Integrated Care System Framework in North West London







N
o
r
t
h
W
e
s
t
L
o
n
d
o
n
I
C
S
:
S
y
s
t
e
m
F
r
a
m
e
w
o
r
k
t
o
d
e
l
i
v
e
r
o
u
r
o
b
j
e
c
t
i
v
e
s
S
e
p
t
e
m
b
e
r
2
0
2
3



I
n
t
r
o
d
u
c
t
i
o
n
t
o
N
W
L
o
n
d
o
n
a
n
d
t
h
e
I
n
t
e
g
r
a
t
e
d
C
a
r
e
S
y
s
t
e
m
(
I
C
S
)
Proposed operating framework (or how decisions are made)
•
Strategy and planning including financial allocations
•
Delivery of care and interventions
•
Assurance
Relative roles of key players
•
Borough/Place Based Partnerships (including public health, primary care, community & mental health, social services,
acute care where required)
•
Provider Collaboratives
•
ICS wide programmes and the ICB
1
W
h
a
t
t
h
i
s
p
r
e
s
e
n
t
a
t
i
o
n
c
o
v
e
r
s

2

N
W
L
o
n
d
o
n
h
a
s
a
p
o
p
u
l
a
t
i
o
n
o
f
a
r
o
u
n
d
2
.
1
m
i
l
l
i
o
n
,
i
s
r
e
l
a
t
i
v
e
l
y
y
o
u
n
g
a
n
d
r
e
l
a
t
i
v
e
l
y
d
i
v
e
r
s
e
Toby to get a number
re diversity
3
I
C
S
h
a
s
f
o
u
r
o
b
j
e
c
t
i
v
e
s
•
I
m
p
r
o
v
e
o
u
t
c
o
m
e
s
i
n
p
o
p
u
l
a
t
i
o
n
h
e
a
l
t
h
a
n
d
h
e
a
l
t
h
c
a
r
e
•
P
r
e
v
e
n
t
i
l
l
-
h
e
a
l
t
h
a
n
d
t
a
c
k
l
e
i
n
e
q
u
a
l
i
t
i
e
s
i
n
o
u
t
c
o
m
e
s
,
e
x
p
e
r
i
e
n
c
e
,
a
c
c
e
s
s
t
o
c
a
r
e
•
E
n
h
a
n
c
e
p
r
o
d
u
c
t
i
v
i
t
y
a
n
d
v
a
l
u
e
f
o
r
m
o
n
e
y
•
S
u
p
p
o
r
t
b
r
o
a
d
e
r
e
c
o
n
o
m
i
c
a
n
d
s
o
c
i
a
l
d
e
v
e
l
o
p
m
e
n
t
W
e
h
a
v
e
c
o
n
t
i
n
u
e
d
o
u
r
f
o
c
u
s
o
n
i
m
p
r
o
v
i
n
g
a
c
c
e
s
s
t
o
c
a
r
e
a
n
d
h
e
a
l
t
h
o
u
t
c
o
m
e
s
…
.
.
•
Improved quality of primary care e.g. diabetes
care, focus on cervical screening
•
Continued to significantly increase capacity in
mental health care with 7% increase in funding
year on year
•
Established focused urgent and emergency care
services for people with acute mental health
problems
•
Reduced rates of emergency admissions
•
Reduced very long waits for outpatients and
surgery
•
Operationalising elective care centre at CMH
•
Improved access to diagnostic services
4
D
e
v
e
l
o
p
m
e
n
t
s
o
v
e
r
t
h
e
l
a
s
t
y
e
a
r
…
B
u
t
c
o
n
t
i
n
u
e
t
o
f
a
c
e
c
o
n
s
i
d
e
r
a
b
l
e
c
h
a
l
l
e
n
g
e
s
•
Overall life expectancy continues to fall with
considerable variation between populations
•
Increasing rates of obesity
•
Still considerable challenges for many/most in accessing
primary care with slow progress towards new models of
care
•
Over 250,000 waiting for an outpatient or inpatient
procedure
•
Median time for first contact with CAMHS is 10 days but
considerable variation by geography and between first
and second contact
•
Length of stay increasing with continued challenges in
discharges resulting in poor use of resources and
deterioration for patients
What else to add?
5
W
e
h
a
v
e
s
e
t
o
u
t
o
u
r
s
t
r
a
t
e
g
y
a
n
d
p
r
i
o
r
i
t
i
e
s
f
o
r
t
h
e
n
e
x
t
f
i
v
e
y
e
a
r
s
Support health and well being
Address inequalities in health
Improve access
Provide care closer to home
Improve productivity & quality of
care
Ensure happy, healthy lives
for children and young people
6
W
e
h
a
v
e
s
e
t
o
u
t
o
u
r
s
t
r
a
t
e
g
y
a
n
d
p
r
i
o
r
i
t
i
e
s
f
o
r
t
h
e
n
e
x
t
f
i
v
e
y
e
a
r
s
(
1
/
2
)
•
Provide employment opportunities for
residents;
•
Commit to the London living wage.
