HFpEF Diagnosis and Management









EDUCATIONAL SLIDE MODULE
HFpEF diagnosis
Date of preparation: August 2022
Version 1.0
SC-CRP-12107





T
h
e
a
i
m
s
o
f
t
h
i
s
e
d
u
c
a
t
i
o
n
a
l
s
l
i
d
e
m
o
d
u
l
e
a
r
e
t
o
:
Module objectives
2




HFpEF diagnosis
What is the current reference standard to diagnose HFpEF?
What is the prevalence of HFpEF?
When should heart failure be suspected?
What is the role of score-based algorithms in the diagnosis
of HFpEF?
Summary
Heart failure presents with multiple signs and symptoms, and
varies between patients
4
McMurray JJV
et al. Eur Heart J
2012;33:1787
Breathlessness
C
o
m
m
o
n
s
y
m
p
t
o
m
s
1
C
o
m
m
o
n
s
i
g
n
s
1
Paroxysmal nocturnal dyspnoea
Orthopnoea
Reduced exercise tolerance
Laterally displaced apex beat
Third heart sound (gallop rhythm)
Pulmonary rales
Elevated jugular venous pressure
Fatigue, tiredness, increased time
to recover after exercise
Ankle swelling
Cardiac murmur
Hepatojugular reflux
Many common heart failure signs and symptoms are present
only in patients with advanced HFpEF
5
1. McMurray JJV
et al. Eur Heart J
2012;33:1787; 2. Borlaug B
et al. Circ Heart Fail
2010;3:588
Breathlessness
C
o
m
m
o
n
s
y
m
p
t
o
m
s
1
C
o
m
m
o
n
s
i
g
n
s
1
Paroxysmal nocturnal dyspnoea
Orthopnoea
Reduced exercise tolerance
Laterally displaced apex beat
Third heart sound (gallop rhythm)
Pulmonary rales
Elevated jugular venous pressure
Fatigue, tiredness, increased time
to recover after exercise
Ankle swelling
Cardiac murmur
Hepatojugular reflux
In early HFpEF, often patients
present
only
with exertional
symptoms
2
These
non-specific and widely
prevalent symptoms, especially in
the elderly population, can make it
difficult to differentiate HFpEF from
other disorders
*PARAGON-HF featured patients with advanced HFpEF (LVEF ≥45%, evidence of structural heart disease, and elevated levels of natriuretic peptides)
Jering K
et al
.
JACC Heart Fail
2021;9:386
P
A
R
A
G
O
N
-
H
F
:
P
r
e
v
a
l
e
n
c
e
o
f
H
F
s
i
g
n
s
a
n
d
s
y
m
p
t
o
m
s
a
t
r
a
n
d
o
m
i
s
a
t
i
o
n
*
PARAGON-HF: Patients with HFpEF presented with fewer
symptoms and often experienced exertional dyspnoea or fatigue
6
I
n
P
A
R
A
G
O
N
-
H
F
,
6
2
%
o
f
p
a
t
i
e
n
t
s
w
i
t
h
H
F
p
E
F
*
h
a
d
≤
2
H
F
s
i
g
n
s
a
n
d
s
y
m
p
t
o
m
s
a
t
r
a
n
d
o
m
i
s
a
t
i
o
n
HFpEF diagnosis
What is the current reference standard to diagnose HFpEF?
What is the prevalence of HFpEF?
When should heart failure be suspected?
What is the role of score-based algorithms in the diagnosis
of HFpEF?
Summary
Shah AM
et al. Circulation
2017;135:224
HFpEF is the most common form of HF in older adults
8
P
a
t
i
e
n
t
s
(
%
)
Stage C HF = structural heart disease with
previous or current HF symptoms
P
r
e
s
e
r
v
e
d
L
V
E
F
>
5
0
%
e
v
i
d
e
n
t
i
n
•
9
1
%
o
f
s
t
a
g
e
C
1
H
F
(
p
r
i
o
r
h
o
s
p
i
t
a
l
i
s
a
t
i
o
n
)
•
8
0
%
o
f
s
t
a
g
e
C
2
H
F
(
n
o
p
r
i
o
r
h
o
s
p
i
t
a
l
i
s
a
t
i
o
n
)
HFpEF diagnosis
What is the current reference standard to diagnose HFpEF?
What is the prevalence of HFpEF?
When should heart failure be suspected?
What is the role of score-based algorithms in the diagnosis
of HFpEF?
Summary
*HR: 2.37 (95% CI 1.09, 5.17)
p
=0.029
LV, left ventricular; PCWP, pulmonary capillary wedge pressure; RHC, right-sided heart catheterisation. Pfeffer MA
et al. Circ Res
2019;124:1598
Right heart catheterisation documents elevated LV filling
pressures at rest and/or during exercise
10
F
i
l
l
i
n
g
p
r
e
s
s
u
r
e
s
a
n
d
e
x
e
r
c
i
s
e
F
i
l
l
i
n
g
p
r
e
s
s
u
r
e
s
a
n
d
d
y
s
p
n
o
e
a
F
i
l
l
i
n
g
p
r
e
s
s
u
r
e
s
a
n
d
s
u
r
v
i
v
a
l
∆
D
y
s
p
n
o
e
a
r
a
t
i
n
g
S
u
r
v
i
v
a
l
(
%
)
P
a
t
i
e
n
t
s
w
i
t
h
H
F
p
E
F
h
a
v
e
h
i
g
h
e
r
P
C
W
P
d
u
r
i
n
g
e
x
e
r
c
i
s
e
,
a
n
d
t
h
i
s
i
s
d
i
r
e
c
t
l
y
c
o
r
r
e
l
a
t
e
d
w
i
t
h
i
n
c
r
e
a
s
e
d
d
y
s
p
n
o
e
a
a
n
d
m
o
r
t
a
l
i
t
y
Echo,
echocardiography; LVEDP, left ventricular end-diastolic pressure; PCWP, pulmonary capillary wedge pressure
Pieske B
et al. Eur Heart J
2019;40:3297
The reference standard to diagnose HFpEF is
heart catheterisation
11
I
n
v
a
s
i
v
e
h
a
e
m
o
d
y
n
a
m
i
c
m
e
a
s
u
r
e
m
e
n
t
s
(left and right heart catheterisation)
At rest
During exercise
(invasive stress test)
LVEDP ≥16 mmHg
OR
PCWP ≥15 mmHg
PCWP ≥25 mmHg
Y
e
s
N
o
Perform
echo stress test
OR
invasive stress test
H
F
p
E
F
H
F
p
E
F
HFpEF diagnosis
What is the current reference standard to diagnose HFpEF?
