Improving Patient Safety and Care Quality Initiative


AIM:
To provide
the highest
quality
mental
health and
community
care in
England by
2020

Build the will

Build
improvement
capability

Alignment

Reduce harm
by 30% every
year

1.
Launch event & roadshows
2.
Microsite
3.
Create compelling narrative
4.
Use of patient and staff stories
5.
Celebrate successes
6.
Network of champions / ambassadors
7.
Learning events

1.
Initial assessment of alignment & capability
2.
Recruiting central QI team
3.
Online training
4.
Face-to-face training
5.
Follow-up coaching on projects
6.
Develop in-house training for 2016 onwards

1.
Align all projects with improvement aims
2.
Align team / service goals with improvement aims
3.
Align all corporate and support systems
4.
Patient and carer involvement in all improvement work
5.
Embed improvement within management structures
1.
Reduce harm from inpatient violence
2.
Reduce harm from falls
3.
Reduce harm from pressure ulcers
4.
Reduce harm from medication errors
5.
Reduce harm from restraints

Right care,
Right place,
Right time

1.
Improving patient and carer experience
2.
Reliable delivery of evidence-based care
3.
Reducing delays and inefficiencies in the system
4.
Improving access to care at the right location



Reducing harm from inpatient violence
AIM
PRIMARY DRIVERS
SECONDARY DRIVERS
CHANGE IDEAS
Reducing falls and harm from falls
Intentional rounding
Equipment safety
checklist
New slippers
Hip protectors
Reducing harm from pressure ulcers
Eliminate new
Grade 3 and 4
pressure ulcers by
31 March 2014
Reduce the
number of Grade
2 pressure ulcers
acquired under our
care by ….% by
31 March 2014
Risk identification
Risk assessment
Reliable
implementation of
SSKIN care bundle
Identification, grading
of pressure ulcers
Education
Understand pressure ulcer risk factors
Analyse local data to assess patients at risk
Assess pressure ulcer risk on admission
Reassess regularly
Communicate risk status
S – Surface
S – Skin inspection
K – Keep moving
I – Incontinence
N - Nutrition
Use national grading tool
Utilise local tissue viability nursing expertise
Initiate and maintain correct and suitable treatment
Staff education – using workbooks, How-To guides, and patient
stories
Patient and family education – information on pressure ulcer risk
and how to minimise whilst in hospital / at home
AIM
PRIMARY DRIVERS
SECONDARY DRIVERS
AIM
PRIMARY DRIVERS
SECONDARY DRIVERS
CHANGE IDEAS
Improving quality of care on an inpatient female
psychiatric ward
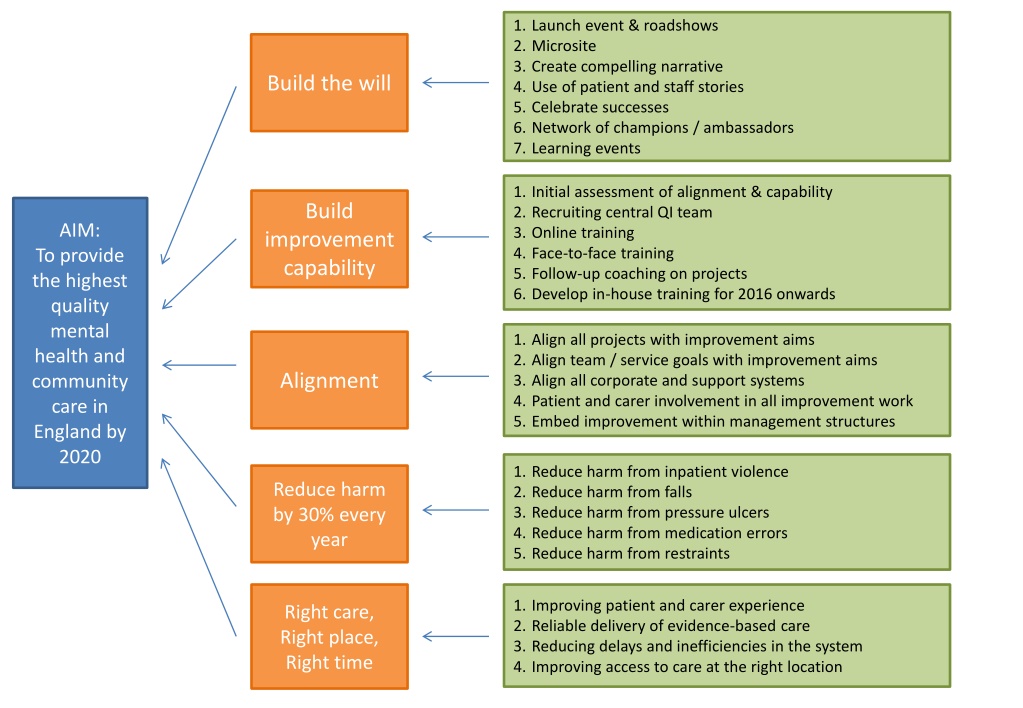
Enhance mental health and community care services in England by 2020 through strategic alignment, capability building, and targeted interventions to reduce harm from inpatient violence, falls, pressure ulcers, medication errors, and restraints. The initiative focuses on patient and staff engagement, training, risk assessment, and prevention strategies to achieve significant harm reduction goals annually while improving patient experience and care delivery efficiency.

