Death and Dying in Human Life


PSYCH 092
–
chapter nineteen
DEATH, DYING, AND BEREAVEMENT
HOW WE DIE
The interdisciplinary field of
thanatology
has expanded tremendously over
the past three decades.
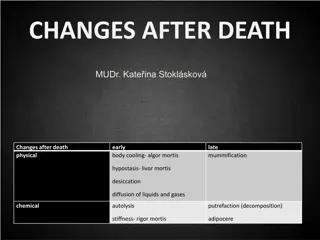
Death is long and drawn out for about three-fourths of people, as a result of
life-saving medical technology.
When the transition from life to death is imminent, the person often moves
through three phases: the
agonal phase
,
clinical death,
and
mortality
, or
permanent death.
Today,
brain death
is used as the definition of death in most industrialized
nations.
When the cerebral cortex no longer registers electrical activity but the brain
stem remains active, a person has entered a
persistent vegetative state
.
Dignity in death is fostered by offering the dying person care, affection,
companionship, and esteem; the truth about diagnosis; and maximum
personal control.

PSYCH 092
–
chapter nineteen
UNDERSTANDING OF AND ATTITUDES TOWARD DEATH
Compared with earlier generations, today more young people reach adulthood
without having experienced the death of someone they know well.
An accurate, biological understanding of death is based on five subconcepts:
nonfunctionality, finality, universality, applicability,
and
causation.
Children typically attain an adultlike, biological understanding of death by the
end of early childhood, but cultural and religious ideas influence their rate of
mastery and how they acquire information.
Children with a good grasp of the facts of death express less anxiety about it.
Teenagers can explain death subconcepts of nonfunctionality and finality, but
they also formulate personal theories about life after death.
Although adolescents are clearly aware that death can occur at any time, their
high-risk activities suggest that they do not take death personally.

PSYCH 092
–
chapter nineteen
In late adulthood, adults think and talk more about death because it is much
closer.
Even people who clearly accept the reality of death may experience
death
anxiety.
People who are depressed or generally anxious are likely to have more severe
death concerns, whereas people who are good at inhibition and at emotional
self-regulation report less death anxiety.
Death anxiety is rarely seen in children except for those who live in high-crime
neighborhoods or war-torn areas, or who are terminally ill.
THINKING AND EMOTIONS OF DYING PEOPLE
Elisabeth Kubler-Ross is credited with awakening society’s sensitivity to the
psychological needs of dying patients, although her theory has been heavily
criticized.
PSYCH 092
–
chapter nineteen
Kubler-Ross devised a theory of five typical responses
–
initially proposed as stages
–
to
the prospect of death and dying:
denial, anger, bargaining, depression,
and
acceptance
.
Although Kubler-Ross cautioned that her five stages should not be viewed as a fixed,
universal sequence, her theory has often been interpreted simplistically, as a universal,
linear sequence.
The reactions Kubler-Ross observed are best viewed as coping strategies that anyone
may call on in the face of threat.
An
appropriate death
makes sense in terms of the individual’s pattern of living and
values, preserves or restores significant relationships, and is as free of suffering as
possible.
Biological, psychological, social, and social and cultural forces influence how people cope
with dying.
The course of the final illness and its symptoms affect the dying person’s reactions.
Vastly different cultural beliefs, guided by religious ideas, also shape people’s dying
experiences.
PSYCH 092
–
chapter nineteen
A PLACE TO DIE
In the past most deaths occurred at home, but in the U.S. today about 40 percent
take place in hospitals and another 20 percent in long-term facilities.
In the 1960s, a death awareness movement led to medical care in hospitals
better suited to the needs of dying people and also to hospice programs.
The preference of 80 percent of Americans is to die at home, but only about one-
fourth experience home death.
To make dying at home feasible, adequate support for the caregiver is essential.
THE RIGHT TO DIE
Today, all U.S. states have laws that honor patients’ wishes concerning
withdrawal of treatment in cases of terminal illness and, sometimes, in cases of a
persistent vegetative state, but no uniform right-to-die policy exists.
PSYCH 092
–
chapter nineteen
People can best ensure that their end-of-life wishes will be followed by preparing
an
advance medical directive
–
either a
living will
or a
durable power of
attorney for health care
.
Only 45 percent of Americans over age 40 have executed such documents, but
nearly 55 percent of adults over age 65 have them.
In
medical aid-in-dying
, at an incurably ill patient’s request, a doctor provides a
prescription for a lethal dose of drugs, which the patient self-administers to end
his or her life. Until recently, it was widely referred to as
physician-assisted
suicide
.