What is the prevalence of HFpEF?
When should heart failure be suspected?
What is the role of score-based algorithms in the diagnosis
of HFpEF?
Summary
H
2
F
P
E
F
s
c
o
r
e
1
•
Uses 6 clinical and
echocardiographic characteristics to
determine probability of HFpEF
•
Enables discrimination of HFpEF
from non-cardiac causes of
dyspnoea and helps determine the
need for further diagnostic testing
HFA-PEFF, Heart Failure Association Pre-test assessment, Echocardiographic & natriuretic peptide score, Functional testing in Case of Uncertainty,
Final Aetiology
1. Reddy YNV
et al. Circulation
2018;138:861; 2.
Pieske B
et al. Eur Heart J
2019;40:3297
Score-based algorithms assign patients with a likelihood
of having HFpEF
13
H
F
A
-
P
E
F
F
d
i
a
g
n
o
s
t
i
c
a
l
g
o
r
i
t
h
m
2
•
Proposes a 4-step diagnostic
approach from initial clinical
assessment to more specialised
tests
•
Can help establish a possible
specific cause of HFpEF or
alternative explanations
S
c
o
r
e
-
b
a
s
e
d
a
l
g
o
r
i
t
h
m
s
a
r
e
b
a
s
e
d
o
n
a
c
o
m
b
i
n
a
t
i
o
n
o
f
c
l
i
n
i
c
a
l
,
l
a
b
o
r
a
t
o
r
y
a
n
d
i
m
a
g
i
n
g
c
h
a
r
a
c
t
e
r
i
s
t
i
c
s
T
h
e
H
2
F
P
E
F
s
c
o
r
e
i
s
a
w
e
i
g
h
t
e
d
s
c
o
r
e
i
n
t
e
g
r
a
t
i
n
g
6
p
r
e
d
i
c
t
i
v
e
v
a
r
i
a
b
l
e
s
t
o
c
r
e
a
t
e
a
c
o
m
p
o
s
i
t
e
s
c
o
r
e
t
h
a
t
e
s
t
i
m
a
t
e
s
t
h
e
p
r
o
b
a
b
i
l
i
t
y
o
f
u
n
d
e
r
l
y
i
n
g
H
F
p
E
F
•
By establishing the probability of
disease, the H
2
FPEF score may be
used to:
–
E
ffectively rule out disease among
patients with low scores (e.g. 0 or 1)
–
E
stablish HFpEF diagnosis with
reasonably high confidence at higher
scores (
e.
g
.
6–9)
–
Identify patients for whom additional
testing is needed with intermediate
scores (e.g
.
2–5)
1. The H
2
FPEF score: An evidence-based approach to
help guide diagnosis of HFpEF
14
E/e’, the
ratio of mitral peak velocity of early filling (E) to early diastolic mitral annular velocity (e’).
Reddy YNV
et al. Circulation
2018;138:861
2. The HFA-PEFF diagnostic algorithm: A consensus
recommendation from the HFA-ESC
15
ECG, electrocardiogram; echo,
echocardiography; ESC, European Society of Cardiology;
HFA-PEFF, Heart Failure Association Pre-test assessment,
Echocardiographic & natriuretic peptide score, Functional testing in Case of Uncertainty, Final Aetiology. Pieske B
et al. Eur Heart J
2019;40:3297
Step F2:
Aetiological
work-up
Step P:
Initial
work-up
Step F1:
Advanced
work-up
Clinical assessment
compatible with HFpEF
Standard diagnostic tests: including
natriuretic peptides, ECG, X-ray, echo
Pretest results
suggestive of HFpEF
Rule out other cardiac/
non-cardiac causes
High
Intermediate
HFA-PEFF score
Not conclusive
Normal
Abnormal
Search for
other cardiac/
non-cardiac
causes
Search for
other cardiac/
non-cardiac
causes
Search for
other cardiac/
non-cardiac
causes
HFpEF confirmed
Normal
Abnormal
Investigate for specific aetiology
Breathless
patient
Low
I
n
v
a
s
i
v
e
d
i
a
s
t
o
l
i
c
s
t
r
e
s
s
t
e
s
t
N
o
n
-
i
n
v
a
s
i
v
e
d
i
a
s
t
o
l
i
c
s
t
r
e
s
s
t
e
s
t
O
R
Step E:
Diagnostic
work-up
AF, atrial fibrillation;
BNP, B-type natriuretic peptide;
E/e’, the
ratio of mitral peak velocity of early filling (E) to early diastolic mitral annular velocity (e’);
GLS, global longitudinal strain;
HFA-
PEFF, Heart Failure Association Pre-test assessment, Echocardiographic & natriuretic peptide score, Functional testing in Case of Uncertainty, Final Aetiology;
LAVI, left atrial volume
