Helicobacter pylori: Morphology, Pathogenesis, and Identification
 undefined
undefined
M
e
d
i
c
a
l
M
i
c
r
o
b
i
o
l
o
g
y
A
s
s
t
.
P
r
o
f
.
D
r
.
D
a
l
y
a
B
a
s
i
l

I
n
t
h
i
s
l
e
c
t
u
r
e
…
…
.
Helicobacter
Campylobacter

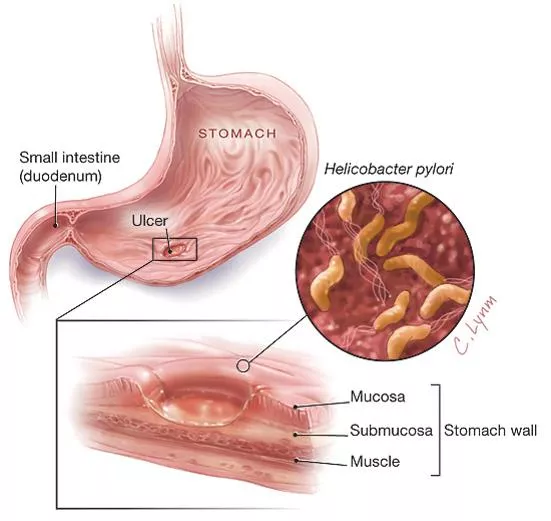
Helicobacter pylori
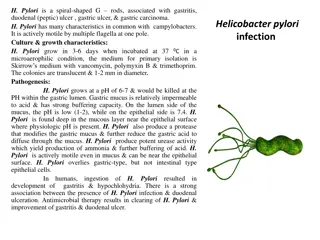
Helicobacter pylori
is a spiral-shaped gram-negative rod.
H pylori
is associated with antral gastritis, duodenal
(peptic) ulcer disease, gastric ulcers, and gastric
carcinoma. Other
Helicobacter
species that infect the
gastric mucosa exist but are rare.
M
o
r
p
h
o
l
o
g
y
&
I
d
e
n
t
i
f
i
c
a
t
i
o
n
Typical Organisms
H pylori
has multiple flagella at one pole and is actively motile.
Culture
Culture sensitivity can be limited by prior therapy, contamination with
other mucosal bacteria, and other factors.
H pylori
grows in 3–6 days
when incubated at 37°C in a microaerophilic environment. The media
for primary isolation include Skirrow's medium with vancomycin,
polymyxin B, and trimethoprim, chocolate medium, and other
selective media with antibiotics (eg, vancomycin, nalidixic acid,
amphotericin). The colonies are translucent and 1–2 mm in diameter.
Growth Characteristics
H pylori
is oxidase-positive and catalase-positive, has a characteristic
morphology, is motile, and is a strong producer of urease.
P
a
t
h
o
g
e
n
e
s
i
s
&
P
a
t
h
o
l
o
g
y
H pylori
grows optimally at a pH of 6.0–7.0 and would be killed or not
grow at the pH within the gastric lumen. Gastric mucus is relatively
impermeable to acid and has a strong buffering capacity. On the
lumen side of the mucus, the pH is low (1.0–2.0) while on the
epithelial side the pH is about 7.4.
H pylori
is found deep in the
mucous layer near the epithelial surface where physiologic pH is
present.
H pylori
also produces a protease that modifies the gastric mucus and
further reduces the ability of acid to diffuse through the mucus.
H pylori
produces potent urease activity, which yields production of
ammonia and further buffering of acid.
H pylori
is quite motile, even in mucus, and is able to find its way to
the epithelial surface.
H pylori
overlies gastric-type but not intestinal-
type epithelial cells.
