Refugee Trauma and Mental Health: Understanding and Support
Explore the impact of trauma on ELL children's mental health, effective school interventions for refugees, definitions of refugee status, and the diverse origins of refugees. Learn how schools can foster resilience in war-exposed youth and support individuals as "persons of concern." Delve into specific refugee populations like those from Palestine, Afghanistan, and Somalia in various regions such as NE Ohio. Understand the UNHC definition of a refugee and the dynamics of displacement due to persecution.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Trauma and Mental Health in ELL Children Dr. Valerie Sartor
How can schools can foster resilience and well-being in refugees and other war-exposed youth?
Definitions Refugee Trauma Effective school interventions?
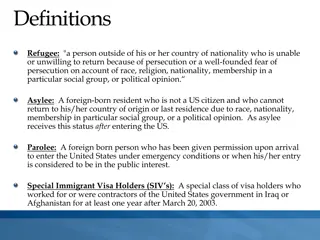
Refugees are a diverse assortment of individuals and groups who have fled their home countries due to actual or feared persecution.
UNHC Definition Owing to well-founded fear of being persecuted for reasons of race, religion, nationality, membership of a particular social group or political opinion, is outside the country of his nationality and is unable or, owing to such fear, is unwilling to avail himself of the protection of that country; or who, not having a nationality and being outside the country of his former habitual residence as a result of such events, is unable or, owing to such fear, is unwilling to return to it.
Person of Concern Persecution distinguishes refugees from other immigrant and migrant groups. The term person of concern describes an individual seeking asylum, lacking citizenship in any nation or state, or displaced within their native country by violence or conflict, as well as returning refugees.
2009 Palestine Afghanistan Iraq Columbia Sudan Somalia Burundi Congo Vietnam Turkey Eritrea
2013 Eastern Europe Asia China Mexico El Salvador Guatemala
NE Ohio 2016 Bhutan Somalia Iraq Burma percent Democratic Sudan Eritrea Burundi Ukraine Syria Other 1,070 refugees 489 refugees 404 refugees 296 refugees 35.8 percent 16.4 percent 13.5 percent 9.9 228 refugees 82 refugees 75 refugees 55 refugees 50 refugees 48 refugees 192 refugees 7.6 percent 2.7 percent 2.5 percent 1.8 percent 1.7 percent 1.6 percent 6.4 percent
Akron On February 9, 2017, CNN Money reported: Between 2007 and 2013, Akron's foreign born population increased by 30.8% from 7,208 to 9,426, helping to stem what could have been a devastating population decline.
47% of persons of interest 44% of refugees are younger than 18 years of age (UNHCR, 2010)
Psychological Distress Exposure to direct or indirect trauma, intergenerational trauma transferred between family members (A. Baker & Shalhoub- Kevorkian, 1999). Trauma may be cumulative - effects increase with repeated trauma (Bronstein & Montgomery, 2011). Trauma can be triggered - after resettlement (Kia- Keating & Ellis, 2007). Symptoms increase by the number/severity of traumas.
Preflight Trauma Witnessed or experienced violence Rape Been imprisoned or detained Lived in hiding Death or persecution of family members Child was persecuted Forced into war or sex slavery
Resettlement Trauma Dysfunctional family units influence a child s ability to adjust and learn at school, because negative/harmful coping behaviors within the family unit directly impact children. Children s emotional and mental states are connected to their family s emotions, attitudes, and beliefs and actions (McBrien, 2005).
Child Response to Trauma Fear, sadness, apathy, inattention, anger, irritability, separation anxiety, sleep disturbances, somatic complaints (e.g., headaches and stomachaches), and school problems (American Psychological Association, 2008)
Traumatized Refugee Youth Experience high rates of anxiety, depression, posttraumatic stress disorder (PTSD), and attention-deficit/hyperactivity disorder among refugee youth (Bronstein & Montgomery, 2011)
PTSD Symptoms Acute: re-experiencing the trauma, avoidance of trauma-related stimuli or emotional numbing, and hyper arousal (American Academy of Child and Adolescent Psychiatry [AACAP], 2010). General: sleep difficulties, irritability, anxiety, difficulty concentrating, oppositional behavior, separation anxiety, fears, apathy, and other impairments, including reduced academic achievement.
Incidence In Western countries the prevalence of PTSD among refugees was 11% among children, 10 times that of age-matched Americans (Fazel, Wheeler, & Danesh, 2005).
