Herpesviruses and Hepatitis Viruses

H
H
e
e
r
r
p
p
e
e
s
s
v
v
i
i
r
r
u
u
s
s
e
e
s
s
&
&
H
H
e
e
p
p
a
a
t
t
i
i
t
t
i
i
s
s
v
v
i
i
r
r
u
u
s
s
e
e
s
s
P
r
o
f
.
D
r
.
D
a
l
y
a
B
a
s
i
l

I
n
t
r
o
d
u
c
t
i
o
n
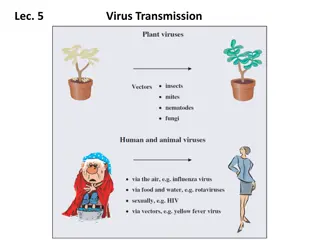
The herpesvirus family contains several of the most
important human viral pathogens.
Clinically, the herpesviruses exhibit a spectrum of
diseases.
Some have a wide host-cell range, whereas others
have a narrow host-cell range.
Ability to establish lifelong persistent infections in
their hosts and to undergo periodic reactivation.
Their frequent reactivation in immunosuppressed
patients causes serious health complications.
C
l
a
s
s
i
f
i
c
a
t
i
o
n
H
e
r
p
e
s
v
i
r
u
s
D
i
s
e
a
s
e
s
HSV-1 and HSV-2
infect epithelial cells and establish latent
infections in neurons. Type 1 is classically associated with
oropharyngeal lesions and causes recurrent attacks of "fever
blisters." Type 2 primarily infects the genital mucosa and is
mainly responsible for genital herpes. Both viruses also cause
neurologic disease. HSV-1 is the leading cause of sporadic
encephalitis in the United States. Both type 1 and type 2 can
cause neonatal infections which are often severe
.
H
e
r
p
e
s
v
i
r
u
s
D
i
s
e
a
s
e
s
Varicella-zoster virus
causes chickenpox (varicella) on primary
infection and establishes latent infection in neurons. Upon
reactivation, the virus causes zoster (shingles). Adults who are
infected for the first time with varicella-zoster virus are appearing to
develop serious viral pneumonia
.
Chickenpox
is a mild, highly contagious disease, chiefly of children,
characterized clinically by a generalized vesicular eruption of the skin
and mucous membranes. The disease may be severe in adults and in
immunocompromised children
.
V
a
r
i
c
e
l
l
a
-
Z
o
s
t
e
r
V
i
r
u
s
H
e
r
p
e
s
v
i
r
u
s
D
i
s
e
a
s
e
s
•
Cytomegalovirus
replicates in epithelial cells of the respiratory
tract, salivary glands, and kidneys and persists in lymphocytes.
It causes mononucleosis. In newborns, cytomegalic inclusion
disease may occur. It is an important cause of congenital
defects and mental retardation
.
•
Human herpesvirus 6
infects T lymphocytes. It is typically
acquired in early infancy and causes exanthem subitum
(roseola infantum).
•
Human herpesvirus 7
, also a T-lymphotropic virus, has not yet
been linked to any specific disease
.
•
EBV
replicates in epithelial cells of the oropharynx and parotid
gland and establishes latent infections in lymphocytes. It
causes infectious mononucleosis and is the cause of human
lymphoproliferative disorders, especially in
immunocompromised patients.
H
e
r
p
e
s
v
i
r
u
s
D
i
s
e
a
s
e
s
Human herpesvirus 8
appears to be associated with the
development of Kaposi sarcoma, a vascular tumor that is
common in patients with AIDS
.
Herpesviruses have been linked with malignant diseases in
humans and lower animals: EBV with Burkitt lymphoma of African
children, with nasopharyngeal carcinoma, and with other
lymphomas; KSHV with Kaposi sarcoma.
C
y
t
o
m
e
g
a
l
o
v
i
r
u
s
•
Cytomegaloviruses are the agents of the most common
congenital infection
.
•
Cytomegalic inclusion disease is a generalized infection of
infants caused by intrauterine or early postnatal infection with
the cytomegaloviruses.
•
The name for the classic cytomegalic inclusion disease derives
from the massive enlargement of cytomegalovirus-infected
cells. Cytomegalovirus poses an important public health
problem because of its high frequency of congenital infections,
which may lead to severe congenital anomalies.
•
In-apparent infection is common during childhood and
adolescence. Severe cytomegalovirus infections are frequently
found in adults who are immunosuppressed.
P
a
t
h
o
g
e
n
e
s
i
s
&
P
a
t
h
o
l
o
g
y
Cytomegalovirus may be
transmitted
person-to-person in
several different ways, all requiring close contact with virus-
bearing material.