P
a
t
h
o
g
e
n
e
s
i
s
&
P
a
t
h
o
l
o
g
y
P
a
t
h
o
g
e
n
e
s
i
s
&
P
a
t
h
o
l
o
g
y
The mechanisms by which
H pylori
causes mucosal inflammation and
damage are not well defined but
probably involve both bacterial and
host factors. The bacteria invade the
epithelial cell surface to a limited
degree. Toxins and
lipopolysaccharide may damage the
mucosal cells, and the ammonia
produced by the urease activity may
directly damage the cells also.
P
a
t
h
o
g
e
n
e
s
i
s
&
P
a
t
h
o
l
o
g
y
Histologically, gastritis is characterized by chronic and active inflammation.
Polymorphonuclear and mononuclear cell infiltrates are seen within the
epithelium and lamina propria. Vacuoles within cells are often pronounced.
Destruction of the epithelium is common, and glandular atrophy may occur.
H
pylori
thus may be a major risk factor for gastric cancer.
C
l
i
n
i
c
a
l
F
i
n
d
i
n
g
s
Acute infection can yield an upper gastrointestinal illness with nausea and
pain; vomiting and fever may be present also. The acute symptoms may last
for less than 1 week or as long as 2 weeks. Once colonized, the
H pylori
infection persists for years and perhaps decades or even a lifetime. About 90%
of patients with duodenal ulcers and 50–80% of those with gastric ulcers have
H pylori
infection.
D
i
a
g
n
o
s
t
i
c
L
a
b
o
r
a
t
o
r
y
T
e
s
t
s
Specimens
Gastric biopsy specimens can be used for histologic examination or minced in saline
and
used for culture. Blood is collected for determination of serum antibodies.
Smears
The diagnosis of gastritis and
H pylori
infection can be made histologically.
A gastroscopy procedure with biopsy is required. Routine stains demonstrate gastritis,
and
Giemsa or special silver stains can show the curved or spiraled organisms.
Culture
Skirrow's medium with vancomycin, polymyxin B, and trimethoprim, chocolate
medium, and
other selective media.
Antibodies
Several assays have been developed to detect serum antibodies specific for
H pylori.
The
serum antibodies persist even if the
H pylori
infection is eradicated, and the role
of antibody tests in diagnosing active infection or following therapy is therefore
limited.
D
i
a
g
n
o
s
t
i
c
L
a
b
o
r
a
t
o
r
y
T
e
s
t
s
Special Tests
Rapid tests to detect urease activity
are widely used for presumptive
identification of
H pylori
in specimens. Gastric biopsy material can be placed
onto a urea-containing medium with a color indicator. If
H pylori
is present,
the urease rapidly splits the urea (1–2 days) and the resulting shift in pH
yields a color change in the medium.
Detection of H pylori antigen in stool specimens
is appropriate as a test of
cure for patients with known
H pylori
infection who have been treated.
Breathing test
13
C- or
14
C-labeled urea is ingested by the patient. If
H pylori
is present, the urease activity generates labeled CO
2
that can be detected in
the patient's exhaled breath.
T
r
e
a
t
m
e
n
t
&
C
o
n
t
r
o
l
Treatment
Triple therapy: metronidazole and either bismuth subsalicylate or bismuth
subcitrate plus either amoxicillin or tetracycline for 14 days eradicates
H. pylori
infection in 70–95% of patients. An acid-suppressing agent given for 4–6 weeks
enhances ulcer healing. Proton pump inhibitors directly inhibit
H pylori
and
appear to be potent urease inhibitors. Either 1 week of a proton pump inhibitor
plus amoxicillin and clarithromycin or of amoxicillin plus metronidazole also is
highly effective.
Epidemiology & Control
H pylori
is present on the gastric mucosa of less than 20% of persons under age
30 but increases in prevalence to 40–60% of persons age 60, including persons
who are asymptomatic. In developing countries, the prevalence of infection may
be 80% or higher in adults. Person-to-person transmission of
H pylori
is likely
because intrafamilial clustering of infection occurs.