Confusion Clinicians question the validity of psychiatric diagnoses for culturally diverse populations. Some argue these children should not be considered ill as their behaviors reflect inevitable responses to extreme circumstances, Others argue that symptom manifestation is culturally bound (Rousseau, 1995).
Services A variety of counseling, individual or family therapy, psycho-education or skills training family or peer support Psychopharmacological interventions via clinical, counseling, or school psychologists Help via psychiatrists; therapists; social workers; nurses; and physicians to address children s psychiatric, social-emotional, or behavioral difficulties
Why Refugees Do Not Seek Services 1. Age very young Children and adolescents generally utilize mental health services at lower rates than adults do (Bean, Eurelings-Bontekoe, Mooijaart, & Spinhoven, 2006), treatment is often contingent on adult referral
2. High frequency of internalizing symptoms Symptoms are less noticeable or intrusive to others, thus reducing likelihood of referral.
3. Racial/ethnic minority status Minorities have significantly lower rates of mental health treatment than White peers (Bean, Eurelings-Bontekoe, et al., 2006) Linguistic and cultural barriers block access to appropriate services, (disparities in participation remain even when access is equalized (Alegria et al., 2010)).
Other Barriers to Services Difficulty navigating public services for children Difficulty understanding these systems of care Economic disadvantages Limited transportation Fear of disclosure or stigma (Hodes, 1998)
How Schools Can Help School participation links to resilience among refugee youth (Montgomery, 2010). Somali adolescent refugees who felt connected to school had lower depression and higher self- efficacy (Kia-Keating & Ellis, 2007). Wilkinson (2002) positive school performance reflects adjustment and acculturation and promotes students social-emotional function- ing/competence.
Schools Link to Community Schools are positioned to provide group services to refugee students - refugees tend to resettle in clusters; group treatment is practical and affordable (Ehntholt et al., 2005). School-based services have ease of access and help reduce stigma associated with treatment (Berger, Pat-Horenczyk, & Gelkopf, 2007).
Measures 1. SDQ: Strengths & Difficulties Questionnaire http://www.sdqinfo.com/py/sdqinfo/b3.py ?language=Englishqz(USA) Measures emotional symptoms, conduct problems, hyperactivity-inattention, peer problems, and personal strengths (Goodman, 2001) 2. Parent Interviews 3. Self-Report Measures 4. Use Multiple Measures/Culturally Sensitive
School Based Interventions 1. Creative Expression & Play Therapy Incorporates creative elements designed to offer children outlets to express their feelings and process emotions. Drawing/Drama/Music https://www.youtube.com/watch?v=xVflDJEyaZk
2. Trauma Focused-CBT Integrates attention to thoughts, behaviors, and feelings, focus on maladaptive behaviors and thoughts - generally problem focused and goal oriented requires practice beyond the sessions
Develops stress management skills via: psychoeducation parent training relaxation training, affective modulation cognitive processing developing narratives of the trauma mastering feared stimuli addressing safety concerns (AACAP, 2010).
Culturally Sensitive TF-CBT Foster coping skills in refugees by incorporating discussion of ethnic traditions and resettlement experiences. https://www.youtube.com/watch?v=axsButK QYCY
Structured and Culturally Sensitive CBT Multiple highly structured, culturally tailored CBT programs for refugee students have been tested.
Culturally Sensitive CCPT Child Centered Play Therapy Sessions use specific toys Therapists respect and feel empathy for students culture(s) Students feel safe communicating thoughts, feelings, and desires Use multicultural dolls, musical instruments, play food, and other toys reflective of children s cultural backgrounds (Schottelkorb et al., 2012)
4 Tier Trauma Systems Therapy Tier 1 activities - psycho-education, outreach, and engagement for the refugee community. Tier 2 activities - weekly skill- building groups for all refugee English language learner students during academic year. Tier 3 - trauma systems therapy for students referred by teachers. Tier 4 -intensive therapy and home-based care for severely impaired students.
