Opioid Misuse and Prescription Drug Guidelines

O
p
i
o
i
d
s
–
A
P
h
a
r
m
a
c
e
u
t
i
c
a
l
P
e
r
s
p
e
c
t
i
v
e
o
n
P
r
e
s
c
r
i
p
t
i
o
n
D
r
u
g
s
Carol Ott, PharmD, BCPP
Clinical Professor of Pharmacy Practice
Clinical Pharmacy Specialist, Outpatient Psychiatry
Eskenazi Health, Indianapolis

Disclosures
•
The speaker has no conflicts of interest to disclose.
•
Consultant – Tippecanoe County Public Defender’s Office
•
Consultant – IU/Dept of Child Services Psychopharmacology Group
•
Member/Chair – Indiana Medicaid Drug Utilization Review Board
•
Member – Indiana Medicaid Mental Health Quality Advisory
Committee
•
Member – Board of Directors – NAMI West Central Indiana
Pain as the 5
th
Vital Sign
Where are Misused Prescription Opioids Coming From?
SAMHSA. NSDUH Data Review, Sept 2016. www.samhsa.gov
Prescription Opioids – Non-Medical Use
SAMHSA Center for Behavioral Health Statistics and Quality,
NSDUH 2014-2015, Jan 2017. www.samhsa.gov
Heroin Use, Past Year, Adults 18 – 25, 2014-2015
SAMHSA Center for Behavioral Health Statistics and Quality,
NSDUH 2014-2015, Jan 2017. www.samhsa.gov
CDC Guidelines to Limit Opioid Prescribing
•
Prefer to start with non-drug therapy and non-opioid medications
•
Have goals for pain and functioning
•
Use immediate-release opioids instead of extended-release for no
more than 7 days for acute pain
•
Use lowest effective dose, lines out when increased monitoring is
required
•
Review history of and risk factors for substance use
•
Use the prescription drug monitoring program for controlled
substance prescriptions
•
Urine drug screening with chronic opioid therapy
Indiana Medicaid Opioid Regulations/Limits
•
Prior authorizations (PA) in place for opioid drug therapy
•
Prefer immediate-release products with 7-day treatment limit without PA
•
Long-acting products require PA
•
Follows CDC and Indiana Medical Licensing Board opioid prescribing rules
•
Covers methadone treatment in a narcotic treatment program (methadone
clinic) as part of the medical billing
•
PA for Suboxone (buprenorphine/naloxone) has been suspended as of Dec 1,
2017 with monitoring of treatment program after prescribing
•
Vivitrol (naltrexone) long-acting injection requires PA for some insurers
Medication-Assisted Treatment for Opioid
Use Disorder
•
Methadone – is an opioid – considered to be maintenance
replacement therapy, must be administered under directly-observed
daily clinic visits
•
Buprenorphine – is an opioid, but can become an opioid-blocker with
higher doses, most often given in combination with naloxone to
prevent injection use, prescribers must have a waiver to prescribe,
does not require daily clinic visits, considered to be maintenance
replacement therapy
•
Naltrexone – opioid-blocker – most often used in long-acting injection
form given every 28 days, considered to be abstinence therapy
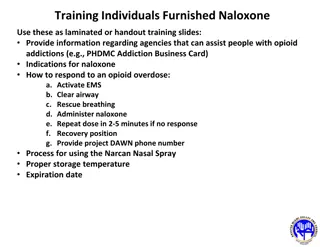
Naloxone
•
Aaron’s Law – July 2015 – removes civil liability from a pharmacist for
dispensing naloxone at a community pharmacy
•
Pharmacies can dispense naloxone kits without a prescription under a
standing order between a prescriber (state health commissioner) and
a pharmacy/pharmacist
•
Two doses of naloxone per dispensing to allow for enough doses for
EMTs to arrive
•
Indiana Medicaid covers naloxone kits in a limited number per year
Criminal Justice Issues
•
County jails do have medical providers, but don’t always have
substance abuse evaluations or treatment
•
Inmates go through detoxification in jail since they don’t have access
to drugs
•
May leave jail and go back to the same life without intervention with
psychosocial services
•
Generally don’t have insurance or Medicaid, so there is no way to pay
for treatment once the inmate leaves jail
•
Some jails are working on addictions treatment programs within the
jail or community corrections
