Overview of Trypanosomes: Characteristics, Life Cycle, and Diseases


HEMOFLAGELLATES-
TRYPANOSOMES
DR MONIKA RAJANI
ASSOCIATE PROFESSOR ,
DEPT OF MICROBIOLOGY
CIMSH ,LKO
DR MONIKA RAJANI

Classification

B-SUPERCLASS
MASTIGOPHORA
1-INTESTINAL FLAGELLATE -Giardia intestinalis
2-GENITAL FLAGELLATE- Trichomonas vaginalis
3-BLOOD AND TISSUE FLAGELLATES- Trypanosoma
Leishmania
DR MONIKA RAJANI
General characteristics
•
Live in
blood and tissues of man
and other vertebrate
hosts and in gut of insect vectors.
•
Life cycle in
two hosts
: vertebrate hosts(definitive host)
and insect vectors(intermediate host).
•
Trypomastigote and amastigote main stages
in life cycle
•
Epimastigote and promastigote forms
are also seen.
•
Multiplication occures by
binary fission
.
•
No sexual cycle is known
.
•
Two modes of development in vectors:
salivaria and
stercoraria.
DR MONIKA RAJANI
Morphological forms
•
Different stages Trypomastigote stage
DR MONIKA RAJANI
Development in vector
•
Salivaria
: trypanosomes migrate to
mouth parts
of
vectors such that infection is transmitted by their
bite
.
•
eg T gambiense ,T rhodesiense by
bite of tsetse fl
y
•
Stercoraria
: Trypanosomes migrate to
hind gut
and
are passed in feces.
•
eg: T cruzi-
Chagas
disease-acquired by rubbing
feces of vector bug into wound caused by its bite.
DR MONIKA RAJANI
Distribution
•
I: African Trypanosomiasis
:
sleeping sickness
•
Caused by
Trypanosoma brucei complex
(T brucei
gambiense, T brucei rhodesiense).
•
II: South American Trypanosomiasis
:
Chagas disease
.
•
Caused by
T cruzi
DR MONIKA RAJANI
Trypanosoma Brucei complex
•
Sleeping sickness
•
Habitat
: man and other vertebrate host.
:blood, lymph nodes,CNS,connective tissues.
DR MONIKA RAJANI
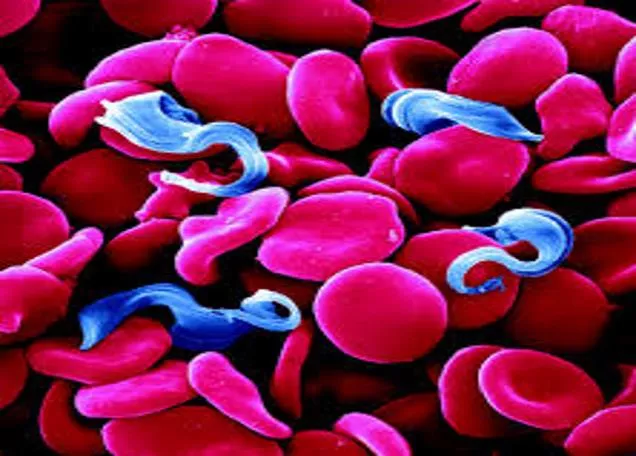
Morphology -
Vertebrate forms
Trypomastigote form
:
pleomorphic
:
long slender forms
, short stumpy
forms and intermediate forms.
:in blood films seen as
colourless
spindle shaped bodies
:move rapidly spinning around cells
:
Giemsa stain
: cytoplasm pale blue
and nucleus is red
:kinetoplast as red dot
:flagellum is red
DR MONIKA RAJANI
Morphology –
Insect forms
•
Epimastigote forms
•
Metacyclic Trypomastigote forms
DR MONIKA RAJANI
LIFE CYCLE
•
Two hosts:
•
Vertebrate host
: man,game animals and domestic
animals
•
Invertebrate host
: tse tse fly(male and female flies of
Glossina spp)
•
Infective form
:
metacyclic trypanomastigote forms
are infective to humans.
•
Mode of transmission
:
bite of tse tse fly
:Congenital transmission
•
Reservoir
:
man is the only reservoir host.
DR MONIKA RAJANI
Life Cycle
DR MONIKA RAJANI
Clinical features
•
West African sleeping sickness(chronic disease).