There is a 4- to 8-week
incubation period
in normal children
and adults after viral exposure.
The virus causes a
systemic infection
; it has been isolated
from lung, liver, esophagus, colon, kidneys, monocytes, and T
and B lymphocytes.
Like all herpesviruses, cytomegalovirus establishes
lifelong
latent
infections. Virus can be shed intermittently from the
pharynx and in the urine for months to years after primary
infection.
C
o
n
g
e
n
i
t
a
l
&
P
e
r
i
n
a
t
a
l
I
n
f
e
c
t
i
o
n
s
T
r
e
a
t
m
e
n
t
&
C
o
n
t
r
o
l
•
Drug treatments of cytomegalovirus infections have shown
some encouraging results. Ganciclovir, a nucleoside
structurally related to acyclovir, has been used successfully
to treat life-threatening cytomegalovirus infections in
immunosuppressed patients
.
•
Both live and recombinant cytomegalovirus vaccines are
under development.
E
p
s
t
e
i
n
-
B
a
r
r
V
i
r
u
s
•
E
B
V
i
s
t
h
e
c
a
u
s
a
t
i
v
e
a
g
e
n
t
o
f
a
c
u
t
e
i
n
f
e
c
t
i
o
u
s
m
o
n
o
n
u
c
l
e
o
s
i
s
•
E
B
V
i
s
a
s
s
o
c
i
a
t
e
d
w
i
t
h
n
a
s
o
p
h
a
r
y
n
g
e
a
l
c
a
r
c
i
n
o
m
a
•
B
u
r
k
i
t
t
l
y
m
p
h
o
m
a
•
H
o
d
g
k
i
n
a
n
d
n
o
n
-
H
o
d
g
k
i
n
l
y
m
p
h
o
m
a
s
•
o
t
h
e
r
l
y
m
p
h
o
p
r
o
l
i
f
e
r
a
t
i
v
e
d
i
s
o
r
d
e
r
s
i
n
i
m
m
u
n
o
d
e
f
i
c
i
e
n
t
i
n
d
i
v
i
d
u
a
l
s
a
n
d
g
a
s
t
r
i
c
c
a
r
c
i
n
o
m
a
.
B
i
o
l
o
g
y
o
f
E
p
s
t
e
i
n
-
B
a
r
r
V
i
r
u
s
The major target cell for EBV is the B lymphocyte.
When human B lymphocytes are infected with
EBV, continuous cell lines can be established,
indicating that cells have been immortalized by
the virus.
EBV-immortalized B lymphocytes express
differentiated functions, such as secretion of
immunoglobulin.
P
a
t
h
o
g
e
n
e
s
i
s
&
P
a
t
h
o
l
o
g
y
Primary Infection
EBV is commonly transmitted by infected saliva and
initiates infection in the oropharynx. Viral replication
occurs in epithelial cells (or surface B lymphocytes) of the
pharynx and salivary glands. Many people shed low levels
of virus for weeks to months after infection. Infected B
cells spread the infection from the oropharynx throughout
the body. In normal individuals, most virus-infected cells
are eliminated, but small numbers of latently infected
lymphocytes persist for the lifetime of the host
.
P
a
t
h
o
g
e
n
e
s
i
s
&
P
a
t
h
o
l
o
g
y
•
Reactivation from Latency
Reactivations of EBV latent infections can occur, as
evidenced by increased levels of virus in saliva and of DNA
in blood cells. These are usually clinically silent.
Immunosuppression is known to reactivate infection,
sometimes with serious consequences.
C
l
i
n
i
c
a
l
F
i
n
d
i
n
g
s
•
Infectious Mononucleosis
The typical illness is self-limited and lasts 2-4
weeks. During the disease, there is an increase in
the number of circulating white blood cells, with a
predominance of lymphocytes. Many of these are
large, atypical T lymphocytes. Low-grade fever and
malaise may persist for weeks to months after acute
illness.
C
l
i
n
i
c
a
l
F
i
n
d
i
n
g
s
:
C
a
n
c
e
r
Sera from patients with Burkitt lymphoma or
nasopharyngeal carcinoma contain elevated levels of
antibody to virus-specific antigens, and the tumor
tissues contain EBV DNA and express a limited number
of viral genes.
Burkitt lymphoma is a tumor of the jaw in African
children and young adults. Most African tumors
(>90%) contain EBV DNA and express EBNA1 antigen
(latent phase antigen). In other parts of the world, only
about 20% of Burkitt lymphomas contain EBV DNA. It
is speculated that EBV may be involved at an early
stage in Burkitt lymphoma by immortalizing B cells.