index; LV, left ventricular;
LVMI, left ventricular mass index; NT-proBNP, N-terminal pro−B-type natriuretic peptide; PASP, pulmonary artery systolic pressure; RWT, relative wall thickness;
SR, sinus rhythm; TR, tricuspid regurgitation. Pieske B
et al. Eur Heart J
2019;40:3297
The HFA-PEFF score (step E) has functional,
morphological and biomarker domains
16
F
u
n
c
t
i
o
n
a
l
M
o
r
p
h
o
l
o
g
i
c
a
l
B
i
o
m
a
r
k
e
r
(
S
R
)
B
i
o
m
a
r
k
e
r
(
A
F
)
F
u
n
c
t
i
o
n
a
l
echo,
echocardiography; LVEDP, left ventricular end-diastolic pressure; PCWP, pulmonary capillary wedge pressure
Pieske B
et al. Eur Heart J
2019;40:3297
In cases of diagnostic uncertainty (step F), functional
tests should be performed
17
I
n
v
a
s
i
v
e
h
a
e
m
o
d
y
n
a
m
i
c
m
e
a
s
u
r
e
m
e
n
t
s
(left and right heart catheterisation)
At rest
During exercise
(invasive stress test)
LVEDP ≥16 mmHg
OR
PCWP ≥15 mmHg
PCWP ≥25 mmHg
Y
e
s
N
o
Perform
echo stress test
OR
invasive stress test
H
F
p
E
F
H
F
p
E
F
HFA-PEFF, Heart Failure Association Pre-test assessment, Echocardiographic & natriuretic peptide score, Functional testing in Case of Uncertainty,
Final Aetiology; NA, not applicable; ROC,
receiver operating characteristic
Reddy YNV
et al. JAMA Cardiol
2022;doi:10.1001/jamacardio.2022.1916
M
u
l
t
i
c
e
n
t
r
e
m
u
l
t
i
n
a
t
i
o
n
a
l
s
t
u
d
y
a
s
s
e
s
s
i
n
g
t
h
e
d
i
a
g
n
o
s
t
i
c
p
e
r
f
o
r
m
a
n
c
e
o
f
t
h
e
H
2
F
P
E
F
a
n
d
H
F
A
-
P
E
F
F
a
l
g
o
r
i
t
h
m
s
The H
2
FPEF and HFA-PEFF algorithms have been validated for
the diagnosis of HFpEF
18
The study showed that both algorithms detected
patients with HFpEF
However, false negatives were more common with
the HFA-PEFF diagnostic algorithm
This highlights that the diagnostic algorithms must
not be used as a ‘rule out’ test for HFpEF
HFA-PEFF, Heart Failure Association Pre-test assessment, Echocardiographic & natriuretic peptide score, Functional testing in Case of Uncertainty,
Final Aetiology
;
HHF, hospitalization for heart failure. Selvaraj S
et al. J Am Coll Cardiol HF
2020;8:640
H
2
FPEF or HFA-PEFF scores can predict risk in patients
with dyspnoea
19
A
m
o
n
g
p
a
t
i
e
n
t
s
w
i
t
h
u
n
e
x
p
l
a
i
n
e
d
d
y
s
p
n
o
e
a
i
n
t
h
e
c
o
m
m
u
n
i
t
y
,
h
i
g
h
e
r
s
c
o
r
e
s
a
r
e
a
s
s
o
c
i
a
t
e
d
w
i
t
h
h
i
g
h
e
r
r
i
s
k
o
f
H
F
h
o
s
p
i
t
a
l
i
s
a
t
i
o
n
o
r
d
e
a
t
h
H
2
F
P
E
F
s
c
o
r
e
F
o
l
l
o
w
-
u
p
t
i
m
e
(
y
e
a
r
s
)
C
u
m
u
l
a
t
i
v
e
r
i
s
k
o
f
H
H
F
o
r
d
e
a
t
h
H
F
A
-
P
E
F
F
s
c
o
r
e
C
u
m
u
l
a
t
i
v
e
r
i
s
k
o
f
H
H
F
o
r
d
e
a
t
h
F
o
l
l
o
w
-
u
p
t
i
m
e
(
y
e
a
r
s
)
p
<
0
.
0
0
1
p
<
0
.
0
0
1
*Patients with unexplained dyspnoea
py, patient-years
Selvaraj S
et al
.
J Am Coll Cardiol HF
2020;8:640
E
v
e
n
t
r
a
t
e
s
f
o
r
a
d
v
e
r
s
e
C
V
o
u
t
c
o
m
e
s
u
s
i
n
g
H
2
F
P
E
F
s
c
o
r
e
c
a
t
e
g
o
r
i
e
s
20
*Patients with unexplained dyspnoea
HFA-PEFF, Heart Failure Association Pre-test assessment, Echocardiographic & natriuretic peptide score, Functional testing in Case of Uncertainty,
Final Aetiology;
py, patient-years
Selvaraj S
et al. J Am Coll Cardiol HF
2020;8:640
E
v
e
n
t
r
a
t
e
s
f
o
r
a
d
v
e
r
s
e
C
V
o
u
t
c
o
m
e
s
u
s
i
n
g
H
F
A
-
P
E
F
F
s
c
o
r
e
c
a
t
e
g
o
r
i
e
s
21
For the HFA-PEFF score, low risk was defined as a score of 2–4, medium risk as score of 5 and high risk as a score of 6. For the H
2
FPEF probability,
<90% was defined as low risk, 90–95% as medium risk, and 96–100% as high risk.