•
Reduce rates of smoking
•
Improve diet and increase exercise, including
improving rates of breastfeeding
•
Increase uptake of the rewind programme to
reverse pre-diabetes
•
Better identify people at risk of high blood
pressure, and better engage them
•
Increase the uptake of preventative services
•
Continue focus on the wider determinants and
inequalities
•
Develop consistency of scope and
quality of services across NWL
•
Focus resource and differentiate
services for groups with poor
outcomes, e.g. black women and
childbirth
•
Build confidence in communities to
come forward for care and support
•
Reduce barriers to care for black and
other ethnic minority groups;
•
Provide bespoke programmes for
most marginalised groups (i.e., SEND
and employment)
•
Expand preventative services, in
particular tackling obesity and
improve healthy weight in early
childhood; increase breastfeeding
rates; improve immunisation rates;
improve oral health
•
Expand access to mental health
support through schools, children’s
health hubs and digital tools
•
Develop consistent, ‘right person first
time’ core models of care through
child health and family hubs
S
u
p
p
o
r
t
h
e
a
l
t
h
a
n
d
w
e
l
l
b
e
i
n
g
A
d
d
r
e
s
s
i
n
e
q
u
a
l
i
t
i
e
s
i
n
h
e
a
l
t
h
E
n
s
u
r
e
h
a
p
p
y
,
h
e
a
l
t
h
y
l
i
v
e
s
f
o
r
c
h
i
l
d
r
e
n
a
n
d
y
o
u
n
g
p
e
o
p
l
e
7
W
e
h
a
v
e
s
e
t
o
u
t
o
u
r
s
t
r
a
t
e
g
y
a
n
d
p
r
i
o
r
i
t
i
e
s
f
o
r
t
h
e
n
e
x
t
f
i
v
e
y
e
a
r
s
(
2
/
2
)
•
Reduce hospital and care home
admissions through improved
local care;
•
Utilise voluntary providers to
support residents after
discharge;
•
Put in place a care plan for
people with an ongoing health or
care need
•
Develop/ roll out integrated
neighbourhood teams to bring
community MH, primary
community, and social care
together locally
•
Implement innovative, cost-effective models of
care in cardiovascular, cancer and children’s
mental health
•
Ensure seamless pathways from general
practice to hospitals and back home again
•
Develop workforce transformation plans
•
Use digital tools to identify those residents most
at risk of and direct early interventions
•
Use data to understand where resources could
be used more effectively, e.g. to predict demand
and manage capacity; to evaluate which
services deliver benefits to which residents
•
Ensure that estate is fit for purpose and better
utilised
•
Rationalise channels for simple urgent care and
streamline access
•
Implement local integrated response to urgent
demand
•
Establish and expand a live Directory of
Services
•
Expand use and capacity of virtual wards
•
Institute more efficient planned surgical centres
•
Redesign access to specialist expertise and
diagnosis
•
Increase mental health capacity including for
people with autism, dementia and learning
disabilities
•
Expand digital technologies
•
Detailed review of emergency care pathways
P
r
o
v
i
d
e
c
a
r
e
c
l
o
s
e
r
t
o
h
o
m
e
I
m
p
r
o
v
e
p
r
o
d
u
c
t
i
v
i
t
y
&
q
u
a
l
i
t
y
o
f
c
a
r
e
I
m
p
r
o
v
e
a
c
c
e
s
s
F
i
v
e
c
o
r
e
d
e
l
i
v
e
r
y
p
r
o
g
r
a
m
m
e
s
:
1.
Improve health and reduce inequalities
2.
Improve access to, and quality and efficiency of, local
care including primary,
social
& community care
3.
Improve access to, and quality and efficiency of, mental
health care services and services supporting learning
disabilities and autism
4.
Improve urgent and emergency care access
5.
Transform planned care to reduce waiting lists
8
W
e
a
r
e
d
e
v
e
l
o
p
i
n
g
d
e
t
a
i
l
e
d
i
m
p
l
e
m
e
n
t
a
t
i
o
n
p
l
a
n
s
a
c
r
o
s
s
t
h
e
1
3
c
o
r
e
p
r
o
g
r
a
m
m
e
s
F
i
v
e
e
n
a
b
l
i
n
g
p
r
o
g
r
a
m
m
e
s
:
6.
Rapidly adopt digital technologies across all services
7.
Utilise data and analytics to improve access, productivity
and quality of care – and support research
8.
Drive research and adopt innovative approaches to
support the ICS objectives
9.
Improve quality and utilisation of estate
10.
Transform the workforce
T
h
r
e
e
p
r
i
o
r
i
t
y
c
l
i
n
i
c
a
l
/
u
s
e
r
a
r
e
a
s
1
1
.
C
a
n
c
e
r
1
2
.
C
h
i
l
d
r
e
n
&
Y
o
u
n
g
P
e
o
p
l
e
1
3
.
M
a
t
e
r
n
i
t
y
Social care??
9
W
h
a
t
d
o
e
s
a
g
r
e
a
t
p
r
o
g
r
a
m
m
e
l
o
o
k
l
i
k
e
Add programme health – clear TOR, specification,
align objectives, outcomes, co-production,
membership , metrics
10
W
e
h
a
v
e
e
s
t
a
b
l
i
s
h
e
d
e
i
g
h
t
B
o
r
o
u
g
h
/
P
l
a
c
e
B
a
s
e
d
P
a
r
t
n
e
r
s
h
i
p
s
(
B
B
P
s
)
a
n
d
P
r
o
v
i
d
e
r
C
o
l
l
a
b
o
r
a
t
i
v
e
s
.