E
p
s
t
e
i
n
-
B
a
r
r
V
i
r
u
s
Viral Hepatitis
•
Viral Hepatitis:
is a liver inflammation caused by five unrelated hepatotropic
viruses
Hepatitis A
,
Hepatitis B
,
Hepatitis C
,
Hepatitis D
, and
Hepatitis E
.
•
Other viruses can also cause liver inflammation include
Herpes simplex
,
Cytomegalovirus
,
Epstein–Barr virus
.
•
It may present in acute (recent infection, relatively rapid onset) or chronic
forms.
- Hepatitis viruses
•
Hepatitis A (HAV) Picornaviridae (1973)
•
Hepatitis B (HBV) Hepadnaviridae (1970)
•
Hepatitis C (HCV) Flaviviridae (1988)
•
Hepatitis D (HDV) (1977)
•
Hepatitis E (HEV) (Caliciviridae) (1983)
•
Hepatitis F – Not separate entity – Mutant of B Virus.
•
Hepatitis G (HGV) Flaviviridae (1995
)
Types of Hepatitis
Hepatitis A Virus
•
Small, ssRNA, non-enveloped
(Naked RNA virus) icosahedral
particle, 27 nm in diameter.
•
Related to enteroviruses, formerly
known as enterovirus 72, now put
in its own family.
•
One stable serotype only.
•
HAV is not cytolytic and is
released by exocytosis.
P
a
t
h
o
g
e
n
e
s
i
s
&
S
y
m
p
t
o
m
s
o
f
H
e
p
a
t
i
t
i
s
A
V
i
r
u
s
HAV invade into human body by fecal-oral route, multiplies in the
intestinal epithelium and reaches the liver by hematogenous spread.
After one week, the HAV reach liver cells when replication will occur.
Then enter intestine with bile and appear in feces.
Incubation Period : 2 to 6 weeks.
The clinical symptoms are include:
•
Jaundice (yellow eyes and skin, dark urine)
•
Abdominal pain
•
Loss of appetite
•
Nausea
•
Fever
•
Diarrhea
•
Fatigue
•
Children often have the disease with few symptoms.
H
e
p
a
t
i
t
i
s
A
V
i
r
u
s
r
e
s
i
s
t
a
n
c
e
•
Stable to: acid at pH 3
•
Solvents (ether, chloroform)
•
detergents
•
saltwater, groundwater(months)
•
drying(stable)
•
Temperature
-
4
℃
: stable for weeks
-
56
℃
for 30 minutes: stable
-
61
℃
for 20 minutes: partial inactivation
25
L
a
b
o
r
a
t
o
r
y
D
i
a
g
n
o
s
i
s
1.
Demonstration of Virus in feces:
By: Immunoelectron microscopy
2.
Virus Isolation: by tissue culture.
3.
Detection of Antibody :By ELISA
4.
Biochemical tests:
i) Alanine aminotransferase (ALT)
ii) Bilirubin
5.
Molecular Diagnosis : Real-Time PCR of feces
H
e
p
a
t
i
t
i
s
A
V
i
r
u
s
v
a
c
c
i
n
e
•
Hepatitis A vaccine in infants is safe and
immunogenic without maternal antibody.
•
Combined hepatitis A and hepatitis B vaccine
approved by FDA in United states for persons above
18 years old.
•
The schedule of this vaccine is: 0,1,6 months.
H
e
p
a
t
i
t
i
s
B
V
i
r
u
s
•
Double stranded DNA enveloped virus.
•
Complete particle 42 nm, the core of the virus containing HBcAg
and HBeAg, and the coat contain HBsAg and at least 4
phenotypes of HBsAg are recognized.
•
The HBcAg is of a single serotype.
•
Hepatitis B virus (HBV) has been classified into 8 genotypes (A-
H).
•
Available data suggests that genotype produces a milder disease,
respond better to IFN therapy, and is less likely to develop
hepatocellular carcinoma.
H
B
V
:
S
t
r
u
c
t
u
r
e
•
Virion also referred to as Dane particle (ds-tranded DNA)
•
42nm enveloped virus
•
Core antigens located in the center (nucleocapsid)
•
Core antigen (HBcAg)
•
e antigen (HBeAg)- an indicator of transmissibility (minor
component of the core- antigenically distinct from HBcAg)
•
22nm spheres and filaments other forms- no DNA in these
forms so they are not infectious (composed of surface
antigen)- these forms outnumber the actual virions
HBV
: Structure
F
o
u
r
s
t
a
g
e
s
i
n
t
h
e
v
i
r
a
l
l
i
f
e
c
y
c
l
e
(
H
B
V
)
•
The first stage is immune tolerance. The duration of this stage
for healthy adults is approximately 2-4 weeks and represents
the incubation period.