•
Painless chancre
at site of bite
•
Fever,chills,rash,anemia,headache
•
Winter Bottoms sign
-
H
epato spleenomegaly, lymphadenopathy
in posterior cervical region.
•
Myocarditis
•
Hematological
manifestations.
•
CNS manifestations
: headache
•
mental dullness,apathy
•
Day time sleepiness
.
•
Profound coma
•
Death
DR MONIKA RAJANI
Lab diagnosis
•
Routine tests:
•
Blood picture-anemia
•
WBC raised,DLC-monocytosis
•
ESR-raised
•
Reversal of albumin globulin ratio
•
CSF:raised pressure,cell counts and proteins
DR MONIKA RAJANI
Lab diagnosis
•
Specific tests:
•
Sample: peripheral blood
•
bone marrow
•
lymph node aspirate
•
CSF
•
chance fluid.
DR MONIKA RAJANI
Microscopy
•
Wet mount
preparation
:demonstration of
trypomastigote forms
.
•
Giemsa stain
of thick
peripheral smears.
•
Concentration
techniques
:buffy coat
:Membrane
filtration methods
DR MONIKA RAJANI
Culture
•
Difficult to grow
•
Not routinely cultured
•
Can be cultivated in Weinmans or Tobies medium
DR MONIKA RAJANI
ANIMAL INOCULATION
•
Inoculation of specimens to
white rat or white
mice.
•
Highly sensitive.
DR MONIKA RAJANI
Serology
•
Antibody detection
-
(within 2-3 weeks)
•
Indirect
H
emagglutination
•
Indirect
I
mmunofluroscence
•
ELISA
•
CFT
•
Card agglutination
trypanosomiasis
test(CATT)
DR MONIKA RAJANI
Serology
•
Antigen detection:
•
Detected from serum or CSF by ELISA.
Molecular tests:
•
PCR
Imaging:
•
CT scan brain
:cerebral edema
•
MRI:
white matter enhancement
.
DR MONIKA RAJANI
Treatment
•
T brucei gambiense:
Pentamidine
•
T brucei rhodesiense:
Suramin
•
In case of CNS involvement :
Melarsoprol(Mel B)
is
DOC.
•
Prophylaxis
: control of flies
Personal protection
No vaccine is available
DR MONIKA RAJANI
Trypanosoma cruzi
•
Chagas disease or South American Trypanosomiasis.
•
Zoonotic disease.
DR MONIKA RAJANI
Habitat
•
In humans:
•
Amastigote forms
: intracellular
parasites
:Seen in muscular tissue,
nervous tissue
and RES.
•
Trypomastigote
forms
:peripheral blood
•
In reduvid bug:
•
Epimastigote
forms
: midgut
•
Metacyclic
trypomastigote
forms
:hind gut and feces
DR MONIKA RAJANI
Morphology
•
Amastigote forms:
•
Oval bodies(2-4um in diameter)
•
Have nucleus,kinetoplast
•
Flagellum is absent
•
Multiplication of parasite occures at this stage
•
Seen In
humans
•
Seen in muscles,nerve cells and RES.
DR MONIKA RAJANI
Morphology
•
Trypomastigote forms:
•
Non multiplying forms
•
Seen in peripheral blood
of humans
•
Long slender forms
•
Nucleus,kinetoplast and
flagellum present
•
Taken up by insect
vectors.
DR MONIKA RAJANI
Morphology
•
Epimastigote forms
:
•
Found in
insect vector
- reduvid bug
•
Also seen in
culture
•
Intermediate form
s
•
Metacyclic trypomastigote forms
DR MONIKA RAJANI
Life cycle
•
Two hosts required
:
•
Man
-definitive host
•
Intermediate host (vector)-
reduviid bug
•
Reservoir hos
t
:
Armadillo,cat,dogs
•
Infective form
:
•
metacyclic trypomastigote
forms
DR MONIKA RAJANI
Mode of transmission
•
When m.m,conjunctiva,wound on skin is
contaminated by feces of bug containing metacyclic
trypanomastigotes.
•
Blood transfusion
•
Organ transplant
•
Vertical transmission
DR MONIKA RAJANI
Life cycle
DR MONIKA RAJANI
Clinical features
•
Acute Chagas disease:
•
seen usually in
children less than two years
of age
•
Occures soon after infection and may last for 1-4 months
•
Chagoma
:subcutaneous manifestation at site of inoculation.
