CH 16: MENTAL HEALTH CONDITIONS
PRIMARY HEALTHCARE 2014
Updates to the 2008 PHC STG & EML
C
H
1
6
:
M
E
N
T
A
L
H
E
A
L
T
H
C
O
N
D
I
T
I
O
N
S
NATIONAL DEPARTMENT OF HEALTH
AFFORDABLE MEDICINES
ESSENTIAL MEDICINES PROGRAMME
•
Midazolam, buccal and IM
:
added
•
Lorazepam, IM:
not added (adults),
deleted (children)
•
Haloperidol, IM:
retained
•
Promethazine, IM:
retained
–
Rapid tranquilisation is not supported by robust data – to obtain study
consent in this setting where patients are disturbed is challenging.
–
Most recommendations are based on clinical experience, theoretical
considerations & research data.
–
4 TREC studies investigated parenteral medicines in “real life”
emergency settings.
Lorazepam’s efficaciousness is supported by TREC II study & is standard of care .
However, combining TREC1 and TRECII studies suggests that midazolam 7.5–15 mg
sedates
more rapidly
than lorazepam.
A limitation in TRECI: mean dose of haloperidol was lower than in other TREC studies.
2
RAPID TRANQUILISATION IN PSYCHIATRY
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Ref 1
Evidence
•
Efficacy:
–
Meta-analysis of benzodiazepines: Insufficient data to support or refute the use of
benzodiazepines (alone or in combination with antipsychotics). Analysis included
TREC studies on lorazepam & midazolam.
•
Safety:
–
Meta-analysis of benzodiazepines : Single case of side effect-respiratory depression
associated with midazolam; successfully treated with
flumazenil.
–
Respiratory depression is a class effect of benzodiazepines.
–
Flumazenil is not essential as an antidote - patient can be manually ventilated.
–
Benzodiazepines safer option as adverse effects (extrapyramidal side effects;
dystonia &
QT prolongation)
associated with antipsychotics.
3
RAPID TRANQUILISATION IN PSYCHIATRY
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Ref 2
4
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
RAPID TRANQUILISATION IN PSYCHIATRY
Pragmatic implications
•
Lorazepam is standard of care.
–
However, lorazepam requires to be refrigerated under lock & key.
–
As benzodiazepines has a class effect in this setting; a single benzodiazepine
was recommended that fulfils most indications throughout the PHC book.
•
Midazolam:
–
Recommended for status epilepticus at primary level (buccally for paediatrics &
IM for adults), supported by good quality evidence (Refer to implementation
slides for Trauma chapter).
–
Buccal midazolam observed to be efficacious in psychiatric emergency setting
for psychiatric agitation.
Ref 3
Step up approach:
•
NICE Guidelines recommends a step up approach in the short-
term management of the disturbed patient:
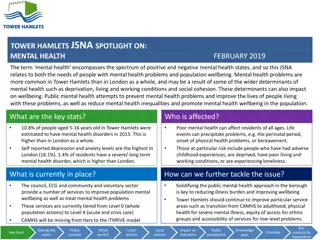
Prevalence
:
•
Patients commonly present with aggression & acute psychosis at
primary level.
5
RAPID TRANQUILISATION IN PSYCHIATRY
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
SEDATION:
Parental therapy
has little
advantage vs. oral
preparations.
Ref 4
Price
•
Lorazepam was not awarded on contract on the current or previous tender cycle.
•
Supply reported to be erratic.
•
Reference price is not available. (A market analysis showed that lorazepam does
not appear to be a reimbursable item on a number of National Healthcare Funds
[including Australia (Pharmaceutical Benefit Scheme), New Zealand (PHARMAC),
Turkey (Ex-Factory), Brazil (Maximum Price to Government]).