HFA-PEFF, Heart Failure Association Pre-test assessment,
Echocardiographic & natriuretic peptide score, Functional testing in Case of Uncertainty, Final Aetiology
Verbrugge FH
et al. Eur J Heart Fail
2021:23;954
A
m
o
n
g
h
o
s
p
i
t
a
l
i
s
e
d
p
a
t
i
e
n
t
s
w
i
t
h
d
e
c
o
m
p
e
n
s
a
t
e
d
H
F
p
E
F
,
h
i
g
h
e
r
r
i
s
k
s
c
o
r
e
s
a
r
e
a
s
s
o
c
i
a
t
e
d
w
i
t
h
h
i
g
h
e
r
i
n
c
i
d
e
n
c
e
o
f
H
F
r
e
a
d
m
i
s
s
i
o
n
H
2
FPEF or HFA-PEFF scores can predict the risk of readmission
in hospitalised patients with decompensated HFpEF
22
Borlaug BA.
Nat Rev Cardiol
2020;17:559
Summary: H
2
FPEF and HFA-PEFF scores indicate probability of HFpEF;
intermediate probability should be followed up with invasive exercise testing
23
Haemodynamic exercise test
H
2
F
P
E
F
s
c
o
r
e
H
F
A
-
P
E
F
F
s
c
o
r
e
•
Current or previous hospitalisation
for heart failure
1–3
•
Favourable symptomatic response to
diuretics
4
•
Overt LA enlargement and/or
LV hypertrophy
5
LA, left atrial; LV, left ventricular
1.
Reddy YNV
et al. Circulation
2018;138:861; 2.
Owan TE
et al. N Engl J Med
2006;355:251; 3. Bhatia RS et al. N Engl J Med 2006;355:260;
4. McKee PA
et al. N Engl J Med
1971;285:1441; 5.
Heidenreich PA
et al. J Am Coll Cardiol
2022;79:e263; 6
.
Pieske B
et al. Eur Heart J
2019;40:3297
In some patients, the diagnosis of HFpEF may be clear
24
H
F
p
E
F
d
i
a
g
n
o
s
i
s
m
a
y
b
e
s
t
r
a
i
g
h
t
f
o
r
w
a
r
d
i
f
p
a
t
i
e
n
t
s
h
a
v
e
p
r
e
s
e
r
v
e
d
L
V
E
F
a
n
d
:
W
h
e
n
t
h
e
H
F
p
E
F
d
i
a
g
n
o
s
i
s
i
s
n
o
t
c
l
e
a
r
,
f
u
r
t
h
e
r
a
s
s
e
s
s
m
e
n
t
s
a
r
e
c
r
u
c
i
a
l
,
s
u
c
h
a
s
u
s
i
n
g
s
c
o
r
e
-
b
a
s
e
d
a
l
g
o
r
i
t
h
m
s
1
,
6
N
o
r
m
a
l
h
e
a
r
t
H
F
p
E
F
Enlarged
left atrium
LV
hypertrophy
HFpEF diagnosis
What is the current reference standard to diagnose HFpEF?
What is the prevalence of HFpEF?
When should heart failure be suspected?
What is the role of score-based algorithms in the diagnosis
of HFpEF?
Summary
Summary
26
HFA-PEFF, Heart Failure Association Pre-test assessment, Echocardiographic & natriuretic peptide score, Functional testing in Case of Uncertainty, Final
Aetiology
1. McDonagh TA
et al. Eur Heart J
2021;42:3599; 2. Heidenreich PA
et al. J Am Coll Cardiol
2022;79:e263;
3. Reddy YNV
et al. Circulation
2018;138:861; 4.
Pieske et al. Eur Heart J
2019;40:3297;
5. Selvaraj S
et al. J Am Coll Cardiol HF
2020;8:640; 6.
Sanders-van Wijk S
et al. Eur J Heart Fail
2021;23:838.
Heart failure with preserved ejection fraction (HFpEF) poses diagnostic challenges due to varied symptoms and signs. This educational slide module explores the complexities faced by physicians in diagnosing HFpEF, current reference standards, and the role of score-based algorithms. It highlights the prevalence of HFpEF, common symptoms and signs, and differentiating factors from other disorders. The module aims to enhance understanding and application of guideline recommendations for identifying and managing HFpEF effectively.