Explore the pharmaceutical perspective on prescription opioids, the impact of pain as a vital sign, sources of misused prescription opioids, non-medical use statistics, heroin trends, and CDC guidelines to limit opioid prescribing. Gain insights on the complexities surrounding opioid misuse and the importance of proper prescribing practices.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Opioids Opioids A Pharmaceutical A Pharmaceutical Perspective on Prescription Drugs Perspective on Prescription Drugs Carol Ott, PharmD, BCPP Clinical Professor of Pharmacy Practice Clinical Pharmacy Specialist, Outpatient Psychiatry Eskenazi Health, Indianapolis
Disclosures The speaker has no conflicts of interest to disclose. Consultant Tippecanoe County Public Defender s Office Consultant IU/Dept of Child Services Psychopharmacology Group Member/Chair Indiana Medicaid Drug Utilization Review Board Member Indiana Medicaid Mental Health Quality Advisory Committee Member Board of Directors NAMI West Central Indiana
Pain as the 5thVital Sign First recognized in the 1990s AMA 2016 pain is not a vital sign, it is a symptom that cannot be measured like blood pressure Heavy marketing by pharmaceutical manufacturers to use their products AMA recommends removing pain as a vital sign Concern by critics that pain would be ignored Does Pain as the 5thvital sign increase prescribing of opioids?
Where are Misused Prescription Opioids Coming From? SAMHSA. NSDUH Data Review, Sept 2016. www.samhsa.gov
Prescription Opioids Non-Medical Use SAMHSA Center for Behavioral Health Statistics and Quality, NSDUH 2014-2015, Jan 2017. www.samhsa.gov
Heroin Use, Past Year, Adults 18 25, 2014-2015 SAMHSA Center for Behavioral Health Statistics and Quality, NSDUH 2014-2015, Jan 2017. www.samhsa.gov
CDC Guidelines to Limit Opioid Prescribing Prefer to start with non-drug therapy and non-opioid medications Have goals for pain and functioning Use immediate-release opioids instead of extended-release for no more than 7 days for acute pain Use lowest effective dose, lines out when increased monitoring is required Review history of and risk factors for substance use Use the prescription drug monitoring program for controlled substance prescriptions Urine drug screening with chronic opioid therapy
Indiana Medicaid Opioid Regulations/Limits Prior authorizations (PA) in place for opioid drug therapy Prefer immediate-release products with 7-day treatment limit without PA Long-acting products require PA Follows CDC and Indiana Medical Licensing Board opioid prescribing rules Covers methadone treatment in a narcotic treatment program (methadone clinic) as part of the medical billing PA for Suboxone (buprenorphine/naloxone) has been suspended as of Dec 1, 2017 with monitoring of treatment program after prescribing Vivitrol (naltrexone) long-acting injection requires PA for some insurers
Medication-Assisted Treatment for Opioid Use Disorder Methadone is an opioid considered to be maintenance replacement therapy, must be administered under directly-observed daily clinic visits Buprenorphine is an opioid, but can become an opioid-blocker with higher doses, most often given in combination with naloxone to prevent injection use, prescribers must have a waiver to prescribe, does not require daily clinic visits, considered to be maintenance replacement therapy Naltrexone opioid-blocker most often used in long-acting injection form given every 28 days, considered to be abstinence therapy
Naloxone Aaron s Law July 2015 removes civil liability from a pharmacist for dispensing naloxone at a community pharmacy Pharmacies can dispense naloxone kits without a prescription under a standing order between a prescriber (state health commissioner) and a pharmacy/pharmacist Two doses of naloxone per dispensing to allow for enough doses for EMTs to arrive Indiana Medicaid covers naloxone kits in a limited number per year
Criminal Justice Issues County jails do have medical providers, but don t always have substance abuse evaluations or treatment Inmates go through detoxification in jail since they don t have access to drugs May leave jail and go back to the same life without intervention with psychosocial services Generally don t have insurance or Medicaid, so there is no way to pay for treatment once the inmate leaves jail Some jails are working on addictions treatment programs within the jail or community corrections