6
RAPID TRANQUILISATION IN PSYCHIATRY
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Listing of product prices for lorazepam, diazepam, midazolam and clonazepam Injections
7
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
RAPID TRANQUILISATION IN PSYCHIATRY
Recommendation
•
Sedation algorithm describing step up therapy:
The sedation algorithm was inserted in the following sections:
16.1 Aggressive disruptive behaviour in adults
16.6.2 Bipolar disorder
16.7.1 Acute psychosis
16.8.2 Substance-induced psychosis
ALWAYS
MONITOR
VITAL SIGNS
OF SEDATED
PATIENT
8
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
RAPID TRANQUILISATION IN PSYCHIATRY
Rationale:
•
Recent expert consensus recommends non-coercive approaches including non-
pharmacological calming techniques & oral preparations to promote patient
collaboration, when safe to do so.
•
Benzodiazepines safer option due to adverse effects (extrapyramidal side effects;
dystonia & QT prolongation) associated with antipsychotics.
•
Lorazepam requires refrigeration under lock & key.
•
Availability issues regarding lorazepam - supply erratic, locally & globally.
•
Midazolam recommended for the management of status epilepticus in adults and
paediatrics with midazolam.
Level of Evidence: II, III Systematic review of low
quality evidence, RCTs, Guidelines
(Refer to the medicine review of midazolam in rapid tranquillisation)
Ref 5
NEW STGS
9
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Rationale:
•
STGs were added to the PHC book for clarity.
•
To provide guidance on additional conditions that commonly present at primary level of care –
with referral to secondary level of care as required.
•
Midazolam:
added
•
Haloperidol
:
added
•
Orphenadrine
:
added
–
Aligned with the Paediatric Hospital level STG, 2013; SAMF 2012;
Section 16.6: Acute dystonic reactions & rationale for considering
midazolam in the PHC book (see slide # 8).
–
STG recommends switching to haloperidol, rather than administering an
additional dose of benzodiazepine - in clinical practice the side effect of
paradoxical disinhibition associated with benzodiazepines is often not
considered.
Level of Evidence: III Expert opinion, Guidelines
10
16.4.1 ACUTELY DISTURBED CHILD OR ADOLESCENT
AWAITING FURTHER EVALUATION
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Ref 6
16.5 ACUTE DYSTONIC REACTION
•
Biperiden, IM/IV:
added
•
Promethazine, IM:
added
–
STG developed to provide guidance on management of acute
dystonia.
–
Aligned with Adult Hospital level STG, 2012 & Paediatric
Hospital level STG, 2013.
–
Promethazine for use in children:
Due to global shortage of
biperiden, promethazine was considered for children
(extrapolated from adult data & dose as per sedation
indication).
11
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Ref 7
12
16.5.2 BIPOLAR DISORDER
•
Diazepam, oral:
added
•
Midazolam, buccal & IM
:
added
•
Haloperidol, IM
:
added
•
Promethazine, IM
: added
–
Aligned with the Adult Hospital level STG.
–
Sedation algorithm included in the STG.
Level of Evidence: II, III Systematic review of low
quality evidence, Guidelines
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Ref 8
2008 PHC STG: Psychosis divided into “Acute psychosis” & “Chronic psychosis”.
•
Diazepam, oral:
added
•
Haloperidol, oral:
moved to chronic psychosis STG
•
Midazolam, buccal & IM
:
added
•
Lorazepam, IM
:
deleted
•
Haloperidol, IM
:
retained
•
Promethazine, IM
: added
•
Chlorpromazine, oral:
moved to chronic psychosis STG
•
Zuclophenthixol acetate, IM:
amended
•
Fluphenazine decanoate, IM:
moved to chronic psychosis STG
•
Zuclopenthixol decanoate, IM:
moved to chronic psychosis STG
–
Aligned with the Adult Hospital level STG, 2012.
–
Sedation algorithm included in the STG.
–
Directions for use of zuclopenthixol acetate, IM amended to align with SAMF 10
th
edition, 2012.
Level of Evidence: II, III Systematic review of low quality evidence,
Guidelines
13
16.7.1 ACUTE PSYCHOSIS
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Ref 8
Schizophrenia where a less sedating agent is required
•
Haloperidol, oral:
dose amended
•
Risperidone, oral:
added
Evidence:
–
Meta-analysis: Risperidone had better overall efficacy
vs
. first-generation
antipsychotic (FGAs) medicines, −0.13 (−0.22 to −0.05, p=0.002).
