth Number 4: There is a Number 4: There is a single renal diet for single renal diet for everyone everyone CKD nutrition is different for everyone! A healthy eating pattern is based on each person's labs, past medical history, nutrition status and current eating habits. A Registered Dietitian is the best person to help patients understand what is right for them to eat. 9 This Photo by Unknown author is licensed under CC BY.
KDIGO 2020 Clinical Practice Guidelines KDIGO 2020 Clinical Practice Guidelines Nutrition Recommendations for CKD Nutrition Recommendations for CKD Patients with Diabetes Patients with Diabetes Nutrition Intake Encourage a balanced, healthy diet that is high in vegetables, fruits, whole grains fiber, legumes, plant-based proteins, unsaturated fats, and nuts Limit processed meats, refined carbohydrates, and sweetened beverages Limit sodium to less than 2000 mg daily Recommend protein to .8 g/kg IBW Glycemic Monitoring Recommended monitoring (CGM may be useful) Reliability of A1C decreases with declining kidney function Glycemic Targets should be individualized ranging from less than 6.5 to less than 8.0 10
What about Protein? What about Protein? Large amounts of protein may harm kidney function by increasing waste products and causing the kidneys to work harder during stage 3, 4, and 5 not on dialysis Not getting enough protein can cause malnutrition and muscle wasting, causing increased risk for illness and infections Eating protein frequently through day stabilizes blood sugar and increases its absorption Plant protein is easiest for kidney to filter; poultry and fish are easier on the kidney than red meat One or two vegetarian meals a week can benefit both kidneys and diabetes and have a comparable amount of potassium and phosphorous Protein is needed to build muscle, heal from injury or surgery, and fight infection 11
Protein Requirements for Protein Requirements for Diabetics with CKD Diabetics with CKD CKD stages 4 and 5 not yet on dialysis 42-65 grams or 6-9 ounces of high-quality animal or plant protein 1 ounce protein = 7 grams protein Dialysis patients have increased protein needs Hemodialysis (HD) patients need 70 to 90 grams or 10 to 13 ounces protein daily of high-quality animal or plant protein Peritoneal Dialysis(PD) patients have higher protein needs than HD and need 80 to 100 grams or 11 to 14 ounces daily of high-quality animal or plant protein 12
What about Potassium? What about Potassium? Research demonstrates that plant-based foods have less effect on potassium then animal and processed foods Potassium has important role in nerve and muscle function, including heart As the GFR decreases, the kidneys do not adequately filter out potassium, which could cause potassium to build up in the blood and be dangerous Elevated blood sugars can cause elevations in potassium Cooking methods can increase or decrease potassium levels Should not stop eating vegetables and fruit to control potassium levels Not all patients need to restrict/limit potassium Potassium typically limited to 2000 mg daily when potassium lab values on upper end of acceptable Dietary intake is not only cause of hyperkalemia oConstipation oMedications oPoorly managed diabetes 13
Not All Potassium Foods are the Same Not All Potassium Foods are the Same Potassium from these foods Potassium from these foods 14
What about Phosphorous? What about Phosphorous? Phosphorus is a mineral that helps keep bones and blood vessels healthy and muscles working properly High phosphorous levels can cause itching, joint pain, and calcification It is found naturally in foods rich in protein, whole grains, dairy, beans and lentils It is often added to foods and drinks as a preservative called phosphorus additives 100%of phosphorous in additives are absorbed, but only 67% of naturally occurring phosphorous is absorbed o Whole grains are better option than white bread Pills are often prescribed to act as a magnet to absorb phosphorous in the gut and eliminate it in the poop 15
What about Fluid? What about Fluid? Managing salt intake and blood glucose will decrease thirst and help prevent gaining excess fluids Anything that melts or pours counts as fluid, you can not pour salad, vegetables and fruit, so they do not count as fluid! Fluid needs are different for people with CKD Stages 3, 4, and early stage 5 usually require 64 oz. of fluid to keep kidney hydrated* Dialysis patients typically need 40 ounces of fluid plus what they urinate out HD patients should not gain more than 5% of their bodyweight between treatments (including weekend) PD patients often do not have to restrict fluid * May differ if history of CHF 16
What about Sodium? What about Sodium? Helps keep fluids balanced in the body When kidneys are not working well, extra sodium and fluid build up in the body o swollen ankles o puffiness o rise in blood pressure o shortness of breath o sometimes fluid around your heart and lung Sodium increases thirst and can cause excessive Interdialytic weight gain in hemodialysis patients Aim for less than 2400 mg sodium per day o 500-700 mg per meal o 400 mg for snacks 17
Diabetes and Kidney Disease Diabetes often appears better managed when a person has kidney disease Insulin in body today will still be here tomorrow Appetite often decreased with kidney disease A1C is not as accurate marker of glucose control Anemia is common and affects accuracy of A1C Glucose Monitoring is better indicator of diabetes management Managing blood sugars can maintain kidney function Hypoglycemia is common, especially with Type 2 Diabetes Hemoglobin A1C combined with home glucose monitoring remains the mainstay for assessing glycemic control in diabetics with renal disease 18