•
In the second stage, an inflammatory reaction with a cytopathic
effect occurs. HBeAg can be identified in the sera. The duration
of this stage for patients with acute infection is approximately 3-
4 weeks (symptomatic period).
•
In the third stage, the host can target the infected hepatocytes
and the HBV Viral replication no longer occurs. HBeAb can be
detected.
•
In the fourth stage, the virus cannot be detected and antibodies
to various viral antigens have been produced.
C
l
i
n
i
c
a
l
s
y
m
p
t
o
m
s
o
f
h
e
p
a
t
i
t
i
s
b
v
i
r
u
s
Signs and symptoms of hepatitis B, ranging from mild to
severe, usually appear about one to four months after
you've been infected. Signs and symptoms of hepatitis B may
include:
•
Abdominal pain
•
Dark urine
•
Fever
•
Joint pain
•
Loss of appetite
•
Nausea and vomiting
•
Weakness and fatigue
•
jaundice
C
l
i
n
i
c
a
l
o
u
t
c
o
m
e
s
o
f
H
e
p
a
t
i
t
i
s
B
i
n
f
e
c
t
i
o
n
s
L
a
b
o
r
a
t
o
r
y
D
I
A
G
N
O
S
I
S
•
Acute HBV infection is characterized by the presence of HBsAg and
immunoglobulin M (IgM) antibody to HBcAg detected by EIA
(Enzyme Immunoassay).
•
During the initial phase of infection, patients are seropositive for
HBeAg, which is a marker of high levels of replication of the virus.
The presence of HBeAg indicates that the blood and body fluids of
the infected individual are highly contagious.
•
Chronic infection is characterized by the persistence of HBsAg for at
least 6 months (with or without concurrent HBeAg).
•
Persistence of HBeAb is the principal marker of risk for developing
chronic liver disease and liver cancer (hepatocellular carcinoma) later
in life.
T
r
e
a
t
m
e
n
t
•
There is no specific treatment for acute hepatitis B. Therefore, care is
aimed at maintaining comfort and adequate nutritional balance,
including replacement of fluids lost from vomiting and diarrhea. Chronic
hepatitis B infection can be treated with drugs, including oral antiviral
agents, such as tenofovir or entecavir.
•
With nucleoside and nucleotide analogs, such as lamivudine, HBV DNA
levels are reduced, but the virus is rarely eliminated and viral replication
resumes in the majority of patients when treatment is stopped. The
emergence of drug-resistant virus mutants in long-term therapy is a
major problem.
•
Interferon - for HBeAg +ve carriers with chronic active hepatitis.
Response rate is 30 to 40%.
•
Treatment can slow the progression of cirrhosis, reduce incidence of
liver cancer and improve long term survival.
H
e
p
a
t
i
t
i
s
B
V
a
c
c
i
n
e
•
Infants: several options that depend on status of the
mother
•
If mother HBsAg negative: birth, 1-2m,6-18m.
•
If mother HBsAg positive: vaccine and Hep B immune
globulin within 12 hours of birth, 1-2m, <6m.
•
Adults: 0,1, 6 months.
•
Vaccine recommended in All those aged 0-18, and
those at
high risk.
H
e
p
a
t
i
t
i
s
C
V
i
r
u
s
(
H
C
V
)
•
Positive stranded RNA genome of around 10,000 bases
•
Enveloped virus, virion, 30-60nm in diameter
•
Morphological structure remains unknown
•
HCV has been classified into a total of six genotypes (type 1 to 6) on the
basis of phylogenetic analysis
•
Genotype 1 and 4 has a poorer prognosis and response to interferon
therapy.
•
HCV can cause acute infections but is more likely to establish chronic
infections.
•
All the manifestations of chronic hepatitis B infection may be seen, but
with a lower frequency i.e. chronic persistent hepatitis, chronic active
hepatitis, cirrhosis, and hepatocellular carcinoma.
N
a
t
u
r
a
l
h
i
s
t
o
r
y
o
f
H
C
V
L
a
b
o
r
a
t
o
r
y
D
i
a
g
n
o
s
i
s
•
HCV antibody
- generally used to diagnose hepatitis C
infection. Not useful in the acute phase as it takes at least 4
weeks after infection before antibody appears.
•
HCV-RNA
- various techniques are available e.g. PCR. May be
used to diagnose HCV infection in the acute phase. However,
its main use is in monitoring the response to antiviral
therapy.