–
NNT for 1 additional responder was 15 (9 to 36) for risperidone.
–
Relapse significantly better with risperidone vs. FGAs, RR 0.74 (0.63 to 0.87), NNT:
11 (7 to33).
–
Extrapyramidal side effects (EPSE) associated with risperidone vs. FGAs were less,
RR (95% CI): 0.61 (0.52 to 0.72).
–
Risperidone RCTs reviewed in the analysis were industry-sponsored. Exclusion of
these studies reduced risperidone effect size in the primary analysis (overall
symptoms) to -0.04, which was not significantly different from FGAs.
14
16.7.2 CHRONIC PSYCHOSIS
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Price:
(Refer to the costing analysis report for details, which included a
sensitivity analysis)
–
Cost effectiveness analysis compared haloperidol,
4–6 mg
to risperidone,
3–20 mg,
for schizophrenia, based on the meta-analysis by Leucht
et al
(2009).
–
Adverse effect of EPSE was costed, assuming that the percentage of patients
requiring an anticholinergic was 45.8% for haloperidol
vs
. 30.8% for risperidone
.
–
The calculated ICERs across the dose range and sensitivity analyses indicated that
risperidone was affordable (comparing haloperidol to risperidone):
15
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
16.7.2 CHRONIC PSYCHOSIS
Ref 9
Other considerations
–
Risperidone associated with more weight gain
vs.
haloperidol 1.7
(0.9 to 2.4); p < 0.0001.
–
Meta-analyses included older studies that used higher doses of FGAs
resulting in definitive EPSE. However, EPSE also associated with
second generation antipsychotics (SGAs), that is dose-dependent.
–
Tardive dyskinesia associated with antipsychotics is often diagnosed
late, & the condition is mostly irreversible.
–
The condition commonly presents at primary level, warranting
continuous availability of an agent.
16
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
16.7.2 CHRONIC PSYCHOSIS
Ref 10
Recommendations
Rationale:
•
Anticholinergics are toxic & switching from low dose FGA to SGA preferred to adding an
anticholinergic (to manage EPSE associated with FGAs).
•
Haloperidol was as efficacious as risperidone for management of chronic schizophrenia.
•
Although haloperidol is associated with a higher incidence of EPSE, risperidone is associated with a
higher incidence of weight gain and metabolic complications/syndrome.
•
Both agents are affordable & available on the current contract.
•
The condition commonly presents at primary level & warrants continuous availability of an agent.
Level of Evidence: I Meta-analysis
17
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: CENTRAL NERVOUS SYSTEM
1.
Haloperidol, oral 5 mg as first line option.
2.
If associated side-effects occur with haloperidol, switch to risperidone rather
than adding an anticholinergic.
3.
A note be included that anticholinergic therapy not be routinely added to
antipsychotics to prevent EPSE.
16.7.2 CHRONIC PSYCHOSIS
Ref 11
Schizophrenia where a more sedating agent is required:
•
Chlorpromazine
:
amended
–
Chlorpromazine 100 mg is the gold standard & reported to be more sedating
than haloperidol.
–
New patients would not be initiated on chlorpromazine at primary level of
care.
–
Those patients stabilised on chlorpromazine should continue therapy.
–
Maximum maintenance dose was amended to 800 mg daily.
Level of Evidence: III Expert opinion, Guidelines
18
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
16.7.2 CHRONIC PSYCHOSIS
Ref 12
Long-term therapy:
•
Fluphenazine decanoate
:
amended
•
Flupenthixol decanoate
:
amended
•
Zuclopenthixol decanoate
:
amended
–
Doses were aligned with the
SAMF 10
th
edition, 2012
.
–
Guidance provided on the weaning off of oral antispsychotics
when changing to a depot preparation.
–
Guidance on the addition of oral risperidone 2 mg for break
through episodes whilst on the long acting depot.