B
B
P
s
b
r
i
n
g
t
o
g
e
t
h
e
r
p
r
i
m
a
r
y
c
a
r
e
,
s
o
c
i
a
l
c
a
r
e
,
p
u
b
l
i
c
h
e
a
l
t
h
,
m
e
n
t
a
l
h
e
a
l
t
h
a
n
d
c
o
m
m
u
n
i
t
y
c
a
r
e
w
i
t
h
i
n
a
B
o
r
o
u
g
h
–
a
n
d
w
o
r
k
c
l
o
s
e
l
y
w
i
t
h
t
h
e
v
o
l
u
n
t
a
r
y
a
n
d
a
c
u
t
e
s
e
c
t
o
r
Hillingdo
n
BBP
PCN
/INTs*
x
6
Hounslo
w
BBP
B
r
en
t
BBP
Community
and
M
ental
H
ealth
C
are
C
ollaborative
(covers four Trusts)
Acute
Care
Collaborative
(covers four Trusts)
Ealin
g
BBP
Har
r
o
w
BBP
Hammersmit
h
&
Fulham
BBP
Kensingto
n
&
Chelsea
BBP
W
estminste
r
BBP
B
i
-
b
o
r
o
u
g
h
PCN
/INTs
x
6
PCN
/INTs
x
6
PCN
/INTs
x
6
PCN
/INTs
x
6
PCN
/INTs
x
6
*
Primary Care Networks, transitioning to Integrated Neighbourhood Teams
PCN
/INTs
x
5
PCN
/INTs
x
4
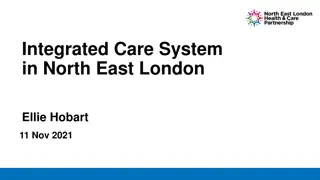
Integrated Care Board supports across the system
11
I
C
B
g
o
v
e
r
n
a
n
c
e
s
t
r
u
c
t
u
r
e
a
l
i
g
n
e
d
t
o
c
o
r
e
f
u
n
c
t
i
o
n
s
Integrated Care Partnership
ICB Board
Audit & Risk
Committee
(statutory)
Remuneration
Committee
(statutory)
Health & Well-being
Boards x 8
ICB Executive
Team
ICS Programme
Boards
Strategic
Commissioning
Committee
Contracting
Committee
Performance*
Committee
Joint Oversight
(Health & Social
Care)
Committees
* Performance covers quality of care, productivity, impact on health outcomes and inequalities in health and wider economic and social growth
Introduction to NW London and the Integrated Care System (ICS)
P
r
o
p
o
s
e
d
o
p
e
r
a
t
i
n
g
f
r
a
m
e
w
o
r
k
(
o
r
h
o
w
d
e
c
i
s
i
o
n
s
a
r
e
m
a
d
e
)
•
S
t
r
a
t
e
g
y
a
n
d
p
l
a
n
n
i
n
g
i
n
c
l
u
d
i
n
g
f
i
n
a
n
c
i
a
l
a
l
l
o
c
a
t
i
o
n
s
•
D
e
l
i
v
e
r
y
o
f
c
a
r
e
a
n
d
i
n
t
e
r
v
e
n
t
i
o
n
s
•
A
s
s
u
r
a
n
c
e
Relative roles of key players
•
Borough/Place Based Partnerships (including public health, primary care, community & mental health , social services ,
acute care)
•
Provider Collaboratives
•
ICS wide programmes and the ICB
12
W
h
a
t
t
h
i
s
p
r
e
s
e
n
t
a
t
i
o
n
c
o
v
e
r
s
13
T
h
e
o
p
e
r
a
t
i
n
g
f
r
a
m
e
w
o
r
k
s
e
t
s
o
u
t
h
o
w
t
h
e
I
C
S
w
i
l
l
o
r
g
a
n
i
s
e
a
r
o
u
n
d
t
h
r
e
e
f
u
n
c
t
i
o
n
s
Strategic
commissioning
Assurance of
delivery
Delivery
14
I
n
p
u
t
s
i
n
d
e
v
e
l
o
p
i
n
g
s
t
r
a
t
e
g
y
A
l
i
g
n
e
d
p
r
i
o
r
i
t
i
e
s
a
c
r
o
s
s
t
h
e
s
y
s
t
e
m
(
o
v
e
r
s
e
e
n
b
y
I
n
t
e
g
r
a
t
e
d
C
a
r
e
P
a
r
t
n
e
r
s
h
i
p
)
C
l
i
n
i
c
a
l
i
n
p
u
t
f
r
o
m
C
R
G
s
‘
T
o
p
-
d
o
w
n
’
p
r
i
o
r
i
t
i
e
s
(
n
a
t
i
o
n
a
l
&
r
e
g
i
o
n
a
l
)
S
h
a
r
e
d
b
o
r
o
u
g
h
p
r
i
o
r
i
t
i
e
s
a
n
d
u
n
d
e
r
s
t
a
n
d
i
n
g
o
f
r
e
s
i
d
e
n
t
n
e
e
d
s
P
r
o
g
r
a
m
m
e
s
t
r
a
t
e
g
i
e
s
R
e
s
i
d
e
n
t
&
u
s
e
r
v
i
e
w
s
A
n
a
l
y
s
i
s
o
f
c
u
r
r
e
n
t
p
e
r
f
o
r
m
a
n
c
e
a
n
d
o
p
p
o
r
t
u
n
i
t
i
e
s
R
e
l
a
t
i
v
e
r
o
l
e
s
i
n
d
e
v
e
l
o
p
i
n
g
s
t
r
a
t
e
g
y
a
n
d
p
l
a
n
s
•
Leads on developing and approving
overarching strategy (pulling together
contributions from LAs, ICS programmes,
providers, etc.)
•
Receives and comments on more detailed
strategies and plans across programmes
•
Reviews progress against plans as part of
overall strategic review
•
Develops section of overarching strategy
for specific area of focus
•
Further develops section of overarching
strategy into strategy for own area
(including demand, capacity, resource
allocation, etc.)