•
HCV-antigen
- an EIA for HCV antigen is available. It is used
in the same capacity as HCV-RNA tests but is much easier to
carry out.
T
r
e
a
t
m
e
n
t
&
p
r
e
v
e
n
t
i
o
n
Treatment:
•
Interferon - may be considered for patients with chronic active
hepatitis. The response rate is around 50% but 50% of
responders will relapse upon withdrawal of treatment.
•
Ribavirin - there is less experience with ribavirin than
interferon. However, recent studies suggest that a combination
of interferon and ribavirin is more effective than interferon
alone.
Prevention:
•
Screening of blood, organ, and tissue.
•
High risk behavior modification.
•
Blood and body fluid precautions.
H
e
p
a
t
i
t
i
s
D
V
i
r
u
s
•
The delta agent is a defective virus.
•
The agent consists of a particle 35 nm in diameter consisting of
the delta antigen surrounded by an outer coat of HBsAg.
•
The genome of the virus is very small and consists of a single-
stranded RNA.
Hepatitis D - Clinical Features:
•
Co-infection
•
Severe acute disease.
•
Low risk of chronic infection.
Hepatitis D – Prevention
Pre or postexposure prophylaxis to prevent HBV infection
reduces the HBV-HDV Coinfection. And education to reduce risk
behaviors among persons with chronic HBV infection.
H
e
p
a
t
i
t
i
s
E
V
i
r
u
s
•
Calicivirus-like viruses
•
unenveloped RNA virus, 32-34 nm in diameter
•
+ve stranded RNA genome, 7.6 kb in size.
•
very labile and sensitive
Prevention of HEV
•
Avoid drinking water and beverages of unknown purity, uncooked
shellfish, and unwashed fruit/vegetables.
•
IG prepared from donors in Western countries does not prevent
infection.
•
Unknown efficacy of IG prepared from donors in endemic areas.
T
h
a
n
k
Y
o
u
The herpesvirus family includes important human viral pathogens, exhibiting a spectrum of diseases and the ability to establish lifelong infections. Herpes simplex viruses (HSV-1 and HSV-2), varicella-zoster virus, cytomegalovirus, and Epstein-Barr virus are discussed in detail, highlighting their clinical manifestations and impact on human health.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Herpesviruses Herpesviruses & & Hepatitis viruses Hepatitis viruses Prof. Dr. Dalya Basil Prof. Dr. Dalya Basil
Introduction Introduction The herpesvirus family contains several of the most important human viral pathogens. Clinically, the herpesviruses exhibit a spectrum of diseases. Some have a wide host-cell range, whereas others have a narrow host-cell range. Ability to establish lifelong persistent infections in their hosts and to undergo periodic reactivation. Their frequent reactivation in immunosuppressed patients causes serious health complications.
Classification Classification
Herpesvirus Herpesvirus Diseases Diseases HSV-1 and HSV-2 infect epithelial cells and establish latent infections in neurons. Type 1 is classically associated with oropharyngeal lesions and causes recurrent attacks of "fever blisters." Type 2 primarily infects the genital mucosa and is mainly responsible for genital herpes. Both viruses also cause neurologic disease. HSV-1 is the leading cause of sporadic encephalitis in the United States. Both type 1 and type 2 can cause neonatal infections which are often severe.
Herpesvirus Herpesvirus Diseases Diseases Varicella-zoster virus causes chickenpox (varicella) on primary infection and establishes latent infection in neurons. Upon reactivation, the virus causes zoster (shingles). Adults who are infected for the first time with varicella-zoster virus are appearing to develop serious viral pneumonia. Chickenpox is a mild, highly contagious disease, chiefly of children, characterized clinically by a generalized vesicular eruption of the skin and mucous membranes. The disease may be severe in adults and in immunocompromised children.
Herpesvirus Herpesvirus Diseases Diseases Cytomegalovirus replicates in epithelial cells of the respiratory tract, salivary glands, and kidneys and persists in lymphocytes. It causes mononucleosis. In newborns, cytomegalic inclusion disease may occur. It is an important cause of congenital defects and mental retardation. Human herpesvirus 6 infects T lymphocytes. It is typically acquired in early infancy and causes exanthem subitum (roseola infantum). Human herpesvirus 7, also a T-lymphotropic virus, has not yet been linked to any specific disease. EBV replicates in epithelial cells of the oropharynx and parotid gland and establishes latent infections in lymphocytes. It causes infectious mononucleosis and is the cause of human lymphoproliferative disorders, immunocompromised patients. especially in
Herpesvirus Herpesvirus Diseases Diseases Human herpesvirus 8 appears to be associated with the development of Kaposi sarcoma, a vascular tumor that is common in patients with AIDS. Herpesviruses have been linked with malignant diseases in humans and lower animals: EBV with Burkitt lymphoma of African children, with nasopharyngeal carcinoma, and with other lymphomas; KSHV with Kaposi sarcoma.