Level of Evidence: III Guidelines
19
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
16.7.2 CHRONIC PSYCHOSIS
Ref 13
Long-term therapy (cont’d):
•
Risperidone
:
added
–
Guidance provided on the addition of oral risperidone 2 mg for
break through episodes whilst on long acting depot
.
For acute dystonic reaction:
•
Biperiden, IM:
deleted
–
Text was amended with cross referral to Section 16.5 Acute
dystonic reaction.
Level of Evidence: III
Expert opinion, Guidelines
20
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
16.7.2 CHRONIC PSYCHOSIS
Ref 14
•
Scope of the primary healthcare worker:
•
Probably not in the scope of the primary healthcare
practitioner to manage substance related disorders
according to the DSM V criteria - possibly too complex.
•
However, alcohol withdrawal should be considered, as this
commonly presents at primary level of care.
Level of evidence: III Expert opinion
21
16.8 SUBSTANCE RELATED DISORDERS
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Ref 15
•
Diazepam, oral
:
added
•
Diazepam, IV
:
added
–
DSM V has combined substance abuse & substance dependent (substance-
induced) disorders under
substance use disorders
.
–
Guidelines:
The STG includes a statement to refer to National Policy guidelines
on detoxification of psychoactive substances.
–
Aligned with Adult Hospital level STG, 2012 & National Policy guidelines on
detoxification of psychoactive substances.
–
STG describes general management with benzodiazepines and referral to
secondary level.
22
16.8.1 SUBSTANCE USE DISORDERS
Level of Evidence: III Guidelines
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Ref 16
•
Diazepam, oral
:
added
•
Midazolam, buccal & IM
:
added
•
Haloperidol, IM
:
added
•
Promethazine, IM
:
added
–
Aligned with Adult Hospital level STG, 2012 & National Policy guidelines on
detoxification of psychoactive substances.
–
Sedation algorithm included in the STG.
23
16.8.2 SUBSTANCE-INDUCED PSYCHOSIS
Level of Evidence: III Guidelines
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Ref 17
•
Thiamine, oral
:
added
•
Diazepam, oral
:
added
–
Aligned with the Adult Hospital level STG, 2012.
–
However, dose of thiamine, oral was amended to 300 mg daily x 14 days.
–
As recommended
by the British Association of Psychopharmacology guidelines (2013).
–
Cochrane review: Evidence from RCTs insufficient to guide clinicians in determining the dose, frequency,
route or duration of thiamine treatment for prophylaxis against or treatment of Wernicke syndrome due to
alcohol abuse.
–
Available data of low quality: 100 mg daily is insufficient.
Level of Evidence: III Guidelines, low quality RCTs
24
16.8.4 ALCOHOL WITHDRAWAL
(UNCOMPLICATED)
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Ref 18
AMENDMENTS
25
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
•
Diazepam, oral:
added
•
Midazolam, buccal & IM
:
added
•
Haloperidol, IM
:
added
•
Promethazine, IM
: added
–
Sedation algorithm included in the STG.
–
Biperiden for acute dystonia:
Although a S21 application had been
utilised to circumvent local supply issues, there is a global shortage
of biperiden. As parenteral atropine has no supporting data in this
clinical setting; promethazine, IM, retained for acute dystonia
induced by antipsychotics.
Level of Evidence: II, III Systematic review of low
quality evidence, Guidelines
26
16.1 AGGRESSIVE DISRUPTIVE BEHAVIOUR
IN ADULTS
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Ref 19
•
Diazepam, oral
:
added
•
Citalopram, oral:
added
•
Fluoxetine, oral:
not added
–
Aligned with the Adult Hospital level STG, 2012.
–
Short course of benzodiazepines (5-10 days) considered for the
acute management of anxiety.
–
Some doctors at primary level would be able to diagnose
chronic anxiety, managed with SSRIs - SSRIs are considered
safer & less sedating than tricyclic antidepressants.
Level of Evidence: III Guidelines
27
16.2 ANXIETY AND STRESS AND RELATED
DISORDERS IN ADULTS
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Ref 20
•
Diazepam, oral
:
added
–
Aligned with the Adult Hospital level STG, 2012.