•
Translates more detailed strategy into
work streams,and project plans (detailed
year 1 plan, outline 5 year plan)
•
Provide clinical input to strategy
development, setting priorities and
providing input to individual programmes
•
For priority areas in overarching strategy,
CRG provides clinical advice/ support into
more detailed programme or collaborative
strategy
•
Supports development of more detailed
plan where relevant
•
Lead on detailed analysis of population
health needs
•
Ensure borough priorities reflected
•
Translates overarching strategy and local
priorities into more detailed strategy for the
borough
•
Translates strategy and programme plans
into local implementation plans (detailed
year 1 plan, outline 5 year plan)
•
Works up more detailed collaborative and
individual provider strategy building on
overarching strategy and programme
strategies
•
Translates collaborative strategy into
project plans (detailed year 1 plan, outline
5 year plan)
•
Lead on detailed analysis of what is
working/not working
•
Provide input on optimal delivery models
and areas for innovation
E
x
a
m
p
l
e
:
D
e
v
e
l
o
p
i
n
g
M
H
s
t
r
a
t
e
g
y
a
n
d
p
l
a
n
s
I
n
p
u
t
s
(
l
e
a
d
r
e
s
p
o
n
s
i
b
i
l
i
t
y
)
•
Population health needs analysis
(BBPs)
•
Views of users and residents
(ICB comms to coordinate)
•
Current care – levels of activity
and performance (collaboratives)
•
Current care - SWOT analysis,
overview of performance
(collaboratives)
•
Emerging best practice, new
ideas, new approaches (CRGs)
•
NHSE requirements and
recommendations (ICB,
collaboratives)
D
e
v
e
l
o
p
p
r
o
p
o
s
a
l
s
a
n
d
o
p
t
i
o
n
s
(
p
r
o
g
r
a
m
m
e
t
e
a
m
)
•
Set out services/interventions based on clinical
evidence base/national guidance
•
Describe optimal delivery models for priority
interventions (inpatient, outpatient, in person, digital,
scale considerations)
•
Analyse capacity (workforce, space) requirements to
deliver against population needs
•
Set out financial implications based on efficient
working
•
Set out estate and workforce requirements based on
efficient working
•
Outline “ask” for future research and innovation
•
Detail plans to go from here to there over next five
years
T
e
s
t
,
d
i
s
c
u
s
s
,
c
o
n
s
u
l
t
•
Discuss and involve users,
residents, staff, wider
stakeholders in each stage of
developing proposals and plans
•
Amend plans accordingly and/or
set out choices
•
Identify areas needing formal
consultation
Work coordinated by programme team, supported by ICB execs, reporting into ICS
wide programme board and ultimately to the ICP
A
n
a
l
y
s
i
s
-
Need
-
Current spend
-
Evidence base to demonstrate
value add
-
Efficient cost of delivery
-
Deliver within our allocation
17
W
h
e
r
e
w
e
w
a
n
t
t
o
g
e
t
t
o
r
e
f
i
n
a
n
c
i
a
l
a
l
l
o
c
a
t
i
o
n
s
C
o
r
e
p
r
i
n
c
i
p
l
e
s
•
Money follows need
•
Services based on evidence of value add – impact on
outcomes
•
Deliver in most efficient way
A
l
l
o
c
a
t
i
o
n
s
•
Allocate money to maximise outcomes
•
All system partners to deliver care in most efficient and
effective way to improve care & outcomes
•
Providers to deliver core service models in line with
population need & focus on continuous improvement to
improve outcomes
•
Flex the commissioned service to react to local evidenced
population need
18
A
c
t
i
o
n
s
i
n
t
h
e
m
e
a
n
t
i
m
e
•
Deliver our financial targets for 23/24
•
Improve our underlying deficit so our recurrent exit run rate in 23/24 allows us to live within our financial allocation in 24/25
•
Continue to establish a clearer understanding of the “as is” understanding of allocations and outcomes achieved by sector
•
Complete a review of expenditure to understand our contracted expenditure, its funding source and the outcomes /
benefits. This will inform the 24/25 financial planning and commissioning cycle.
•
Continuously improve the design of data led change programmes highest priority conditions and align programmes of work
to drive improvement in resident outcomes – diabetes, heart disease, mental health problems, cancer - to build greater
transparency/analysis re need, impact of interventions and optimal cost of delivery
•
Informed by building better links between population and indicative spend by borough and describe impact on outcomes
and resources from moving to agreed service models across NW London in the highest priority conditions
•
Work on how we unlock the financial benefits of innovation and technology so that organisations can commit to change
•
Work on our capital allocation to link this to the overall ICS strategy
•
Lobby for additional capital resource or the ability to generate our own to increase the amount of capital available
•
Continue working with Boroughs on their estates need and strategy
Borough Based Partnership
Develop a ‘Place lens’, taking a PHM approach
Work in partnership with all local organisations, to
undertake
robust capacity and financial planning within
strategic framework
D
evelop effective relationships between partners to
better inform and effect future service provision
Deliver the ICP strategy and objectives, with specific areas
delegated to Borough/Place, such as Primary Care.
Ensure delivery of core NWL specifications at a Place level
Implement effective Integrated Neighbourhood Teams
that bring together primary care, social care, community,
community MH, voluntary sector and relevant acute
outreach, organised around natural communities of
where people live and work/PCNs.
Develop effective communication, engagement and
partnerships with local residents and communities
Support and enable delivery of the local H&WBB Strategy,
and to be a member of the HWBB.
Ensure effective use of one public estate at Place, and to
oversee the development of the NHS local Estate plan
D
e
l
i
v
e
r
y
o
f
c
a
r
e
ICB and ICS wide programmes
Work in partnership with all local organisations, to
undertake robust capacity and financial planning across
all organisations to ensure delivery of core NWL
specifications
Provide a coordinating function where required to ensure
all partners are able to work in the most efficient and
high quality manner
Develop system wide tools to support optimal service
delivery
Build capacity and capability across the ICS – either
directly or in conjunction with providers;
Identify where services aren’t being delivered optimally,
not sufficiently coordinated and take actions to address
Provider Collaboratives
Work in partnership with all local organisations, to
undertake robust capacity and financial planning within
strategic framework
Develop effective relationships between partners to
better inform and effect service provision
Deliver the ICP strategy and objectives, ensuring delivery
of core NWL specifications
Lead transformation of services where largely within the
remit of the collaborative
Leverage the collective resources of the collaborative to
reduce unwarranted variation in patient outcomes,
access, and experience, and building greater resilience for
services, for example, by sharing capacity and resources.
Work with Integrated Neighbourhood Teams that bring
together primary care, social care, community,
community MH, voluntary sector and relevant acute
outreach, organised around natural communities of
where people live and work/PCNs.