Uploaded on Oct 07, 2024 | 0 Views
Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
1. Launch event & roadshows 2. Microsite 3. Create compelling narrative 4. Use of patient and staff stories 5. Celebrate successes 6. Network of champions / ambassadors 7. Learning events Build the will 1. Initial assessment of alignment & capability 2. Recruiting central QI team 3. Online training 4. Face-to-face training 5. Follow-up coaching on projects 6. Develop in-house training for 2016 onwards Build AIM: improvement capability To provide the highest quality mental health and community care in England by 2020 1. Align all projects with improvement aims 2. Align team / service goals with improvement aims 3. Align all corporate and support systems 4. Patient and carer involvement in all improvement work 5. Embed improvement within management structures Alignment 1. Reduce harm from inpatient violence 2. Reduce harm from falls 3. Reduce harm from pressure ulcers 4. Reduce harm from medication errors 5. Reduce harm from restraints Reduce harm by 30% every year 1. Improving patient and carer experience 2. Reliable delivery of evidence-based care 3. Reducing delays and inefficiencies in the system 4. Improving access to care at the right location Right care, Right place, Right time
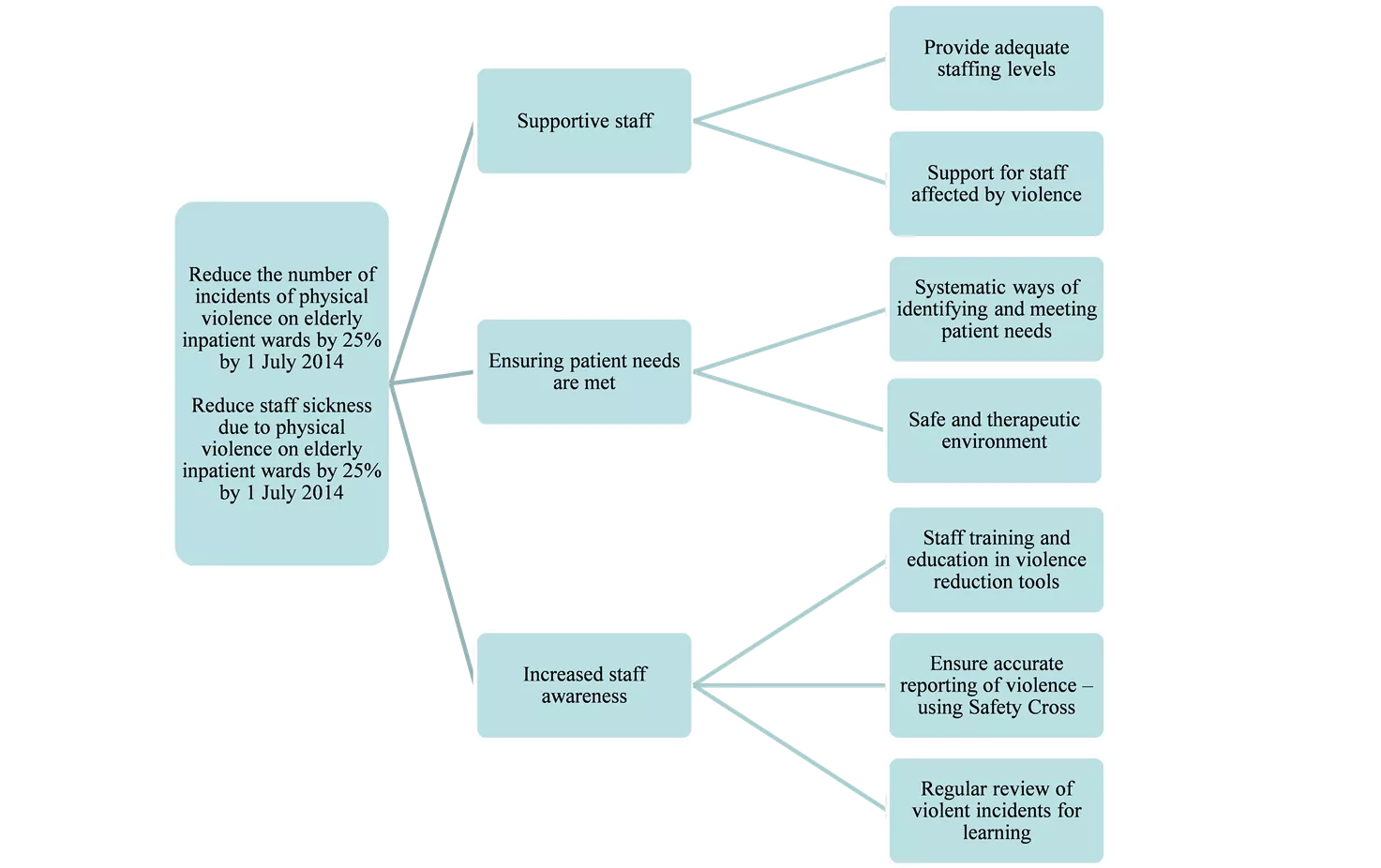
Reducing harm from inpatient violence PRIMARY DRIVERS AIM SECONDARY DRIVERS CHANGE IDEAS Provide adequate staffing levels Supportive staff Support for staff affected by violence Reduce the number of incidents of physical violence on elderly inpatient wards by 25% by 1 July 2014 Systematic ways of identifying and meeting patient needs Ensuring patient needs are met Reduce staff sickness due to physical violence on elderly inpatient wards by 25% by 1 July 2014 Safe and therapeutic environment Staff training and education in violence reduction tools Ensure accurate reporting of violence using Safety Cross Increased staff awareness Regular review of violent incidents for learning
Reducing falls and harm from falls Falls risk assessment on admission Identify those at risk of falling Conduct on-going reassessments Intentional rounding Meet basic needs New slippers Reduce the number of falls on inpatient wards by 20% by August 2014 Reduce harm from falls Hip protectors Asking patient & family re mobility and fall prevention measures at home Interventions to reduce risk Reduce the number of falls with injury on inpatient wards by 20% by August 2014 Use visual / audible cues Medication review Patient education on the positive benefit of interventions Equipment safety checklist Eliminate hazards Safe environment Involve facility management and housekeeping staff