–
Short course of benzodiazepines (5-10 days) considered
for the acute management of anxiety.
Level of Evidence: III Guidelines
28
16.2 ANXIETY AND STRESS AND RELATED
DISORDERS IN ADULTS
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Ref 21
•
Fluoxetine:
not added
•
Citalopram:
added
–
Guidelines supports SSRIs as 1
st
line pharmacotherapy - chronic management of GAD in adults.
–
Paucity of robust data comparing various SSRIs for GAD. RCTs generally show comparable efficacy &
selection further guided by side effect profile of specific SSRIs.
–
1 small RCT (n=34) showed that by 8 weeks, for the treatment of anxiety disorders in the elderly (≥
60 years of age): 65% [(11/17); 95% CI 42 to 87%] in the citalopram group vs. 24% [(4/17); 95% CI 3
to 44%] the placebo group.
–
Lack of available data to support fluoxetine in preventing relapse of generalised anxiety disorders
(chronic management of anxiety).
–
RCT by Allgulander
et al
(2004):
•
Remission rate (Hamilton anxiety scale ≤ 7) higher with sertraline vs. placebo, (37% vs. 23%, p=0.006) at 12
weeks analysis & endpoint analysis with the last observation carried forward (31% vs. 18%, p=0.002).
•
Response rates (Clinical Global Impression ≤ 2) higher for sertraline (63%) vs. placebo (37%).
•
Sertraline was better tolerated
vs.
placebo.
29
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Level of Evidence: III, Guidelines, Low quality RCT
16.2 ANXIETY AND STRESS AND RELATED
DISORDERS IN ADULTS
Ref 22
•
Price
: Current contract price for citalopram cheaper than sertraline.
30
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
BASED ON
WHO/ATC
DDD (MG):
•
Sertraline: 50 mg
•
Citalopram: 20 mg
16.2 ANXIETY AND STRESS AND RELATED
DISORDERS IN ADULTS
Ref 23
16.6.1 MAJOR DEPRESSIVE DISORDER
•
Availability:
–
Fluoxetine, oral is currently only available as a 20 mg capsule on tender; and
doses of 10 mg per day would not be possible.
–
Fluoxetine & not amitryptilline considered for the elderly in this clinical setting.
31
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Level of Evidence: III Expert opinion
Ref 24
16.6.1 MAJOR DEPRESSIVE DISORDER
•
Duration of SSRI therapy:
–
The duration of 9 months appears to be consistent with the literature.
Guidelines recommend a continuation phase of therapy ranging from 6 months
to 9 months:
–
American Psychiatric Association (2010): 4 - 9 months.
–
NICE 2009: 6 months.
–
NEJM 2005: 6 - 9 months.
–
Evidence-based guidelines for treating depressive disorders with
antidepressants: a revision of the 2000 British Association for
Psychopharmacology guidelines: 6 to 9 months.
–
Texas Medication Algorithm Project 1999: 6 to 9 months.
Recommendation:
Continuation phase of SSRI therapy for a period of 6
months, once a patient has been stabilised.
Rationale:
This pragmatic approach consistent with most guidelines
.
Level of Evidence: III Guidelines
32
PRIMARY HEALTHCARE IMPLEMENTATION SLIDES
2014: MENTAL HEALTH CONDITIONS
Ref 25
PRIMARY HEALTHCARE 2014 IMPLEMENTATION
SLIDES:
RESPIRATORY
33
Which of the following can be considered as appropriate primary
health care management of chronic anxiety in an adult patient?
A.
Fluoxetine, oral, Initial dose: 20mg, increased to 40mg if there
is only a partial response after weeks. If no response after 4
weeks, refer patient to secondary level
B.
Tricyclic antidepressants, e.g. Amitriptyline, oral, at bedtime.
Initial dose: 25mg per day. Increase by 25 mg per day at 3–5
day intervals to a maximum dose of 150 mg per day.
C.
Citalopram, oral (Doctor initiated). Initiate at 10 mg daily for
the 1st week. Then increase to 20 mg daily.