Develop effective communication, engagement and
partnerships with local residents and communities
Ensure effective use of the public estate
A
s
s
u
r
a
n
c
e
–
e
n
s
u
r
i
n
g
a
p
p
r
o
p
r
i
a
t
e
b
a
l
a
n
c
e
a
c
r
o
s
s
l
o
c
a
l
g
o
v
e
r
n
a
n
c
e
a
n
d
I
C
B
g
o
v
e
r
n
a
n
c
e
Need to get to the right data with the right people with appropriate actions
First line of defence sits within provider organisations
SOMs
Regular performance review with data collated by programmes
Moving to a single version of the truth (which would reduce need for data collection, allowing greater focus on improvement)
Focus on improvement as much as performance management
Feedback to strategy
Boroughs to input into performance reviews vis SOMs and programmes
Introduction to NW London and the Integrated Care System (ICS)
Proposed operating framework (or how decisions are made)
•
Strategy and planning including financial allocations
•
Delivery of care and interventions
•
Assurance
R
e
l
a
t
i
v
e
r
o
l
e
s
o
f
k
e
y
p
l
a
y
e
r
s
•
B
o
r
o
u
g
h
/
P
l
a
c
e
B
a
s
e
d
P
a
r
t
n
e
r
s
h
i
p
s
•
P
r
o
v
i
d
e
r
C
o
l
l
a
b
o
r
a
t
i
v
e
s
•
I
C
S
w
i
d
e
p
r
o
g
r
a
m
m
e
s
a
n
d
t
h
e
I
C
B
21
W
h
a
t
t
h
i
s
p
r
e
s
e
n
t
a
t
i
o
n
c
o
v
e
r
s
R
o
l
e
s
o
f
B
o
r
o
u
g
h
B
a
s
e
d
P
a
r
t
n
e
r
s
h
i
p
s
S
t
r
a
t
e
g
y
a
n
d
P
l
a
n
n
i
n
g
•
Build detailed analysis of local
residents’ health and care needs
through JSNA
•
Work with local residents and
communities to understand local
priorities and views on
services/interventions
•
Agree local priorities with health and
well-being boards
•
Work with colleagues across the ICS
to develop strategies for different
services through programmes
•
Input into wider NWL system strategy
•
Developing local plan within syste
m
wide strategy, tailoring services to
meet local needs and enhancing
core NWL standards where required
•
Oversee the development of the
NHS local estate plan.
22
D
e
l
i
v
e
r
y
•
Delivery
of local integrated care
including
the targets and trajectories
that link to the ICS operating plan e
.g.
access targets, vaccination
programmes, referral management,
discharges and screening
•
Coordinate the development of
integrated neighbourhood teams
across organisations to deliver
integrated local health and care
services consistent with the strategy
and ‘blueprints’
•
Lead and drive service transformation
working with and across collaboratives
•
Ensure all service delivery meets local
needs, addressing inequalities,
understanding local communities,
taking a PHM approach
•
Deliver core national and NW London
wide requirements for primary care
A
s
s
u
r
a
n
c
e
•
Continually review quality,
productivity and access to care
across all service areas
•
Ensure all national, regional and
local metrics and regularly monitored
•
Put in place processes for rapid
review of quality data, with a “first
line of defence” approach
•
Ensure governance processes
enable timely and robust review and
challenge of data
R
o
l
e
s
o
f
c
o
l
l
a
b
o
r
a
t
i
v
e
s
(
A
c
u
t
e
,
C
o
m
m
u
n
i
t
y
a
n
d
M
H
T
r
u
s
t
s
)
S
t
r
a
t
e
g
y
a
n
d
P
l
a
n
n
i
n
g
•
Provide input on current care –
what’s working, what’s not
•
Identify areas for innovation and
change – horizon scanning approach
•
Advise on optimal delivery models to
support high quality and productive
care
•
Set out areas for enablers where
change is required
•
Work with clinical reference groups
and programmes to develop
strategies for individual areas and
input into overarching strategy
•
Develop strategy and plans for
collaboratives and individual trusts
and sites in partnership with rest of
system – Joint Forward Plan
23
D
e
l
i
v
e
r
y
•
Delivery
of care including
the targets
and trajectories that link to the ICS
operating plan e
.g.
access targets,
discharges
•
Deliver core national and NW London
wide requirements
•
Work with partners across the ICS to
deliver coordinated and integrated
care across care pathways
•
Lead and drive service transformation
working with and across collaboratives
•
Innovate and evolve where
appropriate
•
Provide mutual support and optimise
service delivery across collaborative
•
Ensure all service delivery meets local
needs, addressing inequalities,
understanding local communities,
taking a PHM approach
A
s
s
u
r
a
n
c
e
•
Continually review quality,
productivity and access to care
across all service areas
•
Ensure all national, regional and
local metrics and regularly monitored
•
Put in place processes for rapid
review of quality data, with a “first
line of defence” approach
•
Ensure governance processes
enable timely and robust review and
challenge of data
R
o
l
e
s
o
f
p
r
o
g
r
a
m
m
e
s
•
Build detailed analysis of population needs, drawing on borough-based analysis and assessment
•
Work with residents and users to understand expectations and views on services, drawing on borough, provider and ICB teams
•
Work with Place/Borough Based Partnerships and Provider Collaboratives to understand what currently works well, what could
be improved, what best practice looks like
•
Work with clinical reference groups to set out best practice care, understand new approaches and innovations
•
Draw on national expertise, evidence base, national guidance and priorities
•
Work with Place/Borough Based Partnerships, clinical reference groups and provider collaboratives to set shared core standards
to ensure equity across NWL;
•
Describe best practice interventions and approaches to deliver optimal outcomes
•
Set, and measure, the appropriate outcomes for each segment of the population;
•
Develop robust demand and capacity models
•
Describe optimal delivery models based on ensuring optimal quality and productiv
ity – and set out what this could mean in NWL
•
Develop options for future delivery models and outline criteria to evaluate
•
Set out implications for digital and data, for workforce development, for estate, for research and innovation
•
Agree metrics for reviewing progress
•
Develop plans to deliver over next
five years with clear responsibilities and timelines/milestones
•
Use contracts and reimbursement mechanisms that incentivise providers – and where necessary, align multiple providers – to
deliver the right level of care effectively at the right cost to deliver the set outcomes;
•
Account for procurement and contract management
24
North West London Integrated Care System (ICS) is aiming to deliver objectives focusing on population health, healthcare outcomes, preventing ill-health, tackling inequalities, enhancing productivity, and supporting economic development. The system involves key players in various partnerships and collaboratives to improve access to care and overall health outcomes by addressing challenges and setting strategic priorities for the future.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
North West London ICS: System Framework to deliver our objectives September 2023 0
1 What this presentation covers Introduction to NW London and the Integrated Care System (ICS) Proposed operating framework (or how decisions are made) Strategy and planning including financial allocations Delivery of care and interventions Assurance Relative roles of key players Borough/Place Based Partnerships (including public health, primary care, community & mental health, social services, acute care where required) Provider Collaboratives ICS wide programmes and the ICB 1
NW London has a population of around 2.1 million, is relatively young and relatively diverse Toby to get a number re diversity Harrow Hillingdon Brent Ealing Westminster Hounslow Kensington and Chelsea Hammersmith & Fulham 12.3% of the population are over the age of 65 (nationalaverageis19%) XXX Global majority backgrounds 2