•
Romanas sign:
Classical finding of acute Chagas disease
:inoculation of parasite in conjunctiva.
:Unilateral painless edema of perioccular tissues.
•
Fever,lymphadenopathy,HSM.
•
Acute myocarditis,meningoencephalitis.
•
Symptoms resolve within 4-8 weeks at pts enter chronic
phase.
DR MONIKA RAJANI
Clinical features in chagas disease
DR MONIKA RAJANI
Clinical features
•
Chronic Chagas disease:
•
Seen in adults and older children.
•
Cardiac myopathy
•
Megacolon
•
Mega esoph
agus.
•
Congenital infection
:
•
Myocardial and neurological damage to fetus
DR MONIKA RAJANI
Lab diagnosis
•
Micoscopy :
•
Sample
:fresh
anticoagulated blood or
buffy coat
•
Wet mount
: snake like
motion of trypomastigotes
•
Giemsa stained
thick and
thin peripheral
smears-
trypomastigote forms
•
Acridine orange
stains
DR MONIKA RAJANI
Culture
•
Novy,Neal and Nicolle
(NNN) medium
•
Inoculated with blood and
other specimens.
•
Incubated at 22-24 C till 4
weeks.
•
Epimastigote and
Trypomastigote forms
are
found in culture.
DR MONIKA RAJANI
Animal inoculation
•
Guinea pig or mice are inoculated with blood etc.
•
Trypomastigote forms are looked for in its blood
smears few days later.
Histopathology
•
Biopsy examination of muscles,lymph node aspirates
may reveal amastigote forms.
Intradermal test:
•
Antigen cruzin is prepared from T cruzi culture and
used for i.d test
•
Delayed hypersenstivity reaction
occures
DR MONIKA RAJANI
Xeno diagnosis
•
Bugs are reared in trypanosome free lab and starved
for 2 weeks.
•
They are then fed on patients blood.
•
If trypanomastigotes are ingested they will multiply
in gut of bug
•
Trypanomastigotes can be found in feces of bug 2
weeks later.
DR MONIKA RAJANI
Serology
•
Antigen detect
ion:
•
In urine and sera by ELISA.
•
Antibody detection
:
•
IHA
•
ELISA
•
CFT
•
DAT
•
RADIOIMMUNE PRECIPITATION ASSAY
DR MONIKA RAJANI
Molecular tests
•
PCR
•
Other tests:
•
ECG
•
Endoscopy
DR MONIKA RAJANI
Treatment
•
Nifutrimox
•
Benznidazole
•
Only extracellular forms are killed.
DR MONIKA RAJANI
OBJECTIVE QUESTIONS
DR MONIKA RAJANI
Parasites detected in peripheral blood
•
Trypanosomes
•
Leishmania
•
Plasmodium spp
•
Babesia spp
DR MONIKA RAJANI
Obligate intracellular parasites
•
T cruzi
•
Leishmania spp
•
Plasmodium spp
•
Babesia spp
•
Toxoplasma
DR MONIKA RAJANI
Parasites involving heart
•
T brucei
•
T cruzi
•
Toxoplasma
•
Trichinella
•
Echinococcus granulosus
DR MONIKA RAJANI
THANK YOU
DR MONIKA RAJANI
Trypanosomes are hemoflagellates that reside in the blood and tissues of vertebrate hosts and insect vectors. They undergo a complex life cycle involving two hosts and different developmental stages. Trypanosomes cause diseases like African Trypanosomiasis (sleeping sickness) and South American Trypanosomiasis (Chagas disease). The Trypanosoma Brucei complex is known to cause sleeping sickness in humans and other vertebrate hosts. The morphology of vertebrate forms includes various shapes and movements, often observed in blood films. Development in vectors occurs through two modes: Salivaria and Stercoraria.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
HEMOFLAGELLATES- TRYPANOSOMES DR MONIKA RAJANI ASSOCIATE PROFESSOR , DEPT OF MICROBIOLOGY CIMSH ,LKO DR MONIKA RAJANI
Classification B-SUPERCLASS MASTIGOPHORA 1-INTESTINAL FLAGELLATE -Giardia intestinalis 2-GENITAL FLAGELLATE- Trichomonas vaginalis 3-BLOOD AND TISSUE FLAGELLATES- Trypanosoma Leishmania DR MONIKA RAJANI
General characteristics Live in blood and tissues of man and other vertebrate hosts and in gut of insect vectors. Life cycle in two hosts: vertebrate hosts(definitive host) and insect vectors(intermediate host). Trypomastigote and amastigote main stages in life cycle Epimastigote and promastigote forms are also seen. Multiplication occures by binary fission. No sexual cycle is known. Two modes of development in vectors: salivaria and stercoraria. DR MONIKA RAJANI