Medical aid-in-dying is legal in five U.S. states (Oregon, Washington, Montana,
Vermont, and California) and six other nations: Belgium, the Netherlands,
Luxembourg, Switzerland, Columbia, and Canada.
Opponents claim that legalizing medical aid-in-dying poses risks; the American
Academy of Hospice and Palliative Medicine has expressed concern about aid-in-
dying becoming part of routine medical practice.
PSYCH 092
–
chapter nineteen
In
voluntary euthanasia
, at a patient’s request, a doctor actively takes the
patient’s life in a painless way for the purpose of relieving suffering. It is a
criminal offense in all U.S. states and most other countries, but courts are usually
lenient with the doctors who engaged in it.
Even where it is legal in restricted circumstances, voluntary euthanasia poses
profound ethical dilemmas.
BEREAVEMENT: COPING WITH THE DEATH OF A LOVED ONE
We respond to
bereavement
, the loss of a loved one by death, with
grief
: intense
physical and psychological distress.
Mourning
is the culturally specified expression of the bereaved person’s
thoughts and feelings.
About 5 to 15 percent of bereaved persons experience severe, prolonged
distress, termed
complicated grief.
PSYCH 092
–
chapter nineteen
The grief process is best conceived as a set of
tasks:
to accept the reality of the
loss, to work through the pain of grief, to adjust to a world without the loved one,
and to develop an inner bond with the deceased and move on with life.
Many survivors react with avoidance, which gives way to a cascade of emotional
reactions.
According to the
dual-process of coping with loss
, effective coping requires
people to oscillate between dealing with the emotional consequences of loss and
attending to life changes, which
–
when handled successfully
–
have restorative,
or healing, effects.
Grieving is affected by many factors, including personality, coping style, and
religious and cultural background.
Men typically express distress and depression less directly than women do and
seek social support less readily.
During prolonged dying, the bereaved person has had time to engage in
anticipatory grieving.
PSYCH 092
–
chapter nineteen
The death of a child is the most difficult loss an adult can face.
Aging adults are at risk for bereavement overload because old age often brings
several deaths in close succession, but older adults are often better equipped
than young people to handle these losses.
Public tragedies, such as terrorist attacks and random murders in schools, can
spark bereavement overload.
When people experience several deaths in succession, bereavement overload
can occur, leaving them emotionally overwhelmed, severely depressed, and
vulnerable to post-traumatic stress symptoms and complicated grief.
In some instances
–
for example, a sudden, violent, and unexplainable death or
the loss of a child
–
individual or family therapy with a specially trained
professional can be helpful in dealing with complicated grief.
Exploring the interdisciplinary field of thanatology, this chapter delves into the phases of transitioning from life to death, the definition of death in modern society, and how individuals of different ages perceive and cope with the concept of death. It discusses the importance of providing care and dignity to the dying, examines children's understanding of death, and analyzes the attitudes towards death in late adulthood. The chapter also introduces Elisabeth Kubler-Ross's theory of five typical responses to death and dying, highlighting the complexities of individuals' coping strategies in the face of mortality.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
PSYCH 092 chapter nineteen Almost-death experiences
PSYCH 092 chapter nineteen DEATH, DYING, AND BEREAVEMENT HOW WE DIE The interdisciplinary field of thanatology has expanded tremendously over the past three decades. Death is long and drawn out for about three-fourths of people, as a result of life-saving medical technology. When the transition from life to death is imminent, the person often moves through three phases: the agonal phase, clinical death, and mortality, or permanent death. Today, brain death is used as the definition of death in most industrialized nations. When the cerebral cortex no longer registers electrical activity but the brain stem remains active, a person has entered a persistent vegetative state. Dignity in death is fostered by offering the dying person care, affection, companionship, and esteem; the truth about diagnosis; and maximum personal control.
PSYCH 092 chapter nineteen UNDERSTANDING OF AND ATTITUDES TOWARD DEATH Compared with earlier generations, today more young people reach adulthood without having experienced the death of someone they know well. An accurate, biological understanding of death is based on five subconcepts: nonfunctionality, finality, universality, applicability, and causation. Children typically attain an adultlike, biological understanding of death by the end of early childhood, but cultural and religious ideas influence their rate of mastery and how they acquire information. Children with a good grasp of the facts of death express less anxiety about it. Teenagers can explain death subconcepts of nonfunctionality and finality, but they also formulate personal theories about life after death. Although adolescents are clearly aware that death can occur at any time, their high-risk activities suggest that they do not take death personally.