3 ICS has four objectives Improve outcomes in population health and healthcare Prevent ill-health and tackle inequalities in outcomes, experience, access to care Enhance productivity and value for money Support broader economic and social development 3
4 Developments over the last year What else to add? We have continued our focus on improving access to care and health outcomes .. But continue to face considerable challenges Improved quality of primary care e.g. diabetes care, focus on cervical screening Continued to significantly increase capacity in mental health care with 7% increase in funding year on year Established focused urgent and emergency care services for people with acute mental health problems Reduced rates of emergency admissions Reduced very long waits for outpatients and surgery Operationalising elective care centre at CMH Improved access to diagnostic services Overall life expectancy continues to fall with considerable variation between populations Increasing rates of obesity Still considerable challenges for many/most in accessing primary care with slow progress towards new models of care Over 250,000 waiting for an outpatient or inpatient procedure Median time for first contact with CAMHS is 10 days but considerable variation by geography and between first and second contact Length of stay increasing with continued challenges in discharges resulting in poor use of resources and deterioration for patients 4
5 We have set out our strategy and priorities for the next five years Ensure happy, healthy lives for children and young people Support health and well being Address inequalities in health Improve productivity & quality of care Provide care closer to home Improve access 5
6 We have set out our strategy and priorities for the next five years (1/2) Ensure happy, healthy lives for children and young people Support health and well being Address inequalities in health Provide employment opportunities for residents; Commit to the London living wage. Reduce rates of smoking Improve diet and increase exercise, including improving rates of breastfeeding Increase uptake of the rewind programme to reverse pre-diabetes Better identify people at risk of high blood pressure, and better engage them Increase the uptake of preventative services Continue focus on the wider determinants and inequalities Develop consistency of scope and quality of services across NWL Focus resource and differentiate services for groups with poor outcomes, e.g. black women and childbirth Build confidence in communities to come forward for care and support Reduce barriers to care for black and other ethnic minority groups; Provide bespoke programmes for most marginalised groups (i.e., SEND and employment) Expand preventative services, in particular tackling obesity and improve healthy weight in early childhood; increase breastfeeding rates; improve immunisation rates; improve oral health Expand access to mental health support through schools, children s health hubs and digital tools Develop consistent, right person first time core models of care through child health and family hubs 6
7 We have set out our strategy and priorities for the next five years (2/2) Provide care closer to home Improve access Improve productivity & quality of care Reduce hospital and care home admissions through improved local care; Utilise voluntary providers to support residents after discharge; Put in place a care plan for people with an ongoing health or care need Develop/ roll out integrated neighbourhood teams to bring community MH, primary community, and social care together locally Rationalise channels for simple urgent care and streamline access Implement local integrated response to urgent demand Establish and expand a live Directory of Services Expand use and capacity of virtual wards Institute more efficient planned surgical centres Redesign access to specialist expertise and diagnosis Increase mental health capacity including for people with autism, dementia and learning disabilities Expand digital technologies Detailed review of emergency care pathways Implement innovative, cost-effective models of care in cardiovascular, cancer and children s mental health Ensure seamless pathways from general practice to hospitals and back home again Develop workforce transformation plans Use digital tools to identify those residents most at risk of and direct early interventions Use data to understand where resources could be used more effectively, e.g. to predict demand and manage capacity; to evaluate which services deliver benefits to which residents Ensure that estate is fit for purpose and better utilised 7
8 We are developing detailed implementation plans across the 13 core programmes Five enabling programmes: Five core delivery programmes: 6. Rapidly adopt digital technologies across all services 7. Utilise data and analytics to improve access, productivity and quality of care and support research 8. Drive research and adopt innovative approaches to support the ICS objectives 9. Improve quality and utilisation of estate 10. Transform the workforce 1. Improve health and reduce inequalities 2. Improve access to, and quality and efficiency of, local care including primary, social & community care 3. Improve access to, and quality and efficiency of, mental health care services and services supporting learning disabilities and autism 4. Improve urgent and emergency care access 5. Transform planned care to reduce waiting lists Social care?? Three priority clinical/user areas 11. Cancer 12. Children & Young People 13. Maternity 8
9 What does a great programme look like Add programme health clear TOR, specification, align objectives, outcomes, co-production, membership , metrics 9
10 We have established eight Borough/Place Based Partnerships (BBPs) and Provider Collaboratives. BBPs bring together primary care, social care, public health, mental health and community care within a Borough and work closely with the voluntary and acute sector Integrated Care Board supports across the system Hillingdon BBP Hounslow BBP Brent BBP Ealing BBP Harrow BBP Hammersmith & Fulham BBP Kensington & Chelsea BBP Westminster BBP Bi-borough PCN/INTs*x6 PCN/INTsx6 PCN/INTsx6 PCN/INTsx6 PCN/INTsx6 PCN/INTsx6 PCN/INTsx5 PCN/INTsx4 Community and Mental Health Care Collaborative (covers four Trusts) Acute Care Collaborative (covers four Trusts) *Primary Care Networks, transitioning to Integrated Neighbourhood Teams 10
11 ICB governance structure aligned to core functions Health & Well-being Boards x 8 Integrated Care Partnership Joint Oversight (Health & Social Care) Committees ICB Board Strategic Commissioning Committee Remuneration Committee (statutory) Audit & Risk Committee (statutory) ICB Executive Team Performance* Committee ICS Programme Boards Contracting Committee * Performance covers quality of care, productivity, impact on health outcomes and inequalities in health and wider economic and social growth 11
12 What this presentation covers Introduction to NW London and the Integrated Care System (ICS) Proposed operating framework (or how decisions are made) Strategy and planning including financial allocations Delivery of care and interventions Assurance Relative roles of key players Borough/Place Based Partnerships (including public health, primary care, community & mental health , social services , acute care) Provider Collaboratives ICS wide programmes and the ICB 12