INTERVENTIONS Pressure Ulcer Prevention Key Driver Diagram Leader: _______________ Date: ___/___/___ Utilize a validated standard tool for the skin and risk assessment. Assess skin and risk within four hours of admission. Reassess skin at least once per shift (standardize times) Consider Stage I pressure ulcer as a vital sign to be periodically assessed The risk and skin assessment should be age appropriate. Pediatric versus adult. Be sure to look under medical devices attached to patients Use cameras to photograph and document present-on-admission skin issues. KEY DRIVERS Use topical agents that hydrate the skin & form a moisture barrier to reduce skin damage. Offer toileting often, PO fluids, reassess for wet skin. Involve licensed and unlicensed staff such as nurse aids in every hour rounding for 5 Ps: pain, position, potty, personal belongings and safe pathway Use under-pads that wick moisture away from skin and provide a quick-drying surface. Keep supplies readily available at the bedside in the event the patient is incontinent. Avoid using a thick paste as a cleansing/moisture barrier (staff tend to clean the paste when stool is present resulting in skin injury as the paste is not easily removed). Conduct Skin / Risk Assessment & Reassessment SMART AIM Manage Moisture Reduce the number of hospital acquired pressure ulcers organization- wide by 40% by December 31, 2013. Give patients food/liquid preferences to enhance hydration and nutrition. Provide nutritional supplements if not contraindicated. Create an automatic registered dietician consult if the patient is at high risk. Assess weight, food and fluid intake and laboratory data. Provide at risk patients with a different color water container so all staff and families will know to encourage hydration. Assist the patient with meals and encourage snacks. Offer water to the patient when rounding for 5 Ps: pain, position, potty, personal belongings and safe pathway Optimize Hydration and Nutrition Set specific time frames to reposition using a visual or musical cues, e.g. a turning clock, bells, and alarms, at the nurse s station as a reminder to turn and reposition the patient. Use visual cues at the bed side to turn the patient, e.g. a turning clock or white board that has the time for the next turn. Establish rules for which side patients should be on at certain times (e.g. even hours on right side, odd hours on left side). Ensure pressure-reducing equipment is available at all times. (pillows, beds, heel protectors, foam wedges for positioning, etc.) to redistribute the potential pressure areas. Use