CASE STUDY
PRIMARY HEALTHCARE 2014 IMPLEMENTATION
SLIDES:
RESPIRATORY
34
A.
Fluoxetine, oral, Initial dose: 20mg, increased to 40mg if there is
only a partial response after weeks. If no response after 4 weeks,
refer patient to secondary level
B.
Tricyclic antidepressants, e.g. Amitriptyline, oral, at bedtime.
Initial dose: 25mg per day. Increase by 25 mg per day at 3–5 day
intervals to a maximum dose of 150 mg per day.
C.
Citalopram, oral. Initiate at 10 mg daily for the 1st week. Then
increase to 20 mg daily.
Note:
Citalopram must be doctor initiated.
CASE STUDY: SOLUTION
PRIMARY HEALTHCARE 2014 IMPLEMENTATION
SLIDES:
RESPIRATORY
35
PRIMARY HEALTHCARE 2014 IMPLEMENTATION
SLIDES:
RESPIRATORY
36
37
PRIMARY HEALTHCARE 2014 IMPLEMENTATION
SLIDES:
RESPIRATORY
38
39
40
41
PRIMARY HEALTHCARE 2014 IMPLEMENTATION
SLIDES:
RESPIRATORY
42
PRIMARY HEALTHCARE 2014 IMPLEMENTATION
SLIDES:
RESPIRATORY
43
PRIMARY HEALTHCARE 2014 IMPLEMENTATION
SLIDES:
RESPIRATORY
44
44
45
46
PRIMARY HEALTHCARE 2014 IMPLEMENTATION
SLIDES:
RESPIRATORY
47
48
PRIMARY HEALTHCARE 2014 IMPLEMENTATION
SLIDES:
RESPIRATORY
49
DISCLAIMER
This slide set is an implementation tool and should be used alongside the published STG. This information does not supersede or replace the STG itself.
Rapid tranquilisation in psychiatry involves the use of benzodiazepines and antipsychotics for managing disturbed patients. This overview discusses the efficacy, safety, and pragmatic implications of using medications like midazolam and lorazepam, along with recommended step-up approaches for short-term management.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
CH 16: MENTAL HEALTH CONDITIONS NATIONAL DEPARTMENT OF HEALTH AFFORDABLE MEDICINES ESSENTIAL MEDICINES PROGRAMME PRIMARY HEALTHCARE 2014 Updates to the 2008 PHC STG & EML
RAPID TRANQUILISATION IN PSYCHIATRY Midazolam, buccal and IM: added Lorazepam, IM: not added (adults), deleted (children) Haloperidol, IM: retained Promethazine, IM: retained Rapid tranquilisation is not supported by robust data to obtain study consent in this setting where patients are disturbed is challenging. Most recommendations are based on clinical experience, theoretical considerations & research data. 4 TREC studies investigated parenteral medicines in real life emergency settings. Lorazepam s efficaciousness is supported by TREC II study & is standard of care . However, combining TREC1 and TRECII studies suggests that midazolam 7.5 15 mg sedates more rapidly than lorazepam. A limitation in TRECI: mean dose of haloperidol was lower than in other TREC studies. Ref 1 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 2
RAPID TRANQUILISATION IN PSYCHIATRY Evidence Efficacy: Meta-analysis of benzodiazepines: Insufficient data to support or refute the use of benzodiazepines (alone or in combination with antipsychotics). Analysis included TREC studies on lorazepam & midazolam. Safety: Meta-analysis of benzodiazepines : Single case of side effect-respiratory depression associated with midazolam; successfully treated with flumazenil. Respiratory depression is a class effect of benzodiazepines. Flumazenil is not essential as an antidote - patient can be manually ventilated. Benzodiazepines safer option as adverse effects (extrapyramidal side effects; dystonia & QT prolongation) associated with antipsychotics. Ref 2 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 3
RAPID TRANQUILISATION IN PSYCHIATRY Pragmatic implications Lorazepam is standard of care. However, lorazepam requires to be refrigerated under lock & key. As benzodiazepines has a class effect in this setting; a single benzodiazepine was recommended that fulfils most indications throughout the PHC book. Midazolam: Recommended for status epilepticus at primary level (buccally for paediatrics & IM for adults), supported by good quality evidence (Refer to implementation slides for Trauma chapter). Buccal midazolam observed to be efficacious in psychiatric emergency setting for psychiatric agitation. Ref 3 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 4