13 The operating framework sets out how the ICS will organise around three functions Reducing inequalities and making London the world s healthiest global city Reducing inequalities and making London the world s healthiest global city Strategy Setting overall strategy and agreeing plans Allocating resources Redesigning, innovating and transforming pathways Setting core service specifications & contracting for services Strategic commissioning Delivery Delivering against agreed pathways and specifications through borough based partnerships and provider collaboratives Tailoring specifications to local circumstance and need where necessary Aligning enablers to support delivery Assurance of delivery Delivery Assurance Overseeing the system (in particular the NHS funded parts) Supporting quality, finance, operational performance and workforce 13
14 Inputs in developing strategy Aligned priorities across the system (overseen by Integrated Care Partnership) Shared borough priorities and understanding of resident needs Top-down priorities (national & regional) Analysis of current performance and opportunities Resident & user views Clinical input from CRGs Programme strategies Priorities identified based on local needs and preferences ( bottom up priorities) Support from ICB Programmes or Collaboratives lead Bre Eal Strategy H&F Joint Strategic Needs Assessments Har Finance Place-based planning NWL-wide planning Hil Joint Health and Wellbeing Strategies Communications and engagement Hou Co-ordination and support from NWL-wide programme teams (Local Care, Acute Care, Mental Health) K&C Clinical / professional leadership through CRGs Wm BBPs lead 14
Relative roles in developing strategy and plans Overarching strategy Detailed strategy Planning Leads on developing and approving overarching strategy (pulling together contributions from LAs, ICS programmes, providers, etc.) Develops section of overarching strategy for specific area of focus Receives and comments on more detailed strategies and plans across programmes Reviews progress against plans as part of overall strategic review ICP (Local Authorities & NHS) Further develops section of overarching strategy into strategy for own area (including demand, capacity, resource allocation, etc.) For priority areas in overarching strategy, CRG provides clinical advice/ support into more detailed programme or collaborative strategy Translates overarching strategy and local priorities into more detailed strategy for the borough Translates more detailed strategy into work streams,and project plans (detailed year 1 plan, outline 5 year plan) ICS programmes Provide clinical input to strategy development, setting priorities and providing input to individual programmes Supports development of more detailed plan where relevant CRGs Lead on detailed analysis of population health needs Ensure borough priorities reflected Translates strategy and programme plans into local implementation plans (detailed year 1 plan, outline 5 year plan) BBPs (Local Authority based) Lead on detailed analysis of what is working/not working Provide input on optimal delivery models and areas for innovation Works up more detailed collaborative and individual provider strategy building on overarching strategy and programme strategies Translates collaborative strategy into project plans (detailed year 1 plan, outline 5 year plan) Collaboratives/ providers 15
Example: Developing MH strategy and plans Inputs (lead responsibility) Develop proposals and options (programme team) Test, discuss, consult Set out services/interventions based on clinical evidence base/national guidance Discuss and involve users, residents, staff, wider stakeholders in each stage of developing proposals and plans Population health needs analysis (BBPs) Describe optimal delivery models for priority interventions (inpatient, outpatient, in person, digital, scale considerations) Views of users and residents (ICB comms to coordinate) Amend plans accordingly and/or set out choices Analyse capacity (workforce, space) requirements to deliver against population needs Current care levels of activity and performance (collaboratives) Identify areas needing formal consultation Set out financial implications based on efficient working Current care - SWOT analysis, overview of performance (collaboratives) Set out estate and workforce requirements based on efficient working Emerging best practice, new ideas, new approaches (CRGs) Outline ask for future research and innovation NHSE requirements and recommendations (ICB, collaboratives) Detail plans to go from here to there over next five years Work coordinated by programme team, supported by ICB execs, reporting into ICS wide programme board and ultimately to the ICP 16
17 Where we want to get to re financial allocations Allocations Allocate money to maximise outcomes All system partners to deliver care in most efficient and effective way to improve care & outcomes Providers to deliver core service models in line with population need & focus on continuous improvement to improve outcomes Flex the commissioned service to react to local evidenced population need Analysis - Need - Current spend - Evidence base to demonstrate value add - Efficient cost of delivery - Deliver within our allocation Core principles Money follows need Services based on evidence of value add impact on outcomes Deliver in most efficient way 17
18 Actions in the meantime Deliver our financial targets for 23/24 Improve our underlying deficit so our recurrent exit run rate in 23/24 allows us to live within our financial allocation in 24/25 Continue to establish a clearer understanding of the as is understanding of allocations and outcomes achieved by sector Complete a review of expenditure to understand our contracted expenditure, its funding source and the outcomes / benefits. This will inform the 24/25 financial planning and commissioning cycle. Continuously improve the design of data led change programmes highest priority conditions and align programmes of work to drive improvement in resident outcomes diabetes, heart disease, mental health problems, cancer - to build greater transparency/analysis re need, impact of interventions and optimal cost of delivery Informed by building better links between population and indicative spend by borough and describe impact on outcomes and resources from moving to agreed service models across NW London in the highest priority conditions Work on how we unlock the financial benefits of innovation and technology so that organisations can commit to change Work on our capital allocation to link this to the overall ICS strategy Lobby for additional capital resource or the ability to generate our own to increase the amount of capital available Continue working with Boroughs on their estates need and strategy 18