Morphological forms Different stages Trypomastigote stage DR MONIKA RAJANI
Development in vector Salivaria: trypanosomes migrate to mouth parts of vectors such that infection is transmitted by their bite. eg T gambiense ,T rhodesiense by bite of tsetse fly Stercoraria: Trypanosomes migrate to hind gut and are passed in feces. eg: T cruzi- Chagasdisease-acquired by rubbing feces of vector bug into wound caused by its bite. DR MONIKA RAJANI
Distribution I: African Trypanosomiasis: sleeping sickness Caused by Trypanosoma brucei complex (T brucei gambiense, T brucei rhodesiense). II: South American Trypanosomiasis: Chagas disease. Caused by T cruzi DR MONIKA RAJANI
Trypanosoma Brucei complex Sleeping sickness Habitat: man and other vertebrate host. :blood, lymph nodes,CNS,connective tissues. DR MONIKA RAJANI
Morphology -Vertebrate forms Trypomastigote form : pleomorphic :long slender forms, short stumpy forms and intermediate forms. :in blood films seen as colourless spindle shaped bodies :move rapidly spinning around cells :Giemsa stain: cytoplasm pale blue and nucleus is red :kinetoplast as red dot :flagellum is red DR MONIKA RAJANI
Morphology Insect forms Epimastigote forms Metacyclic Trypomastigote forms DR MONIKA RAJANI
LIFE CYCLE Two hosts: Vertebrate host: man,game animals and domestic animals Invertebrate host: tse tse fly(male and female flies of Glossina spp) Infective form:metacyclic trypanomastigote forms are infective to humans. Mode of transmission:bite of tse tse fly :Congenital transmission Reservoir: man is the only reservoir host. DR MONIKA RAJANI
Life Cycle DR MONIKA RAJANI
Clinical features West African sleeping sickness(chronic disease). Painless chancre at site of bite Fever,chills,rash,anemia,headache Winter Bottoms sign - Hepato spleenomegaly, lymphadenopathy in posterior cervical region. Myocarditis Hematological manifestations. CNS manifestations: headache mental dullness,apathy Day time sleepiness. Profound coma Death DR MONIKA RAJANI
Lab diagnosis Routine tests: Blood picture-anemia WBC raised,DLC-monocytosis ESR-raised Reversal of albumin globulin ratio CSF:raised pressure,cell counts and proteins DR MONIKA RAJANI
Lab diagnosis Specific tests: Sample: peripheral blood bone marrow lymph node aspirate CSF chance fluid. DR MONIKA RAJANI
Microscopy Wet mount preparation :demonstration of trypomastigote forms. Giemsa stain of thick peripheral smears. Concentration techniques:buffy coat :Membrane filtration methods DR MONIKA RAJANI
Culture Difficult to grow Not routinely cultured Can be cultivated in Weinmans or Tobies medium DR MONIKA RAJANI
ANIMAL INOCULATION Inoculation of specimens to white rat or white mice. Highly sensitive. DR MONIKA RAJANI
Serology Antibody detection- (within 2-3 weeks) Indirect Hemagglutination Indirect Immunofluroscence ELISA CFT Card agglutination trypanosomiasis test(CATT) DR MONIKA RAJANI
Serology Antigen detection: Detected from serum or CSF by ELISA. Molecular tests: PCR Imaging: CT scan brain:cerebral edema MRI:white matter enhancement. DR MONIKA RAJANI
Treatment T brucei gambiense: Pentamidine T brucei rhodesiense: Suramin In case of CNS involvement : Melarsoprol(Mel B) is DOC. Prophylaxis: control of flies Personal protection No vaccine is available DR MONIKA RAJANI
Trypanosoma cruzi Chagas disease or South American Trypanosomiasis. Zoonotic disease. DR MONIKA RAJANI
