Comprehensive Approach to Heart Failure Management in the Community
This detailed guide covers the signs of decompensation in heart failure patients, actions to take in primary care including diagnostic tests like echocardiograms, and treatment strategies for fluid overload, blood pressure control, heart rate management, and comorbidities like COPD and renal issues. It also outlines when to refer patients with specific BNP levels and ejection fractions to specialist care, and provides contact information for the Heart Failure Team.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Heart Failure Management in the Community Date 18th May 2023 Michelle Thomas Heart Failure Specialist Nurse Team Leader
What will you see in Primary Care? Clinical signs of decompensation Fluid overload / increased oedema/weight gain Decreased appetite Palpitations Increased breathlessness Weight loss Increased fatigue Change in NYHA scale Dizziness/Falls Syncope
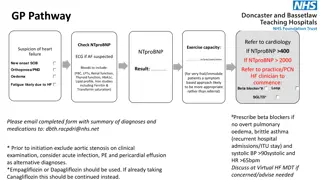
What action can you take? Blood pressure Heart Rate/ECG Pulse Oximetry Is there an Echocardiogram ? (confirmed diagnosis within 2 years to see HF team) BNP but also important to look at other causes of raised BNP (COPD, pulmonary hypertension, pneumonia, PE, CKD / AKI, hypertension, AF, diabetic, age >70 years, myocarditis, Kawasaki disease, ascitic cirrhosis, Cushing s syndrome, primary hyperaldosteronism, sepsis). Be aware that BNP level can be reduced in obesity.
Treatment Fluid overload- increase diuretics Poor Blood pressure control- treat in line with NICE guidance Low Blood pressure- split doses of prognostic medications (reduce or stop only if absolutely necessary) Poor heart rate control- treat Known LVSD Sinus Rhythm aim for 60bpm Known or new AF aim for rate around 70, >80 years of age 80bpm Anaemia treat or refer in line with guidance COPD- optimise therapies in line with guidance Renal deterioration- reduce dosage of medication- don t stop- seek advice
Who will we see? BNP 400 2000ng/L requires an echo within 6 weeks BNP> 2000ng/L requires an echo within 2 weeks Ejection Fraction <45% Ejection Fraction >50% with moderately dilated left atria and raised PASP >25mmHg Ejection Fraction 45-49% need blood pressure, heart rate and oedema management in Primary Care.
Contacts Heart Failure Team 0151 604 7711 option 2 Diane Taylor Senior Matron in Heart Failure Michelle Thomas Heart Failure Specialist Nurse Team Leader 07769782980 Linda Crosthwaite Heart Failure Specialist Nurse Andrew Booth Heart Failure Specialist Nurse Robin Lee Heart Failure Specialist Nurse Hayley Howard-Davies Heart Failure Specialist Nurse