C
a
m
p
y
l
o
b
a
c
t
e
r
Campylobacters cause both diarrheal and systemic diseases and are among
the most widespread causes of infection in the world. The classification of
bacteria within the family Campylobacteriaceae has changed frequently.
Some species previously classified as campylobacters have been reclassified in
the genus
Helicobacter
. The genus
Arcobacter
has been created.
C jejuni
is the prototype organism in the group and is a very common cause of
diarrhea in humans.
C
a
m
p
y
l
o
b
a
c
t
e
r
j
e
j
u
n
i
&
C
a
m
p
y
l
o
b
a
c
t
e
r
c
o
l
i
C jejuni
and
Campylobacter coli
have emerged as common human pathogens,
causing mainly enteritis and occasionally systemic infection.
C jejuni
and
C coli
cause infections that are clinically indistinguishable, and
laboratories generally do not differentiate between the two species. Between
5% and 10% of infections reported to be caused by
C jejuni
are probably
caused by
C coli.
These bacteria are at least as common as salmonellae and
shigellae as a cause of diarrhea; an estimated 2 million cases occur in the
United States each year.
M
o
r
p
h
o
l
o
g
y
&
I
d
e
n
t
i
f
i
c
a
t
i
o
n
Typical Organisms
C jejuni
and the other campylobacters are gram-negative rods with comma,
S, or "gull wing" shapes. They are motile, with a single polar flagellum, and do
not form spores.
C
u
l
t
u
r
e
The culture characteristics are most important in the isolation and
identification of
C jejuni
and the other campylobacters. Selective media are
needed, and incubation must be in an atmosphere with reduced O
2
(5% O
2
)
with added CO
2
(10% CO
2
). A relatively simple way to produce the incubation
atmosphere is to place the plates in an anaerobe incubation jar and to
produce the gas with a commercially available gas-generating pack or by gas
exchange. Incubation of primary plates for isolation of
C jejuni
should be at
42°C. Although
C jejuni
grows well at 36–37°C, incubation at 42°C prevents
growth of most of the other bacteria present in feces, thus simplifying the
identification of
C jejuni.
C
u
l
t
u
r
e
Several selective media are in widespread use. Skirrow's medium
contains vancomycin, polymyxin B, and trimethoprim to inhibit growth
of other bacteria.
Other selective media also contain antimicrobials, including
cephalothin or cefoperazone, and inhibitory compounds; because they
contain a cephalosporin, they will not grow
Campylobacter fetus
and
several other
Campylobacter
species. The selective media are
suitable for isolation of
C jejuni
at 42°C; when media without
antibiotics are incubated at 36–37°C, other campylobacters may be
isolated. The colonies tend to be colorless or gray. They may be
watery and spreading or round and convex, and both colony types may
appear on one agar plate.
P
a
t
h
o
g
e
n
e
s
i
s
&
P
a
t
h
o
l
o
g
y
The infection is acquired by the oral route from food,
drink, or contact with infected animals or animal
products.
C jejuni
is susceptible to gastric acid, and
ingestion of about 10
4
organisms is usually necessary to
produce infection.
The organisms multiply in the small intestine, invade the
epithelium, and produce inflammation that results in the
appearance of red and white blood cells in the stools.
Occasionally, the bloodstream is invaded and a clinical
picture of enteric fever develops. Localized tissue
invasion coupled with the toxic activity appears to be
responsible for the enteritis.
C
l
i
n
i
c
a
l
F
i
n
d
i
n
g
s
Clinical manifestations are acute onset of crampy abdominal pain,
profuse diarrhea that may be grossly bloody, headache, malaise, and
fever. Usually the illness is self-limited to a period of 5–8 days, but
occasionally it continues longer.
C jejuni
isolates are usually
susceptible to erythromycin, and therapy shortens the duration of
fecal shedding of bacteria. Most cases resolve without antimicrobial
therapy.