device that elevates the heel and prevents external rotation. Use breathable glide sheets that can stay in place / Use lifting devices to prevent shearing or friction / Use ceiling lifts to encourage mobility and movement while preventing work-related injuries Limit linen layers to no more than three (> four has been shown to be a HAPUt risk factor). Minimize Pressure Patient / Staff / Family Awareness of Risk GLOBAL AIM Zero Hospital Acquired Pressure Ulcers every month Identify a staff nurse for each unit as a skin care resource. Conduct nurse-to-nurse shift reports at bedside to include skin assessment with two sets of eyes (to improve accuracy of skin assessment and documentation). Develop documentation tools to prompt daily skin inspections. Visual cues should be available to ensure the completion of the assessment. Use multiple methods to visually identify patients at risk. Use visual cues in the patient s room, door, or front of the medical record, etc.
Reducing harm from pressure ulcers AIM SECONDARY DRIVERS PRIMARY DRIVERS Understand pressure ulcer risk factors Risk identification Analyse local data to assess patients at risk Assess pressure ulcer risk on admission Eliminate new Grade 3 and 4 pressure ulcers by 31 March 2014 Reassess regularly Risk assessment Communicate risk status Reduce the number of Grade 2 pressure ulcers acquired under our care by .% by 31 March 2014 S Surface S Skin inspection K Keep moving I Incontinence N - Nutrition Reliable implementation of SSKIN care bundle Use national grading tool Identification, grading of pressure ulcers Utilise local tissue viability nursing expertise Initiate and maintain correct and suitable treatment Staff education using workbooks, How-To guides, and patient stories Education Patient and family education information on pressure ulcer risk and how to minimise whilst in hospital / at home
Improving quality of care on an inpatient female psychiatric ward PRIMARY DRIVERS AIM SECONDARY DRIVERS CHANGE IDEAS Review of delays at weekly bed meetings Bed occupancy Ward Environment Rewrite protocol Stop sleep outs Ensure daily 1:1 time with named nurse Nursing input To improve the inpatient experience for adult female inpatients on a mental health unit in order to increase satisfaction by 25% in 10 months Offer pharmacy advice to every patient during stay Multidisciplinary Ward Team Process Pharmacy input Train one staff member on each ward to use support skills Family support Change concept of large MDT ward round meetings Ward round Patient Choice Complaints OT programme To change OT programme content Ward Activities Add senior OT to project team