Other Therapy EMDR http://www.emdr.com/what-is-emdr/ Hypnotherapy https://my.clevelandclinic.org/health/articles/clin ical-hypnotherapy Still Others; http://www.kidsmentalhealthinfo.com/topics/chi ld-trauma/effective-treatments-child-traumatic- stress/
Summary Variety of interventions exist School-based interventions appear effective Clinicians and educators face difficulties evaluating and creating interventions Intervention research is unclear refugees are vulnerable populations Interventions must be culturally appropriate
References American Academy of Child and Adolescent Psychiatry. (2010). Practice parameter for the assessment and treatment of children and adolescents with posttraumatic stress disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 49, 414 430. doi:10.1016/j.jaac.2009.12.020 Baker, A., & Shalhoub-Kevorkian, N. (1999). Effects of political and military traumas on children: The Palestinian case. Clinical Psychology Review, 19, 935 950. doi:10.1016/S0272-7358(99)00004-5 Alegria, M., Vallas, M., & Pumariega, A. J. (2010). Racial and ethnic disparities in pediatric mental health. Child and Adolescent Psychiatric Clinics of North America, 19, 759 774. doi:10.1016/j.chc.2010.07.001 American Academy of Child and Adolescent Psychiatry. (2010). Practice parameter for the assessment and treatment of children and adolescents with posttraumatic stress disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 49, 414 430. doi:10.1016/j.jaac.2009.12.020 American Psychological Association. (2008). Children and trauma: Update for mental health professionals. Retrieved from http://apa.org/pi/families/resources/ update.pdf Bean, T., Eurelings-Bontekoe, E., Mooijaart, A., & Spinhoven, P. (2006). Factors asso- ciated with mental health service need and utilization among unaccompanied refugee adolescents. Administration and Policy in Mental Health and Mental Health Services Research, 33, 342 355. doi:10.1007/s10488- 006-0046-2 Berger, R., Pat-Horenczyk, R., & Gelkopf, M. (2007). School-based intervention for prevention and treatment of elementary-students terror-related distress in Israel: A quasi-randomized controlled trial. Journal of Traumatic Stress, 20, 541 551. Bronstein, I., & Montgomery, P. (2011). Psychological distress in refugee children: A systematic review. Clinical Child and Family Psychology Review, 14, 44 56. doi:10.1007/s10567-010-0081-0 Ehntholt, K. A., Smith, P. A., & Yule, W. (2005). School-based cognitive-behavioral therapy group intervention for refugee children who have experienced war-related trauma. Clinical Child Psychology and Psychiatry, 10, 235 250. doi:10.1177/1359104505051214 Fazel, M., Wheeler, J., & Danesh, J. (2005). Prevalence of serious mental disorder in 7000 refugees resettled in Western countries: A systematic review. Lancet, 365, 1309 1314. doi:10.1016/S0140-6736(05)61027-6 Hodes, M. (1998). Refugee children: May need a lot of psychiatric help. British Medical Journal, 316, 793 794. doi:10.2307/25178549. Kia-Keating, M., & Ellis, B. H. (2007). Belonging and connection to school in resettle- ment: Young refugees, school belonging, and psychosocial adjustment. Clinical Child Psychology and Psychiatry, 12, 29 43. doi:10.1177/135910450707105 McBrien, J. L. (2005). Educational needs and barriers for refugee students in the United States: A review of the literature. Review of Educational Research, 75(3), 329 364. Montgomery, E. (2010). Trauma and resilience in young refugees: A 9-year follow-up study. Development and Psychopathology, 22, 477 489. doi:10.1017/ S0954579410000180 Rousseau, C. (1995). The mental health of refugee children. Transcultural Psychiatric Research Review, 32, 299 331. doi:10.1177/136346159503200304 Schottelkorb, A. A., Doumas, D. M., & Garcia, R. (2012). Treatment for childhood refugee trauma: A randomized, controlled trial. International Journal of Play Therapy, 21, 57 73. doi:10.1037/a0027430. Sullivan, A. L., & Simonson, G. R. (2016). A systematic review of school-based social-emotional interventions for refugee and war-traumatized youth. Review of Educational Research, 86(2), 503-530. United Nations High Commissioner for Refugees. (2010). Statistical yearbook 2010, 10th edition: Trends in displacement, protection and solutions. Geneva, Switzerland. United Nations High Commissioner for Refugees. (2012a). Global trends 2011: A year of crises. Retrieved from http://unhcr.org.au/unhcr/images/Global%20Trends%20 2011.pdf Wilkinson, L. (2002). Factors influencing the academic success of refugee youth in Canada. Journal of Youth Studies, 5, 173 193. doi:10.1080/13676260220134430