D
i
a
g
n
o
s
t
i
c
L
a
b
o
r
a
t
o
r
y
T
e
s
t
s
Specimens
Diarrheal stool is the usual specimen. Campylobacters from other
types of specimens are usually incidental findings or are found in the
setting of known outbreaks of disease.
Smears
Gram-stained smears of stool may show the typical "gull wing"-shaped
rods. Dark-field or phase contrast microscopy may show the typical
darting motility of the organisms.
Culture
Culture on the selective media is the definitive test to diagnose
C
jejuni
enteritis. If another species of
Campylobacter
is suspected,
medium without a cephalosporin should be used and incubated at 36–
37°C.
E
p
i
d
e
m
i
o
l
o
g
y
&
C
o
n
t
r
o
l
Campylobacter enteritis
resembles other acute bacterial
diarrheas, particularly shigella dysentery. The source of
infection may be food (eg, milk, undercooked fowl) or
contact with infected animals or humans and their
excreta. Outbreaks arising from a common source, eg,
unpasteurized milk, may require public health control
measures.
C
a
m
p
y
l
o
b
a
c
t
e
r
f
e
t
u
s
C fetus
subspecies
fetus
is an opportunistic pathogen that
causes systemic infections in immunocompromised
patients. It may occasionally cause diarrhea.
The gastrointestinal tract may be the portal of entry when
C fetus
causes bacteremia and systemic infection.
C fetus
has several surface array proteins (S protein, MW 100,000–
149,000) which form a capsule-like structure on the
surface of the organism (as compared with the
polysaccharide capsules of pathogens such as
Neisseria
meningitidis
and
Streptococcus pneumoniae
).
T
T
h
h
a
a
n
n
k
k
Y
Y
o
o
u
u
In this detailed lecture, Assistant Professor Dr. Dalya Basil discusses the characteristics, identification methods, growth characteristics, and pathogenesis of Helicobacter pylori. This spiral-shaped, gram-negative rod bacterium is associated with various gastric conditions, including gastritis, ulcers, and even gastric carcinoma. The content covers key aspects such as morphology, culture sensitivity, growth requirements, and mechanisms through which H. pylori causes mucosal damage, involving both bacterial and host factors.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Medical Microbiology Asst. Prof. Dr. Dalya Basil
In this lecture. Helicobacter Campylobacter
Helicobacter pylori Helicobacter pylori is a spiral-shaped gram-negative rod. H pylori is associated with antral gastritis, duodenal (peptic) ulcer disease, gastric carcinoma. Other Helicobacter species that infect the gastric mucosa exist but are rare. ulcers, and gastric
Morphology & Identification Typical Organisms H pylori has multiple flagella at one pole and is actively motile. Culture Culture sensitivity can be limited by prior therapy, contamination with other mucosal bacteria, and other factors. H pylori grows in 3 6 days when incubated at 37 C in a microaerophilic environment. The media for primary isolation include Skirrow's medium with vancomycin, polymyxin B, and trimethoprim, chocolate medium, and other selective media with antibiotics (eg, vancomycin, nalidixic acid, amphotericin). The colonies are translucent and 1 2 mm in diameter. Growth Characteristics H pylori is oxidase-positive and catalase-positive, has a characteristic morphology, is motile, and is a strong producer of urease.
Pathogenesis & Pathology H pylori grows optimally at a pH of 6.0 7.0 and would be killed or not grow at the pH within the gastric lumen. Gastric mucus is relatively impermeable to acid and has a strong buffering capacity. On the lumen side of the mucus, the pH is low (1.0 2.0) while on the epithelial side the pH is about 7.4. H pylori is found deep in the mucous layer near the epithelial surface where physiologic pH is present. H pylori also produces a protease that modifies the gastric mucus and further reduces the ability of acid to diffuse through the mucus. H pylori produces potent urease activity, which yields production of ammonia and further buffering of acid. H pylori is quite motile, even in mucus, and is able to find its way to the epithelial surface. H pylori overlies gastric-type but not intestinal- type epithelial cells.