Uploaded on Jul 11, 2024 | 10 Views
Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
HFpEF diagnosis EDUCATIONAL SLIDE MODULE Date of preparation: August 2022 Version 1.0 SC-CRP-12107
Module objectives The aims of this educational slide module are to: 1 Highlight the challenges faced by physicians in the lead up to diagnosis of HFpEF 2 Understand the latest guideline/consensus recommendations for the diagnosis of patients with HFpEF 3 Explain the current diagnostic reference standards for HFpEF, including associated challenges Explore recent diagnostic criteria that may facilitate the identification of patients at risk of developing HFpEF 4 2
HFpEF diagnosis When should heart failure be suspected? What is the prevalence of HFpEF? What is the current reference standard to diagnose HFpEF? What is the role of score-based algorithms in the diagnosis of HFpEF? Summary
Heart failure presents with multiple signs and symptoms, and varies between patients Common symptoms1 Common signs1 Breathlessness Elevated jugular venous pressure Paroxysmal nocturnal dyspnoea Hepatojugular reflux Orthopnoea Third heart sound (gallop rhythm) Reduced exercise tolerance Pulmonary rales Fatigue, tiredness, increased time to recover after exercise Laterally displaced apex beat Ankle swelling Cardiac murmur 4 McMurray JJV et al. Eur Heart J 2012;33:1787
Many common heart failure signs and symptoms are present only in patients with advanced HFpEF Common symptoms1 Common signs1 Breathlessness Elevated jugular venous pressure In early HFpEF, often patients present only with exertional symptoms2 Paroxysmal nocturnal dyspnoea Hepatojugular reflux Orthopnoea Third heart sound (gallop rhythm) Thesenon-specific and widely prevalent symptoms, especially in the elderly population, can make it difficult to differentiate HFpEF from Reduced exercise tolerance Pulmonary rales Fatigue, tiredness, increased time to recover after exercise Laterally displaced apex beat other disorders Ankle swelling Cardiac murmur 5 1. McMurray JJV et al. Eur Heart J 2012;33:1787; 2. Borlaug B et al. Circ Heart Fail 2010;3:588
PARAGON-HF: Patients with HFpEF presented with fewer symptoms and often experienced exertional dyspnoea or fatigue PARAGON-HF: Prevalence of HF signs and symptoms at randomisation* 100 90 In PARAGON-HF, 62% of patients with HFpEF* had 2 HF signs and symptoms at randomisation Proportion with signs or 80 70 symptoms (%) 60 50 40 30 20 10 0 Dyspnoea on exertion Fatigue Oedema Orthopnoea Jugular venous distention Rales Paroxysmal nocturnal dyspnoea Dyspnoea Third heart sound *PARAGON-HF featured patients with advanced HFpEF (LVEF 45%, evidence of structural heart disease, and elevated levels of natriuretic peptides) Jering K et al. JACC Heart Fail 2021;9:386 6
HFpEF diagnosis When should heart failure be suspected? What is the prevalence of HFpEF? What is the current reference standard to diagnose HFpEF? What is the role of score-based algorithms in the diagnosis of HFpEF? Summary
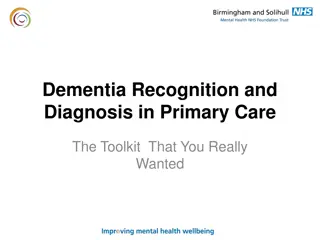
HFpEF is the most common form of HF in older adults Stage 0 Stage A Stage B Stage C1 Stage C2 100% 3 Stage C HF = structural heart disease with previous or current HF symptoms 4 6 6 9 5 7 6 7 90% 10 80% 27 29 31 Preserved LVEF >50%evident in 91% of stage C1 HF (prior hospitalisation) 80% of stage C2 HF (no prior hospitalisation) 30 70% 30 Patients (%) 60% 50% 40% 58 53 52 52 30% 48 20% 10% 7 7 5 5 3 0% Overall study population >80 years 70 75 years 75 80 years 70 years 8 Shah AM et al. Circulation 2017;135:224
HFpEF diagnosis When should heart failure be suspected? What is the prevalence of HFpEF? What is the current reference standard to diagnose HFpEF? What is the role of score-based algorithms in the diagnosis of HFpEF? Summary
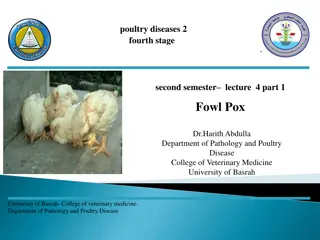
Right heart catheterisation documents elevated LV filling pressures at rest and/or during exercise Filling pressures and exercise Filling pressures and dyspnoea Filling pressures and survival p=0.002 r=0.44 p<0.0001 HFpEF Control 100 40 15 * 90 * 80 30 Dyspnoea rating 70 Survival (%) PCWP (mmHg) 10 60 High PCWP at: Rest 50 20 Exercise 40 + + Series 1 5 30 - + Series 2 10 Series 3 + - 20 Series 4 - - 10 0 0 0 Baseline Leg raise 20W Peak 1 min recovery 0 10 20 30 40 50 0 4 8 12 16 Time (years) PCWP with exercise (mmHg) Patients with HFpEF have higher PCWP during exercise, and this is directly correlated with increased dyspnoea and mortality *HR: 2.37 (95% CI 1.09, 5.17) p=0.029 LV, left ventricular; PCWP, pulmonary capillary wedge pressure; RHC, right-sided heart catheterisation. Pfeffer MA et al. Circ Res 2019;124:1598 10
The reference standard to diagnose HFpEF is heart catheterisation Invasive haemodynamic measurements (left and right heart catheterisation) During exercise (invasive stress test) At rest PCWP 25 mmHg LVEDP 16 mmHg OR PCWP 15 mmHg HFpEF No Yes Perform echo stress test OR invasive stress test HFpEF Echo, echocardiography; LVEDP, left ventricular end-diastolic pressure; PCWP, pulmonary capillary wedge pressure Pieske B et al. Eur Heart J 2019;40:3297 11