Cytomegalovirus Cytomegalovirus Cytomegaloviruses are the agents of the most common congenital infection . Cytomegalic inclusion disease is a generalized infection of infants caused by intrauterine or early postnatal infection with the cytomegaloviruses. The name for the classic cytomegalic inclusion disease derives from the massive enlargement of cytomegalovirus-infected cells. Cytomegalovirus poses an important public health problem because of its high frequency of congenital infections, which may lead to severe congenital anomalies. In-apparent infection is common during childhood and adolescence. Severe cytomegalovirus infections are frequently found in adults who are immunosuppressed.
Pathogenesis & Pathology Pathogenesis & Pathology Cytomegalovirus may be transmitted person-to-person in several different ways, all requiring close contact with virus- bearing material. There is a 4- to 8-week incubation period in normal children and adults after viral exposure. The virus causes a systemic infection; it has been isolated from lung, liver, esophagus, colon, kidneys, monocytes, and T and B lymphocytes. Like all herpesviruses, cytomegalovirus establishes lifelong latent infections. Virus can be shed intermittently from the pharynx and in the urine for months to years after primary infection.
Congenital & Perinatal Infections Congenital & Perinatal Infections
Treatment & Control Treatment & Control Drug treatments of cytomegalovirus infections have shown some encouraging results. Ganciclovir, a nucleoside structurally related to acyclovir, has been used successfully to treat life-threatening cytomegalovirus infections in immunosuppressed patients . Both live and recombinant cytomegalovirus vaccines are under development.
Epstein Epstein- -Barr Virus Barr Virus EBV EBV is is the mononucleosis mononucleosis EBV EBV is is associated Burkitt Burkitt lymphoma Hodgkin Hodgkin and other other immunodeficient immunodeficient carcinoma carcinoma. the causative causative agent agent of of acute acute infectious infectious associated with lymphoma and non non- -Hodgkin lymphoproliferative lymphoproliferative with nasopharyngeal nasopharyngeal carcinoma carcinoma Hodgkin lymphomas lymphomas disorders disorders and and in in individuals individuals gastric gastric
Biology of Epstein Biology of Epstein- -Barr Virus Barr Virus The major target cell for EBV is the B lymphocyte. When human B lymphocytes are infected with EBV, continuous cell lines can be established, indicating that cells have been immortalized by the virus. EBV-immortalized differentiated functions, such as secretion of immunoglobulin. B lymphocytes express
Pathogenesis & Pathology Pathogenesis & Pathology Primary Infection EBV is commonly transmitted by infected saliva and initiates infection in the oropharynx. Viral replication occurs in epithelial cells (or surface B lymphocytes) of the pharynx and salivary glands. Many people shed low levels of virus for weeks to months after infection. Infected B cells spread the infection from the oropharynx throughout the body. In normal individuals, most virus-infected cells are eliminated, but small numbers of latently infected lymphocytes persist for the lifetime of the host .
Pathogenesis & Pathology Pathogenesis & Pathology Reactivation from Latency Reactivations of EBV latent infections can occur, as evidenced by increased levels of virus in saliva and of DNA in blood cells. These are usually clinically silent. Immunosuppression is known to reactivate infection, sometimes with serious consequences.
Clinical Findings Clinical Findings Infectious Mononucleosis The typical illness is self-limited and lasts 2-4 weeks. During the disease, there is an increase in the number of circulating white blood cells, with a predominance of lymphocytes. Many of these are large, atypical T lymphocytes. Low-grade fever and malaise may persist for weeks to months after acute illness.
Clinical Findings: Cancer Clinical Findings: Cancer Sera from patients with Burkitt lymphoma or nasopharyngeal carcinoma contain elevated levels of antibody to virus-specific antigens, and the tumor tissues contain EBV DNA and express a limited number of viral genes. Burkitt lymphoma is a tumor of the jaw in African children and young adults. Most African tumors (>90%) contain EBV DNA and express EBNA1 antigen (latent phase antigen). In other parts of the world, only about 20% of Burkitt lymphomas contain EBV DNA. It is speculated that EBV may be involved at an early stage in Burkitt lymphoma by immortalizing B cells.