Pathogenesis & Pathology The mechanisms by which H pylori causes mucosal damage are not well defined but probably involve both bacterial and host factors. The bacteria invade the epithelial cell surface to a limited degree. lipopolysaccharide may damage the mucosal cells, produced by the urease activity may directly damage the cells also. inflammation and Toxins and and the ammonia
Pathogenesis & Pathology Histologically, gastritis is characterized by chronic and active inflammation. Polymorphonuclear and mononuclear cell infiltrates are seen within the epithelium and lamina propria. Vacuoles within cells are often pronounced. Destruction of the epithelium is common, and glandular atrophy may occur. H pylori thus may be a major risk factor for gastric cancer.
Clinical Findings Acute infection can yield an upper gastrointestinal illness with nausea and pain; vomiting and fever may be present also. The acute symptoms may last for less than 1 week or as long as 2 weeks. Once colonized, the H pylori infection persists for years and perhaps decades or even a lifetime. About 90% of patients with duodenal ulcers and 50 80% of those with gastric ulcers have H pylori infection.
Diagnostic Laboratory Tests Specimens Gastric biopsy specimens can be used for histologic examination or minced in saline and used for culture. Blood is collected for determination of serum antibodies. Smears The diagnosis of gastritis and H pylori infection can be made histologically. A gastroscopy procedure with biopsy is required. Routine stains demonstrate gastritis, and Giemsa or special silver stains can show the curved or spiraled organisms. Culture Skirrow's medium with vancomycin, polymyxin B, and trimethoprim, chocolate medium, and other selective media. Antibodies Several assays have been developed to detect serum antibodies specific for H pylori. The serum antibodies persist even if the H pylori infection is eradicated, and the role of antibody tests in diagnosing active infection or following therapy is therefore limited.
Diagnostic Laboratory Tests Special Tests Rapid tests to detect urease activity are widely used for presumptive identification of H pylori in specimens. Gastric biopsy material can be placed onto a urea-containing medium with a color indicator. If H pylori is present, the urease rapidly splits the urea (1 2 days) and the resulting shift in pH yields a color change in the medium. Detection of H pylori antigen in stool specimens is appropriate as a test of cure for patients with known H pylori infection who have been treated. Breathing test13C- or14C-labeled urea is ingested by the patient. If H pylori is present, the urease activity generates labeled CO2that can be detected in the patient's exhaled breath.
Treatment & Control Treatment Triple therapy: metronidazole and either bismuth subsalicylate or bismuth subcitrate plus either amoxicillin or tetracycline for 14 days eradicates H. pylori infection in 70 95% of patients. An acid-suppressing agent given for 4 6 weeks enhances ulcer healing. Proton pump inhibitors directly inhibit H pylori and appear to be potent urease inhibitors. Either 1 week of a proton pump inhibitor plus amoxicillin and clarithromycin or of amoxicillin plus metronidazole also is highly effective. Epidemiology & Control H pylori is present on the gastric mucosa of less than 20% of persons under age 30 but increases in prevalence to 40 60% of persons age 60, including persons who are asymptomatic. In developing countries, the prevalence of infection may be 80% or higher in adults. Person-to-person transmission of H pylori is likely because intrafamilial clustering of infection occurs.
Campylobacter Campylobacters cause both diarrheal and systemic diseases and are among the most widespread causes of infection in the world. The classification of bacteria within the family Campylobacteriaceae has changed frequently. Some species previously classified as campylobacters have been reclassified in the genus Helicobacter. The genus Arcobacter has been created. C jejuni is the prototype organism in the group and is a very common cause of diarrhea in humans.