HFpEF diagnosis When should heart failure be suspected? What is the prevalence of HFpEF? What is the current reference standard to diagnose HFpEF? What is the role of score-based algorithms in the diagnosis of HFpEF? Summary
Score-based algorithms assign patients with a likelihood of having HFpEF Score-based algorithms are based on a combination of clinical, laboratory and imaging characteristics H2FPEF score1 Uses 6 clinical and echocardiographic characteristics to determine probability of HFpEF Enables discrimination of HFpEF from non-cardiac causes of dyspnoea and helps determine the need for further diagnostic testing HFA-PEFF diagnostic algorithm2 Proposes a 4-step diagnostic approach from initial clinical assessment to more specialised tests Can help establish a possible specific cause of HFpEF or alternative explanations HFA-PEFF, Heart Failure Association Pre-test assessment, Echocardiographic & natriuretic peptide score, Functional testing in Case of Uncertainty, Final Aetiology 1. Reddy YNV et al. Circulation 2018;138:861; 2. Pieske B et al. Eur Heart J 2019;40:3297 13
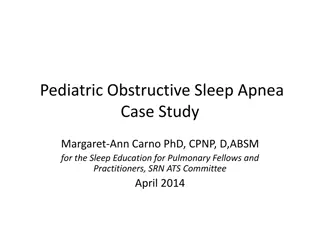
1. The H2FPEF score: An evidence-based approach to help guide diagnosis of HFpEF By establishing the probability of disease, the H2FPEF score may be used to: Effectively rule out disease among patients with low scores (e.g. 0 or 1) Establish HFpEF diagnosis with reasonably high confidence at higher scores (e.g. 6 9) Identify patients for whom additional testing is needed with intermediate scores (e.g. 2 5) The H2FPEF score combines clinical characteristics (top) with associated probability of HFpEF (bottom): Clinical variable Values Points Heavy Body mass index >30 kg/m2 2 H2 Hypertensive 1 2 antihypertensive medicines F Atrial Fibrillation Paroxysmal or persistent 3 Pulmonary hypertension Doppler echocardiogram estimated pulmonary artery systolic pressure >35 mmHg P 1 E F Elder Age >60 years 1 Filling pressure 1 Doppler echocardiographic E/e >9 Sum (0 9) H2FPEF score Total points 4 6 8 0 2 5 7 9 1 3 Probability of HFpEF 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 0.95 The H2FPEF score is a weighted score integrating 6 predictive variables to create a composite score that estimates the probability of underlying HFpEF 14 E/e , the ratio of mitral peak velocity of early filling (E) to early diastolic mitral annular velocity (e ). Reddy YNV et al. Circulation 2018;138:861
2. The HFA-PEFF diagnostic algorithm: A consensus recommendation from the HFA-ESC Breathless patient Clinical assessment compatible with HFpEF Standard diagnostic tests: including natriuretic peptides, ECG, X-ray, echo Pretest results suggestive of HFpEF Step P: Initial work-up Rule out other cardiac/ non-cardiac causes Search for other cardiac/ non-cardiac causes Step E: Diagnostic work-up HFA-PEFF score High Intermediate Low Invasive diastolic stress test Non-invasive diastolic stress test OR Search for other cardiac/ non-cardiac causes Search for other cardiac/ non-cardiac causes Step F1: Advanced work-up Normal Abnormal Not conclusive Abnormal Normal HFpEF confirmed Step F2: Aetiological work-up Investigate for specific aetiology ECG, electrocardiogram; echo, echocardiography; ESC, European Society of Cardiology; HFA-PEFF, Heart Failure Association Pre-test assessment, Echocardiographic & natriuretic peptide score, Functional testing in Case of Uncertainty, Final Aetiology. Pieske B et al. Eur Heart J 2019;40:3297 15
The HFA-PEFF score (step E) has functional, morphological and biomarker domains Functional Functional Morphological Biomarker (SR) Biomarker (AF) NT-proBNP >220 pg/ml OR BNP >80 pg/ml NT-proBNP >660 pg/ml OR BNP >240 pg/ml LAVI >34 ml/m2 OR LVMI 149/122 g/m2 (m/w) and RWT >0.42 Septal e <7 cm/s or lateral e <10 cm/s OR Average E/e 15 OR TR velocity >2.8 m/s (PASP >35 mmHg) Major criteria: 2 points LAVI 29 34 ml/m2 OR LVMI >115/95 g/m2 (m/w) OR RWT >0.42 OR LV wall thickness 12 mm Average E/e 9 14 OR GLS <16% NT-proBNP 125 220 pg/ml OR BNP 35 80 pg/ml NT-proBNP 365 660 pg/ml OR BNP 105 240 pg/ml Minor criteria: 1 point 5 points: HFpEF 2 4 points: perform diastolic stress test or invasive haemodynamic measurements AF, atrial fibrillation; BNP, B-type natriuretic peptide; E/e , the ratio of mitral peak velocity of early filling (E) to early diastolic mitral annular velocity (e ); GLS, global longitudinal strain; HFA- PEFF, Heart Failure Association Pre-test assessment, Echocardiographic & natriuretic peptide score, Functional testing in Case of Uncertainty, Final Aetiology; LAVI, left atrial volume index; LV, left ventricular; LVMI, left ventricular mass index; NT-proBNP, N-terminal pro B-type natriuretic peptide; PASP, pulmonary artery systolic pressure; RWT, relative wall thickness; SR, sinus rhythm; TR, tricuspid regurgitation. Pieske B et al. Eur Heart J 2019;40:3297 16