RAPID TRANQUILISATION IN PSYCHIATRY Step up approach: NICE Guidelines recommends a step up approach in the short- term management of the disturbed patient: Non-pharmacological techniques of de-escalation. Oral therapy Parenteral therapy Prevalence: Patients commonly present with aggression & acute psychosis at primary level. Ref 4 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 5
RAPID TRANQUILISATION IN PSYCHIATRY Price Lorazepam was not awarded on contract on the current or previous tender cycle. Supply reported to be erratic. Reference price is not available. (A market analysis showed that lorazepam does not appear to be a reimbursable item on a number of National Healthcare Funds [including Australia (Pharmaceutical Benefit Scheme), New Zealand (PHARMAC), Turkey (Ex-Factory), Brazil (Maximum Price to Government]). Listing of product prices for lorazepam, diazepam, midazolam and clonazepam Injections PRICE SOURCE Australia PBS New Zealand Turkey Brazil MSH price guide LORAZEPAM INJ DIAZEPAM INJ Not listed Not listed Not listed Not listed Not listed MIDAZOLAM INJ Not listed 1mg/ml Not listed 5mg/ml, 1mg/ml, 2mg/ml 1mg/ml, 5mg/ml 10mg/2ml 10mg/2ml Not listed 5mg/ml , 10mg/ml Not listed PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 6
RAPID TRANQUILISATION IN PSYCHIATRY Recommendation Sedation algorithm describing step up therapy: Non-pharmacological techniques of de-escalation. Benzodiazepines (e.g. midazolam) Oral therapy initially ; then IM therapy if oral route not possible or failed. Psychotics (haloperidol with promethazine) once diagnosis made. The sedation algorithm was inserted in the following sections: 16.1 Aggressive disruptive behaviour in adults 16.6.2 Bipolar disorder 16.7.1 Acute psychosis 16.8.2 Substance-induced psychosis PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 7
RAPID TRANQUILISATION IN PSYCHIATRY Rationale: Recent expert consensus recommends non-coercive approaches including non- pharmacological calming techniques & oral preparations to promote patient collaboration, when safe to do so. Benzodiazepines safer option due to adverse effects (extrapyramidal side effects; dystonia & QT prolongation) associated with antipsychotics. Lorazepam requires refrigeration under lock & key. Availability issues regarding lorazepam - supply erratic, locally & globally. Midazolam recommended for the management of status epilepticus in adults and paediatrics with midazolam. Level of Evidence: II, III Systematic review of low quality evidence, RCTs, Guidelines (Refer to the medicine review of midazolam in rapid tranquillisation) Ref 5 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 8
NEW STGS Rationale: STGs were added to the PHC book for clarity. To provide guidance on additional conditions that commonly present at primary level of care with referral to secondary level of care as required. SECTION CONDITION MEDICINE MANAGEMENT 16.4.1 ACUTELY DISTURBED CHILD OR ADOLESCENT AWAITING PSYCHIATRIC EVALUATION ACUTE DYSTONIC REACTION SUICIDE RISK ASSESMENT BIPOLAR DISORDER ACUTE PSYCHOSIS CHRONIC PSYCHOSIS SUBSTANCE USE DISORDERS SUBSTANCE-INDUCED MOOD DISORDER SUBSTANCE-INDUCED PSYCHOSIS Yes 16.5 16.6.1.1 16.6.2 16.7.1 16.7.2 16.8.1 16.8.2 16.8.3 Yes No referral Yes Yes Yes Yes Yes Yes 16.8.4 ALCOHOL WITHDRAWAL (UNCOMPLICATED) Yes PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 9