Epstein Epstein- -Barr Virus Barr Virus
Viral Hepatitis Viral Hepatitis: is a liver inflammation caused by five unrelated hepatotropic viruses Hepatitis A, Hepatitis B, Hepatitis C, Hepatitis D, and Hepatitis E. Other viruses can also cause liver inflammation include Herpes simplex, Cytomegalovirus, Epstein Barr virus. It may present in acute (recent infection, relatively rapid onset) or chronic forms. - Hepatitis viruses Hepatitis A (HAV) Picornaviridae (1973) Hepatitis B (HBV) Hepadnaviridae (1970) Hepatitis C (HCV) Flaviviridae (1988) Hepatitis D (HDV) (1977) Hepatitis E (HEV) (Caliciviridae) (1983) Hepatitis F Not separate entity Mutant of B Virus. Hepatitis G (HGV) Flaviviridae (1995)
Hepatitis A Virus Small, (Naked RNA virus) icosahedral particle, 27 nm in diameter. Related to enteroviruses, formerly known as enterovirus 72, now put in its own family. One stable serotype only. HAV is not cytolytic and is released by exocytosis. ssRNA, non-enveloped
Pathogenesis & Symptoms of Hepatitis A Virus Pathogenesis & Symptoms of Hepatitis A Virus HAV invade into human body by fecal-oral route, multiplies in the intestinal epithelium and reaches the liver by hematogenous spread. After one week, the HAV reach liver cells when replication will occur. Then enter intestine with bile and appear in feces. Incubation Period : 2 to 6 weeks. The clinical symptoms are include: Jaundice (yellow eyes and skin, dark urine) Abdominal pain Loss of appetite Nausea Fever Diarrhea Fatigue Children often have the disease with few symptoms.
Hepatitis A Virus resistance Hepatitis A Virus resistance Stable to: acid at pH 3 Solvents (ether, chloroform) detergents saltwater, groundwater(months) drying(stable) Temperature - 4 : stable for weeks - 56 for 30 minutes: stable - 61 for 20 minutes: partial inactivation
Laboratory Diagnosis Laboratory Diagnosis 1. Demonstration of Virus in feces: By: Immunoelectron microscopy 2. Virus Isolation: by tissue culture. 3. Detection of Antibody :By ELISA 4. Biochemical tests: 5. Molecular Diagnosis : Real-Time PCR of feces i) Alanine aminotransferase (ALT) ii) Bilirubin 25
Hepatitis A Virus vaccine Hepatitis A Virus vaccine Hepatitis A vaccine in infants is safe and immunogenic without maternal antibody. Combined hepatitis A and hepatitis B vaccine approved by FDA in United states for persons above 18 years old. The schedule of this vaccine is: 0,1,6 months.
Hepatitis B Virus Hepatitis B Virus Double stranded DNA enveloped virus. Complete particle 42 nm, the core of the virus containing HBcAg and HBeAg, and the coat contain HBsAg and at least 4 phenotypes of HBsAg are recognized. The HBcAg is of a single serotype. Hepatitis B virus (HBV) has been classified into 8 genotypes (A- H). Available data suggests that genotype produces a milder disease, respond better to IFN therapy, and is less likely to develop hepatocellular carcinoma.
HBV HBV : Structure : Structure Virion also referred to as Dane particle (ds-tranded DNA) 42nm enveloped virus Core antigens located in the center (nucleocapsid) Core antigen (HBcAg) e antigen (HBeAg)- an indicator of transmissibility (minor component of the core- antigenically distinct from HBcAg) 22nm spheres and filaments other forms- no DNA in these forms so they are not infectious (composed of surface antigen)- these forms outnumber the actual virions
Four stages in the viral life cycle (HBV) Four stages in the viral life cycle (HBV) The first stage is immune tolerance. The duration of this stage for healthy adults is approximately 2-4 weeks and represents the incubation period. In the second stage, an inflammatory reaction with a cytopathic effect occurs. HBeAg can be identified in the sera. The duration of this stage for patients with acute infection is approximately 3- 4 weeks (symptomatic period). In the third stage, the host can target the infected hepatocytes and the HBV Viral replication no longer occurs. HBeAb can be detected. In the fourth stage, the virus cannot be detected and antibodies to various viral antigens have been produced.