In cases of diagnostic uncertainty (step F), functional tests should be performed Invasive haemodynamic measurements (left and right heart catheterisation) During exercise (invasive stress test) At rest PCWP 25 mmHg LVEDP 16 mmHg OR PCWP 15 mmHg HFpEF No Yes Perform echo stress test OR invasive stress test HFpEF echo, echocardiography; LVEDP, left ventricular end-diastolic pressure; PCWP, pulmonary capillary wedge pressure Pieske B et al. Eur Heart J 2019;40:3297 17
The H2FPEF and HFA-PEFF algorithms have been validated for the diagnosis of HFpEF Multicentre multinational study assessing the diagnostic performance of the H2FPEF and HFA-PEFF algorithms ROC curve for H2FPEF and HFA-PEFF score Prevalence of HFpEF for each score category The study showed that both algorithms detected patients with HFpEF 100 1.0 H2FPEF score HFA-PEFF score HFpEF (%) 80 0.8 Sensitivity However, false negatives were more common with the HFA-PEFF diagnostic algorithm 0.6 60 40 0.4 H2FPEF score HFA-PEFF score 20 0.2 This highlights that the diagnostic algorithms must not be used as a rule out test for HFpEF P<0.0001 0 0 Low Intermediate High 0 0.2 0.4 0.6 0.8 1.0 1 Specificity Score probability category p-value p-value Overall score OR per unit change (95% CI) AUC (95% CI) AUC comparison H2FPEF (n=627) 2.18 (1.89, 2.52) 0.845 (0.810, 0.875) <0.001 1 [Reference] NA HFA-PEFF (n=594) 1.53 (1.37, 1.72) 0.710 (0.659, 0.756) <0.001 0.134 ( 0.177, 0.094) <0.001 HFA-PEFF, Heart Failure Association Pre-test assessment, Echocardiographic & natriuretic peptide score, Functional testing in Case of Uncertainty, Final Aetiology; NA, not applicable; ROC, receiver operating characteristic Reddy YNV et al. JAMA Cardiol 2022;doi:10.1001/jamacardio.2022.1916 18
H2FPEF or HFA-PEFF scores can predict risk in patients with dyspnoea Among patients with unexplained dyspnoea in the community, higher scores are associated with higher risk of HF hospitalisation or death H2FPEF score HFA-PEFF score 0.40 0.40 Asymptomatic Symptomatic, H2FPEF score 1 2 Symptomatic, H2FPEF score 3 4 Symptomatic, H2FPEF score 5 Known HFpEF Asymptomatic Symptomatic, H2FPEF score 0 2 Symptomatic, H2FPEF score 3 Symptomatic, H2FPEF score 4 Known HFpEF Cumulative risk of HHF or death Cumulative risk of HHF or death 0.30 0.30 p<0.001 p<0.001 0.20 0.20 0.10 0.10 0.00 0.00 2 4 6 0 2 4 6 0 Follow-up time (years) Follow-up time (years) HFA-PEFF, Heart Failure Association Pre-test assessment, Echocardiographic & natriuretic peptide score, Functional testing in Case of Uncertainty, Final Aetiology; HHF, hospitalization for heart failure. Selvaraj S et al. J Am Coll Cardiol HF 2020;8:640 19
Event rates for adverse CV outcomes using H2FPEF score categories Outcome Patient groups N events Events/100 py (95% CI) HR (95% CI) Asymptomatic (n=3749) 416 20.7 (31.6, 45.8) Reference HF hospitalisation or death H2FPEF score 1 2 (n=150)* H2FPEF score3 4 (n=264)* H2FPEF score 5 (n=227)* Known HFpEF (n=502) 21 26.8 (17.4, 41.0) 1.30 (0.84, 2.01) 62 47.1 (36.7, 60.4) 2.31 (1.77, 3.02) 55 48.4 (37.2, 63.1) 2.38 (1.80, 3.16) 172 72.6 (62.6, 84.3) 3.62 (3.03, 4.32) Asymptomatic (n=3749) 119 5.9 (5.0, 7.1) Reference HF hospitalisation H2FPEF score 1 2 (n=150)* H2FPEF score3 4 (n=264)* H2FPEF score 5 (n=227)* Known HFpEF (n=502) 4 5.1 (1.9, 13.6) 0.86 (0.32, 2.34) 25 19.1 (12.9, 28.2) 3.26 (2.12, 5.02) 22 19.6 (12.9, 29.8) 3.37 (2.14, 5.31) 63 32.4 (25.3, 41.5) 5.59 (4.12, 7.59) Asymptomatic (n=3749) 343 16.9 (15.2, 18.8) Reference Death H2FPEF score 1 2 (n=150)* H2FPEF score3 4 (n=264)* H2FPEF score 5 (n=227)* Known HFpEF (n=502) 19 24.1 (15.4, 37.7) 1.43 (0.90, 2.28) 52 38.4 (29.3, 50.4) 2.32 (1.73, 3.11) 39 32.9 (24.0, 45.0) 1.98 (1.42, 2.75) 143 58.0 (49.2, 68.3) 3.55 (2.92, 4.32) 0.25 0.5 1 2 4 8 *Patients with unexplained dyspnoea py, patient-years Selvaraj S et al. J Am Coll Cardiol HF 2020;8:640 20
Event rates for adverse CV outcomes using HFA-PEFF score categories Outcome Patient groups N events Events/100 py (95% CI) HR (95% CI) Asymptomatic (n=3749) 416 20.7 (31.6, 45.8) Reference HF hospitalisation or death HFA-PEFF score 0 2 (n=117)* 19 31.8 (20.3, 49.9) 1.56 (0.98, 2.47) HFA-PEFF score 3 (n=214)* 36 32.4 (23.4, 44.9) 1.58 (1.12, 2.22) HFA-PEFF score 4 6 (n=310)* 83 54.3 (43.8, 67.3) 2.67 (2.11, 3.38) Known HFpEF (n=502) 172 72.6 (62.6, 84.3) 3.62 (3.03, 4.32) Asymptomatic (n=3749) 119 5.9 (5.0, 7.1) Reference HF hospitalisation HFA-PEFF score 0 2 (n=117)* 4 6.8 (2.5, 18.0) 1.16 (0.43, 3.13) HFA-PEFF score 3 (n=214)* 10 9.1 (4.9, 16.9) 1.54 (0.81, 2.94) HFA-PEFF score 4 6 (n=310)* 37 24.3 (17.6, 33.5) 4.17 (2.88, 6.03) Known HFpEF (n=502) 63 32.4 (25.3, 41.5) 5.59 (4.12, 7.59) Asymptomatic (n=3749) 343 16.9 (15.2, 18.8) Reference Death HFA-PEFF score 0 2 (n=117)* 16 26.4 (16.2, 43.1) 1.59 (0.96, 2.62) HFA-PEFF score 3 (n=214)* 29 25.7 (17.8, 36.9) 1.54 (1.05, 2.25) HFA-PEFF score 4 6 (n=310)* 65 40.8 (32.0, 52.1) 2.46 (1.88, 3.20) Known HFpEF (n=502) 143 58.0 (49.2, 68.3) 3.55 (2.92, 4.32) 0.25 0.5 1 2 4 8 *Patients with unexplained dyspnoea HFA-PEFF, Heart Failure Association Pre-test assessment, Echocardiographic & natriuretic peptide score, Functional testing in Case of Uncertainty, Final Aetiology; py, patient-years Selvaraj S et al. J Am Coll Cardiol HF 2020;8:640 21