Glucose/Insulin Homeostasis Glucose/Insulin Homeostasis Decreased adiponectin concentrations are seen in CKD and may contribute to the insulin resistance Recent data suggest that alterations in body metabolism with CKD may alter adipose tissue patterns that are consistent with a more pro-inflammatory and insulin-resistant state Erythropoietin deficiency may contribute to insulin resistance Increased insulin resistance may contribute to increased risk of cardiovascular disease in patients with CKD Low Vitamin D leads to decreased insulin production and results in muscle breakdown 19
Combining Kidney Diet with the Diabetic Diet Combining Kidney Diet with the Diabetic Diet Focus on similarities, not differences Provide guidelines for assistance Stress need to eat 3 balanced meals at regular times Renal practice group has some good handouts with diabetic renal material NKF recently updated diabetic kidney material on their website 20
Balance Balancematters matters Slow and steady. Fat, fiber and protein slow the break down of food in the stomach, slowing therise in blood sugar. Mouth 21
Sample Meals DaVita.com Lunch Breakfast Acai Berry Bowl Dinner Peanut Butter Sandwich lunch box Easy Chicken and Pasta Dinner Calories 456 Carbs (g) 50 Calories 192 Carbs (g) 28 Calories 400 Carbs (g) 45 Potassium (mg) 489 Phosphorus (mg) 322 Sodium (mg) 510 Fiber (g) 8 Potassium (mg) 349 Phosphorus (mg) 140 Sodium (mg) 82 Fiber (g) 7 Potassium (mg) 455 Phosphorus (mg) 270 Sodium (mg) 328 Total | Calories 1,048 | Potassium 1,293 mg | Sodium 920 mg I Phosphorous 732 mg 23
Lifestyle Changes Can Improve Diabetes Management Eating 3 balanced meals at regular times Meals should contain 45 to 60 grams of carbohydrates 150 to 300 minutes of weekly physical activity Eating 5 servings vegetables/fruit daily Less potassium absorbed from plants than animal foods Prevents constipation and helps maintain potassium in target range Aids weight loss 24
AB has been a lawyer for many years, and he finally made partner last year. He was referred to the dietitian and started making the following changes. He has been trying not to skip lunch and is trying to limit restaurant eating to 3 times a week. He is checking his blood sugar 3 times a week and wonders if he can stop checking since A1C has improved and diabetes medications are being reduced. He is eating 3 times daily most days. He expressed interest in increasing physical activity. He is working hard to increase intake of caffeine free beverages. 25
Nutrition Question # 1 Nutrition Question # 1 Your Patient AB asks about the increase in potassium, which of the following should you not do? 1. Tell him to limit high potassium fruits/vegetables 2. Ask if he is having regular bowel movements 3. Ask what his sugars have been like when he is testing at home 26
Nutrition Question # 2 Nutrition Question # 2 AB s A1C has improved from 8.0 to 6.5, which of the following should you not do? 1. Congratulate him on his improvement, and tell him better blood sugar management can slow progression ok kidney disease 2. Tell him he no longer needs to check his blood sugar 3. Encourage him to continue to eat balanced meals, balanced meal should contain complex carbohydrate, lean protein(plant protein, poultry or fish), and vegetables. 27
Nutrition Question # 3 Nutrition Question # 3 Dialysis patients should never consume potatoes, tomatoes, bananas, dried beans, whole-grains, and nuts. 1. True 2. False 28
What are the specific recommendations for AB? What are the specific recommendations for AB? Reinforce no restriction on phosphorus lab values in range Moderate protein, more plant-based options Daily recommendation of 60 70g per day Absorb less potassium from plant based protein than animal protein Encourage intake every 4/5 hours and congratulate him on not skipping meals Encourage plate method to encourage balanced eating and increase intake of vegetables/fruit to increase loss of phosphorous, potassium, and fluids in stool. Encourage him to read labels for potassium additives, carbohydrates, and sodium Encourage limiting sodium to 2000 mg daily or 600 mg per meal Encourage regular monitoring of blood sugar at home. Encourage 64 ounces of water daily Encourage 150 minutes physical activity weekly. May break into 10 minute intervals. 29
Key nutrition components for preserving Key nutrition components for preserving kidney health kidney health Eat an adequate amount of protein Limit salt intake to help keep blood pressure under control Maintain potassium within recommended range Maintain phosphorus within recommended range Well managed blood sugars Take in amount of fluid as directed by kidney team 30
When is it best to bring in an RD? Complex nutritional needs Example = CKD + Diabetes Should consider nutrition referral when GFR drops below 50. Detailed nutrition questions Patient interest/request 31
Does my patient quality to see an RD? Private Insurances often following Medicare guidelines, but vary Patient may need to call insurance to check their coverage 32
How do I find an RD qualified to help? How do I find an RD qualified to help? Find a Nutrition Expert (eatright.org) Check with your local hospital system Call insurance company Ask other doctors/healthcare professionals 33
Resources Resources Nutrition | National Kidney Foundation DASH Eating Plan | NHLBI, NIH The DASH Diet for Healthy Weight Loss, Lower Blood Pressure and Cholesterol Diet Review: DASH | The Nutrition Source | Harvard T.H. Chan School of Public Health Understanding the DASH diet: MedlinePlus Medical Encyclopedia Cooking Matters PATH | Chronic Disease Self-Management | NKFM Home | Diabetes Prevention Program (readysetprevent.org) 34
MICMT Resources https://micmt-cares.org/ MICMT Contact: https://micmt-cares.org/contact 35
Disclaimer Disclaimer Each physician organization and/or practice is solely responsible for all medical care and services delivered to its patients and all decisions related to such medical care and services. Neither MICMT or the Regents of the University of Michigan shall be responsible for any delivery of medical care or other services to any patient, or any decisions, acts or omissions of persons in connection with the delivery of medical care or other services to any patient. 36