Habitat In humans: Amastigote forms: intracellular parasites :Seen in muscular tissue, nervous tissue and RES. Trypomastigote forms:peripheral blood In reduvid bug: Epimastigote forms: midgut Metacyclic trypomastigote forms:hind gut and feces DR MONIKA RAJANI
Morphology Amastigote forms: Oval bodies(2-4um in diameter) Have nucleus,kinetoplast Flagellum is absent Multiplication of parasite occures at this stage Seen In humans Seen in muscles,nerve cells and RES. DR MONIKA RAJANI
Morphology Trypomastigote forms: Non multiplying forms Seen in peripheral blood of humans Long slender forms Nucleus,kinetoplast and flagellum present Taken up by insect vectors. DR MONIKA RAJANI
Morphology Epimastigote forms: Found in insect vector- reduvid bug Also seen in culture Intermediate forms Metacyclic trypomastigote forms DR MONIKA RAJANI
Life cycle Two hosts required: Man-definitive host Intermediate host (vector)- reduviid bug Reservoir host: Armadillo,cat,dogs Infective form: metacyclic trypomastigote forms DR MONIKA RAJANI
Mode of transmission When m.m,conjunctiva,wound on skin is contaminated by feces of bug containing metacyclic trypanomastigotes. Blood transfusion Organ transplant Vertical transmission DR MONIKA RAJANI
Life cycle DR MONIKA RAJANI
Clinical features Acute Chagas disease: seen usually in children less than two years of age Occures soon after infection and may last for 1-4 months Chagoma:subcutaneous manifestation at site of inoculation. Romanas sign: Classical finding of acute Chagas disease :inoculation of parasite in conjunctiva. :Unilateral painless edema of perioccular tissues. Fever,lymphadenopathy,HSM. Acute myocarditis,meningoencephalitis. Symptoms resolve within 4-8 weeks at pts enter chronic phase. DR MONIKA RAJANI
Clinical features in chagas disease DR MONIKA RAJANI
Clinical features Chronic Chagas disease: Seen in adults and older children. Cardiac myopathy Megacolon Mega esophagus. Congenital infection: Myocardial and neurological damage to fetus DR MONIKA RAJANI
Lab diagnosis Micoscopy : Sample:fresh anticoagulated blood or buffy coat Wet mount: snake like motion of trypomastigotes Giemsa stained thick and thin peripheral smears- trypomastigote forms Acridine orange stains DR MONIKA RAJANI
Culture Novy,Neal and Nicolle (NNN) medium Inoculated with blood and other specimens. Incubated at 22-24 C till 4 weeks. Epimastigote and Trypomastigote forms are found in culture. DR MONIKA RAJANI
Animal inoculation Guinea pig or mice are inoculated with blood etc. Trypomastigote forms are looked for in its blood smears few days later. Histopathology Biopsy examination of muscles,lymph node aspirates may reveal amastigote forms. Intradermal test: Antigen cruzin is prepared from T cruzi culture and used for i.d test Delayed hypersenstivity reaction occures DR MONIKA RAJANI
Xeno diagnosis Bugs are reared in trypanosome free lab and starved for 2 weeks. They are then fed on patients blood. If trypanomastigotes are ingested they will multiply in gut of bug Trypanomastigotes can be found in feces of bug 2 weeks later. DR MONIKA RAJANI
Serology Antigen detection: In urine and sera by ELISA. Antibody detection: IHA ELISA CFT DAT RADIOIMMUNE PRECIPITATION ASSAY DR MONIKA RAJANI
Molecular tests PCR Other tests: ECG Endoscopy DR MONIKA RAJANI
Treatment Nifutrimox Benznidazole Only extracellular forms are killed. DR MONIKA RAJANI
OBJECTIVE QUESTIONS DR MONIKA RAJANI
Parasites detected in peripheral blood Trypanosomes Leishmania Plasmodium spp Babesia spp DR MONIKA RAJANI
Obligate intracellular parasites T cruzi Leishmania spp Plasmodium spp Babesia spp Toxoplasma DR MONIKA RAJANI
Parasites involving heart T brucei T cruzi Toxoplasma Trichinella Echinococcus granulosus DR MONIKA RAJANI
THANK YOU DR MONIKA RAJANI