H2FPEF or HFA-PEFF scores can predict the risk of readmission in hospitalised patients with decompensated HFpEF Among hospitalised patients with decompensated HFpEF, higher risk scores are associated with higher incidence of HF readmission 60 HF readmissions incidence rate per 100 patient-years 55 50 45 40 35 30 = HFA-PEFF score 25 = H2FPEF 20 0 1 2 3 4 Medium 5 6 7 8 9 Low High HFpEF risk For the HFA-PEFF score, low risk was defined as a score of 2 4, medium risk as score of 5 and high risk as a score of 6. For the H2FPEF probability, <90% was defined as low risk, 90 95% as medium risk, and 96 100% as high risk. HFA-PEFF, Heart Failure Association Pre-test assessment, Echocardiographic & natriuretic peptide score, Functional testing in Case of Uncertainty, Final Aetiology Verbrugge FH et al. Eur J Heart Fail 2021:23;954 22
Summary: H2FPEF and HFA-PEFF scores indicate probability of HFpEF; intermediate probability should be followed up with invasive exercise testing Patient with unexplained dyspnoea Assessment of pre-test probability: clinical evaluation plus echocardiography H2FPEF score HFA-PEFF score Score label Clinical variable Characteristics Points Domains Major criteria (2 points) Minor criteria (1 point) H2 Heavy BMI >30 kg/m2 2 Functional Septal e <7 cm/s Lateral e <10 cm/s Average E/e ratio 15 Velocity of the tricuspid regurgitation >2.8 m/s (pulmonary artery systolic pressure >35 mmHg) Average E/e ratio 9 14 Global longitudinal strain <16% Hypertension 1 2 antihypertensive medications F Atrial fibrillation Persistent or paroxysmal 3 P Pulmonary hypertension Pulmonary artery systolic pressure >35 mmHg (measured on Doppler echocardiography) 1 Morphological LAVI >34 ml/m2 LVMI 149/122 g/m2(m/w) and relative wall thickness >0.42 LAVI 29 34 ml/m2 LVMI >115/95 g/m2(m/w) Relative wall thickness >0.42 Left ventricular wall thickness 12 mm E Old age Age >60 years 1 Biomarker (sinus rhythm) NT-proBNP >220 pg/ml BNP >80 pg/ml NT-proBNP 125 220 pg/ml BNP 35 80 pg/ml F Filling pressure 1 E/e ratio >9 (measured on Doppler echocardiography) Biomarker (atrial fibrillation) NT-proBNP >660 pg/ml BNP >240 pg/ml NT-proBNP 365 660 pg/ml BNP 105 240 pg/ml Low probability, unlikely HFpEF (H2FPEF score of 0 1, HFA-PEFF score of 0 1) Intermediate probability High probability, likely HFpEF (H2FPEF score of 6 9, HFA-PEFF score of 5 6) (H2FPEF score of 2 5, HFA-PEFF score of 2 4) Haemodynamic exercise test 23 Borlaug BA. Nat Rev Cardiol 2020;17:559
In some patients, the diagnosis of HFpEF may be clear HFpEF diagnosis may be straightforward if patients have preserved LVEF and: Normal heart HFpEF Enlarged left atrium Current or previous hospitalisation for heart failure1 3 Favourable symptomatic response to diuretics4 Overt LA enlargement and/or LV hypertrophy5 LV hypertrophy When the HFpEF diagnosis is not clear, further assessments are crucial, such as using score-based algorithms1,6 LA, left atrial; LV, left ventricular 1. Reddy YNV et al. Circulation 2018;138:861; 2. Owan TE et al. N Engl J Med 2006;355:251; 3. Bhatia RS et al. N Engl J Med 2006;355:260; 4. McKee PA et al. N Engl J Med 1971;285:1441; 5. Heidenreich PA et al. J Am Coll Cardiol 2022;79:e263; 6. Pieske B et al. Eur Heart J 2019;40:3297 24
HFpEF diagnosis When should heart failure be suspected? What is the prevalence of HFpEF? What is the current reference standard to diagnose HFpEF? What is the role of score-based algorithms in the diagnosis of HFpEF? Summary
Summary HFpEF diagnosis remains a challenge due to non-specific signs and symptoms1,2 The H2FPEF and HFA-PEFF algorithms can aid diagnosis in patients with unexplained dypnoea3,4 HFpEF should be suspected in patients with high scores In patients with intermediate scores, additional tests are required4 6 In both algorithms, higher scores are associated with increased risk of HF hospitalisation or death5 HFA-PEFF, Heart Failure Association Pre-test assessment, Echocardiographic & natriuretic peptide score, Functional testing in Case of Uncertainty, Final Aetiology 1. McDonagh TA et al. Eur Heart J 2021;42:3599; 2. Heidenreich PA et al. J Am Coll Cardiol 2022;79:e263; 3. Reddy YNV et al. Circulation 2018;138:861; 4. Pieske et al. Eur Heart J 2019;40:3297; 5. Selvaraj S et al. J Am Coll Cardiol HF 2020;8:640; 6. Sanders-van Wijk S et al. Eur J Heart Fail 2021;23:838. 26















 has functional,")
, functional")