Delivery of care Borough Based Partnership ICB and ICS wide programmes Provider Collaboratives Develop a Place lens , taking a PHM approach Work in partnership with all local organisations, to undertake robust capacity and financial planning across all organisations to ensure delivery of core NWL specifications Work in partnership with all local organisations, to undertake robust capacity and financial planning within strategic framework Work in partnership with all local organisations, to undertake robust capacity and financial planning within strategic framework Develop effective relationships between partners to better inform and effect service provision Provide a coordinating function where required to ensure all partners are able to work in the most efficient and high quality manner Develop effective relationships between partners to better inform and effect future service provision Deliver the ICP strategy and objectives, ensuring delivery of core NWL specifications Deliver the ICP strategy and objectives, with specific areas delegated to Borough/Place, such as Primary Care. Develop system wide tools to support optimal service delivery Lead transformation of services where largely within the remit of the collaborative Ensure delivery of core NWL specifications at a Place level Build capacity and capability across the ICS either directly or in conjunction with providers; Leverage the collective resources of the collaborative to reduce unwarranted variation in patient outcomes, access, and experience, and building greater resilience for services, for example, by sharing capacity and resources. Implement effective Integrated Neighbourhood Teams that bring together primary care, social care, community, community MH, voluntary sector and relevant acute outreach, organised around natural communities of where people live and work/PCNs. Identify where services aren t being delivered optimally, not sufficiently coordinated and take actions to address Work with Integrated Neighbourhood Teams that bring together primary care, social care, community, community MH, voluntary sector and relevant acute outreach, organised around natural communities of where people live and work/PCNs. Develop effective communication, engagement and partnerships with local residents and communities Support and enable delivery of the local H&WBB Strategy, and to be a member of the HWBB. Develop effective communication, engagement and partnerships with local residents and communities Ensure effective use of one public estate at Place, and to oversee the development of the NHS local Estate plan Ensure effective use of the public estate 19
Assurance ensuring appropriate balance across local governance and ICB governance Need to get to the right data with the right people with appropriate actions First line of defence sits within provider organisations SOMs Regular performance review with data collated by programmes Moving to a single version of the truth (which would reduce need for data collection, allowing greater focus on improvement) Focus on improvement as much as performance management Feedback to strategy Boroughs to input into performance reviews vis SOMs and programmes 20
21 What this presentation covers Introduction to NW London and the Integrated Care System (ICS) Proposed operating framework (or how decisions are made) Strategy and planning including financial allocations Delivery of care and interventions Assurance Relative roles of key players Borough/Place Based Partnerships Provider Collaboratives ICS wide programmes and the ICB 21
22 Roles of Borough Based Partnerships Delivery Delivery of local integrated care including the targets and trajectories that link to the ICS operating plan e.g. access targets, vaccination programmes, referral management, discharges and screening Coordinate the development of integrated neighbourhood teams across organisations to deliver integrated local health and care services consistent with the strategy and blueprints Lead and drive service transformation working with and across collaboratives Ensure all service delivery meets local needs, addressing inequalities, understanding local communities, taking a PHM approach Deliver core national and NW London wide requirements for primary care Strategy and Planning Build detailed analysis of local residents health and care needs through JSNA Work with local residents and communities to understand local priorities and views on services/interventions Agree local priorities with health and well-being boards Work with colleagues across the ICS to develop strategies for different services through programmes Input into wider NWL system strategy Developing local plan within system wide strategy, tailoring services to meet local needs and enhancing core NWL standards where required Oversee the development of the NHS local estate plan. Assurance Continually review quality, productivity and access to care across all service areas Ensure all national, regional and local metrics and regularly monitored Put in place processes for rapid review of quality data, with a first line of defence approach Ensure governance processes enable timely and robust review and challenge of data 22
23 Roles of collaboratives (Acute, Community and MH Trusts) Strategy and Planning Provide input on current care what s working, what s not Identify areas for innovation and change horizon scanning approach Advise on optimal delivery models to support high quality and productive care Set out areas for enablers where change is required Work with clinical reference groups and programmes to develop strategies for individual areas and input into overarching strategy Develop strategy and plans for collaboratives and individual trusts and sites in partnership with rest of system Joint Forward Plan Delivery Delivery of care including the targets and trajectories that link to the ICS operating plan e.g. access targets, discharges Deliver core national and NW London wide requirements Work with partners across the ICS to deliver coordinated and integrated care across care pathways Lead and drive service transformation working with and across collaboratives Innovate and evolve where appropriate Provide mutual support and optimise service delivery across collaborative Ensure all service delivery meets local needs, addressing inequalities, understanding local communities, taking a PHM approach Assurance Continually review quality, productivity and access to care across all service areas Ensure all national, regional and local metrics and regularly monitored Put in place processes for rapid review of quality data, with a first line of defence approach Ensure governance processes enable timely and robust review and challenge of data 23
24 Roles of programmes Build detailed analysis of population needs, drawing on borough-based analysis and assessment Work with residents and users to understand expectations and views on services, drawing on borough, provider and ICB teams Work with Place/Borough Based Partnerships and Provider Collaboratives to understand what currently works well, what could be improved, what best practice looks like Work with clinical reference groups to set out best practice care, understand new approaches and innovations Draw on national expertise, evidence base, national guidance and priorities Work with Place/Borough Based Partnerships, clinical reference groups and provider collaboratives to set shared core standards to ensure equity across NWL; Describe best practice interventions and approaches to deliver optimal outcomes Set, and measure, the appropriate outcomes for each segment of the population; Develop robust demand and capacity models Describe optimal delivery models based on ensuring optimal quality and productivity and set out what this could mean in NWL Develop options for future delivery models and outline criteria to evaluate Set out implications for digital and data, for workforce development, for estate, for research and innovation Agree metrics for reviewing progress Develop plans to deliver over next five years with clear responsibilities and timelines/milestones Use contracts and reimbursement mechanisms that incentivise providers and where necessary, align multiple providers to deliver the right level of care effectively at the right cost to deliver the set outcomes; Account for procurement and contract management 24