Clinical symptoms of hepatitis b virus Clinical symptoms of hepatitis b virus Signs and symptoms of hepatitis B, ranging from mild to severe, usually appear about one to four months after you've been infected. Signs and symptoms of hepatitis B may include: Abdominal pain Dark urine Fever Joint pain Loss of appetite Nausea and vomiting Weakness and fatigue jaundice
Clinical Clinical outcomes of Hepatitis B infections outcomes of Hepatitis B infections
Laboratory DIAGNOSIS Laboratory DIAGNOSIS Acute HBV infection is characterized by the presence of HBsAg and immunoglobulin M (IgM) antibody to HBcAg detected by EIA (Enzyme Immunoassay). During the initial phase of infection, patients are seropositive for HBeAg, which is a marker of high levels of replication of the virus. The presence of HBeAg indicates that the blood and body fluids of the infected individual are highly contagious. Chronic infection is characterized by the persistence of HBsAg for at least 6 months (with or without concurrent HBeAg). Persistence of HBeAb is the principal marker of risk for developing chronic liver disease and liver cancer (hepatocellular carcinoma) later in life.
Treatment Treatment There is no specific treatment for acute hepatitis B. Therefore, care is aimed at maintaining comfort and adequate nutritional balance, including replacement of fluids lost from vomiting and diarrhea. Chronic hepatitis B infection can be treated with drugs, including oral antiviral agents, such as tenofovir or entecavir. With nucleoside and nucleotide analogs, such as lamivudine, HBV DNA levels are reduced, but the virus is rarely eliminated and viral replication resumes in the majority of patients when treatment is stopped. The emergence of drug-resistant virus mutants in long-term therapy is a major problem. Interferon - for HBeAg +ve carriers with chronic active hepatitis. Response rate is 30 to 40%. Treatment can slow the progression of cirrhosis, reduce incidence of liver cancer and improve long term survival.
Hepatitis B Vaccine Hepatitis B Vaccine Infants: several options that depend on status of the mother If mother HBsAg negative: birth, 1-2m,6-18m. If mother HBsAg positive: vaccine and Hep B immune globulin within 12 hours of birth, 1-2m, <6m. Adults: 0,1, 6 months. Vaccine recommended in All those aged 0-18, and those at high risk.
Hepatitis C Virus (HCV) Hepatitis C Virus (HCV) Positive stranded RNA genome of around 10,000 bases Enveloped virus, virion, 30-60nm in diameter Morphological structure remains unknown HCV has been classified into a total of six genotypes (type 1 to 6) on the basis of phylogenetic analysis Genotype 1 and 4 has a poorer prognosis and response to interferon therapy. HCV can cause acute infections but is more likely to establish chronic infections. All the manifestations of chronic hepatitis B infection may be seen, but with a lower frequency i.e. chronic persistent hepatitis, chronic active hepatitis, cirrhosis, and hepatocellular carcinoma.
Natural history of HCV Natural history of HCV
Laboratory Diagnosis Laboratory Diagnosis HCV antibody - generally used to diagnose hepatitis C infection. Not useful in the acute phase as it takes at least 4 weeks after infection before antibody appears. HCV-RNA - various techniques are available e.g. PCR. May be used to diagnose HCV infection in the acute phase. However, its main use is in monitoring the response to antiviral therapy. HCV-antigen - an EIA for HCV antigen is available. It is used in the same capacity as HCV-RNA tests but is much easier to carry out.
Treatment & prevention Treatment & prevention Treatment: Interferon - may be considered for patients with chronic active hepatitis. The response rate is around 50% but 50% of responders will relapse upon withdrawal of treatment. Ribavirin - there is less experience with ribavirin than interferon. However, recent studies suggest that a combination of interferon and ribavirin is more effective than interferon alone. Prevention: Screening of blood, organ, and tissue. High risk behavior modification. Blood and body fluid precautions.
Hepatitis D Virus Hepatitis D Virus The delta agent is a defective virus. The agent consists of a particle 35 nm in diameter consisting of the delta antigen surrounded by an outer coat of HBsAg. The genome of the virus is very small and consists of a single- stranded RNA. Hepatitis D - Clinical Features: Co-infection Severe acute disease. Low risk of chronic infection. Hepatitis D Prevention Pre or postexposure prophylaxis to prevent HBV infection reduces the HBV-HDV Coinfection. And education to reduce risk behaviors among persons with chronic HBV infection.
Hepatitis E Virus Hepatitis E Virus Calicivirus-like viruses unenveloped RNA virus, 32-34 nm in diameter +ve stranded RNA genome, 7.6 kb in size. very labile and sensitive Prevention of HEV Avoid drinking water and beverages of unknown purity, uncooked shellfish, and unwashed fruit/vegetables. IG prepared from donors in Western countries does not prevent infection. Unknown efficacy of IG prepared from donors in endemic areas.
Thank You Thank You





























")





")