Campylobacter jejuni & Campylobacter coli C jejuni and Campylobacter coli have emerged as common human pathogens, causing mainly enteritis and occasionally systemic infection. C jejuni and C coli cause infections that are clinically indistinguishable, and laboratories generally do not differentiate between the two species. Between 5% and 10% of infections reported to be caused by C jejuni are probably caused by C coli. These bacteria are at least as common as salmonellae and shigellae as a cause of diarrhea; an estimated 2 million cases occur in the United States each year.
Morphology & Identification Typical Organisms C jejuni and the other campylobacters are gram-negative rods with comma, S, or "gull wing" shapes. They are motile, with a single polar flagellum, and do not form spores.
Culture The culture characteristics are most important in the isolation and identification of C jejuni and the other campylobacters. Selective media are needed, and incubation must be in an atmosphere with reduced O2(5% O2) with added CO2(10% CO2). A relatively simple way to produce the incubation atmosphere is to place the plates in an anaerobe incubation jar and to produce the gas with a commercially available gas-generating pack or by gas exchange. Incubation of primary plates for isolation of C jejuni should be at 42 C. Although C jejuni grows well at 36 37 C, incubation at 42 C prevents growth of most of the other bacteria present in feces, thus simplifying the identification of C jejuni.
Culture Several selective media are in widespread use. Skirrow's medium contains vancomycin, polymyxin B, and trimethoprim to inhibit growth of other bacteria. Other cephalothin or cefoperazone, and inhibitory compounds; because they contain a cephalosporin, they will not grow Campylobacter fetus and several other Campylobacter species. The selective media are suitable for isolation of C jejuni at 42 C; when media without antibiotics are incubated at 36 37 C, other campylobacters may be isolated. The colonies tend to be colorless or gray. They may be watery and spreading or round and convex, and both colony types may appear on one agar plate. selective media also contain antimicrobials, including
Pathogenesis & Pathology The infection is acquired by the oral route from food, drink, or contact with infected products. C jejuni is susceptible to gastric acid, and ingestion of about 104organisms is usually necessary to produce infection. animals or animal The organisms multiply in the small intestine, invade the epithelium, and produce inflammation that results in the appearance of red and white blood cells in the stools. Occasionally, the bloodstream is invaded and a clinical picture of enteric fever invasion coupled with the toxic activity appears to be responsible for the enteritis. develops. Localized tissue
Clinical Findings Clinical manifestations are acute onset of crampy abdominal pain, profuse diarrhea that may be grossly bloody, headache, malaise, and fever. Usually the illness is self-limited to a period of 5 8 days, but occasionally it continues longer. C jejuni isolates are usually susceptible to erythromycin, and therapy shortens the duration of fecal shedding of bacteria. Most cases resolve without antimicrobial therapy.
Diagnostic Laboratory Tests Specimens Diarrheal stool is the usual specimen. Campylobacters from other types of specimens are usually incidental findings or are found in the setting of known outbreaks of disease. Smears Gram-stained smears of stool may show the typical "gull wing"-shaped rods. Dark-field or phase contrast microscopy may show the typical darting motility of the organisms. Culture Culture on the selective media is the definitive test to diagnose C jejuni enteritis. If another species of Campylobacter is suspected, medium without a cephalosporin should be used and incubated at 36 37 C.
Epidemiology & Control Campylobacter enteritis resembles other acute bacterial diarrheas, particularly shigella dysentery. The source of infection may be food (eg, milk, undercooked fowl) or contact with infected animals or humans and their excreta. Outbreaks arising from a common source, eg, unpasteurized milk, may require public health control measures.
Campylobacter fetus C fetus subspecies fetus is an opportunistic pathogen that causes systemic infections patients. It may occasionally cause diarrhea. in immunocompromised The gastrointestinal tract may be the portal of entry when C fetus causes bacteremia and systemic infection. C fetus has several surface array proteins (S protein, MW 100,000 149,000) which form a capsule-like structure on the surface of the organism polysaccharide capsules of pathogens such as Neisseria meningitidis and Streptococcus pneumoniae). (as compared with the