PSYCH 092 chapter nineteen In late adulthood, adults think and talk more about death because it is much closer. Even people who clearly accept the reality of death may experience death anxiety. People who are depressed or generally anxious are likely to have more severe death concerns, whereas people who are good at inhibition and at emotional self-regulation report less death anxiety. Death anxiety is rarely seen in children except for those who live in high-crime neighborhoods or war-torn areas, or who are terminally ill. THINKING AND EMOTIONS OF DYING PEOPLE Elisabeth Kubler-Ross is credited with awakening society s sensitivity to the psychological needs of dying patients, although her theory has been heavily criticized.
PSYCH 092 chapter nineteen Kubler-Ross devised a theory of five typical responses initially proposed as stages to the prospect of death and dying: denial, anger, bargaining, depression, and acceptance. Although Kubler-Ross cautioned that her five stages should not be viewed as a fixed, universal sequence, her theory has often been interpreted simplistically, as a universal, linear sequence. The reactions Kubler-Ross observed are best viewed as coping strategies that anyone may call on in the face of threat. An appropriate death makes sense in terms of the individual s pattern of living and values, preserves or restores significant relationships, and is as free of suffering as possible. Biological, psychological, social, and social and cultural forces influence how people cope with dying. The course of the final illness and its symptoms affect the dying person s reactions. Vastly different cultural beliefs, guided by religious ideas, also shape people s dying experiences.
PSYCH 092 chapter nineteen A PLACE TO DIE In the past most deaths occurred at home, but in the U.S. today about 40 percent take place in hospitals and another 20 percent in long-term facilities. In the 1960s, a death awareness movement led to medical care in hospitals better suited to the needs of dying people and also to hospice programs. The preference of 80 percent of Americans is to die at home, but only about one- fourth experience home death. To make dying at home feasible, adequate support for the caregiver is essential. THE RIGHT TO DIE Today, all U.S. states have laws that honor patients wishes concerning withdrawal of treatment in cases of terminal illness and, sometimes, in cases of a persistent vegetative state, but no uniform right-to-die policy exists.
PSYCH 092 chapter nineteen People can best ensure that their end-of-life wishes will be followed by preparing an advance medical directive either a living will or a durable power of attorney for health care. Only 45 percent of Americans over age 40 have executed such documents, but nearly 55 percent of adults over age 65 have them. In medical aid-in-dying, at an incurably ill patient s request, a doctor provides a prescription for a lethal dose of drugs, which the patient self-administers to end his or her life. Until recently, it was widely referred to as physician-assisted suicide. Medical aid-in-dying is legal in five U.S. states (Oregon, Washington, Montana, Vermont, and California) and six other nations: Belgium, the Netherlands, Luxembourg, Switzerland, Columbia, and Canada. Opponents claim that legalizing medical aid-in-dying poses risks; the American Academy of Hospice and Palliative Medicine has expressed concern about aid-in- dying becoming part of routine medical practice.
PSYCH 092 chapter nineteen In voluntary euthanasia, at a patient s request, a doctor actively takes the patient s life in a painless way for the purpose of relieving suffering. It is a criminal offense in all U.S. states and most other countries, but courts are usually lenient with the doctors who engaged in it. Even where it is legal in restricted circumstances, voluntary euthanasia poses profound ethical dilemmas. BEREAVEMENT: COPING WITH THE DEATH OF A LOVED ONE We respond to bereavement, the loss of a loved one by death, with grief: intense physical and psychological distress. Mourning is the culturally specified expression of the bereaved person s thoughts and feelings. About 5 to 15 percent of bereaved persons experience severe, prolonged distress, termed complicated grief.
PSYCH 092 chapter nineteen The grief process is best conceived as a set of tasks: to accept the reality of the loss, to work through the pain of grief, to adjust to a world without the loved one, and to develop an inner bond with the deceased and move on with life. Many survivors react with avoidance, which gives way to a cascade of emotional reactions. According to the dual-process of coping with loss, effective coping requires people to oscillate between dealing with the emotional consequences of loss and attending to life changes, which when handled successfully have restorative, or healing, effects. Grieving is affected by many factors, including personality, coping style, and religious and cultural background. Men typically express distress and depression less directly than women do and seek social support less readily. During prolonged dying, the bereaved person has had time to engage in anticipatory grieving.
PSYCH 092 chapter nineteen The death of a child is the most difficult loss an adult can face. Aging adults are at risk for bereavement overload because old age often brings several deaths in close succession, but older adults are often better equipped than young people to handle these losses. Public tragedies, such as terrorist attacks and random murders in schools, can spark bereavement overload. When people experience several deaths in succession, bereavement overload can occur, leaving them emotionally overwhelmed, severely depressed, and vulnerable to post-traumatic stress symptoms and complicated grief. In some instances for example, a sudden, violent, and unexplainable death or the loss of a child individual or family therapy with a specially trained professional can be helpful in dealing with complicated grief.