16.4.1 ACUTELY DISTURBED CHILD OR ADOLESCENT AWAITING FURTHER EVALUATION Midazolam: added Haloperidol: added Orphenadrine: added Aligned with the Paediatric Hospital level STG, 2013; SAMF 2012; Section 16.6: Acute dystonic reactions & rationale for considering midazolam in the PHC book (see slide # 8). STG recommends switching to haloperidol, rather than administering an additional dose of benzodiazepine - in clinical practice the side effect of paradoxical disinhibition associated with benzodiazepines is often not considered. Level of Evidence: III Expert opinion, Guidelines Ref 6 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 10
16.5 ACUTE DYSTONIC REACTION Biperiden, IM/IV: added Promethazine, IM: added STG developed to provide guidance on management of acute dystonia. Aligned with Adult Hospital level STG, 2012 & Paediatric Hospital level STG, 2013. Promethazine for use in children: Due to global shortage of biperiden, promethazine was considered for children (extrapolated from adult data & dose as per sedation indication). Ref 7 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 11
16.5.2 BIPOLAR DISORDER Diazepam, oral: added Midazolam, buccal & IM: added Haloperidol, IM: added Promethazine, IM: added Aligned with the Adult Hospital level STG. Sedation algorithm included in the STG. Level of Evidence: II, III Systematic review of low quality evidence, Guidelines Ref 8 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 12
16.7.1 ACUTE PSYCHOSIS 2008 PHC STG: Psychosis divided into Acute psychosis & Chronic psychosis . Diazepam, oral: added Haloperidol, oral: moved to chronic psychosis STG Midazolam, buccal & IM: added Lorazepam, IM: deleted Haloperidol, IM: retained Promethazine, IM: added Chlorpromazine, oral: moved to chronic psychosis STG Zuclophenthixol acetate, IM: amended Fluphenazine decanoate, IM: moved to chronic psychosis STG Zuclopenthixol decanoate, IM: moved to chronic psychosis STG Aligned with the Adult Hospital level STG, 2012. Sedation algorithm included in the STG. Directions for use of zuclopenthixol acetate, IM amended to align with SAMF 10th edition, 2012. Level of Evidence: II, III Systematic review of low quality evidence, Guidelines Ref 8 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 13
16.7.2 CHRONIC PSYCHOSIS Schizophrenia where a less sedating agent is required Haloperidol, oral: dose amended Risperidone, oral: added Evidence: Meta-analysis: Risperidone had better overall efficacy vs. first-generation antipsychotic (FGAs) medicines, 0.13 ( 0.22 to 0.05, p=0.002). NNT for 1 additional responder was 15 (9 to 36) for risperidone. Relapse significantly better with risperidone vs. FGAs, RR 0.74 (0.63 to 0.87), NNT: 11 (7 to33). Extrapyramidal side effects (EPSE) associated with risperidone vs. FGAs were less, RR (95% CI): 0.61 (0.52 to 0.72). Risperidone RCTs reviewed in the analysis were industry-sponsored. Exclusion of these studies reduced risperidone effect size in the primary analysis (overall symptoms) to -0.04, which was not significantly different from FGAs. PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 14
16.7.2 CHRONIC PSYCHOSIS Price:(Refer to the costing analysis report for details, which included a sensitivity analysis) Cost effectiveness analysis compared haloperidol, 4 6 mg to risperidone, 3 20 mg, for schizophrenia, based on the meta-analysis by Leucht et al (2009). Adverse effect of EPSE was costed, assuming that the percentage of patients requiring an anticholinergic was 45.8% for haloperidol vs. 30.8% for risperidone. The calculated ICERs across the dose range and sensitivity analyses indicated that risperidone was affordable (comparing haloperidol to risperidone): Effect i. Overall efficacy ii. One additional responder iii. Relapse improved - R11.88 to R161.74 ICER R8.64 to R117.63 -R16.20 to -R220.56 Sensitivity analysis (lower limit) Sensitivity analysis (upper limit) R5.40 to R73.52 -R9.72 to R132.33 R21.60 to R294.07 -R38.89 to R529.33 -R7.56 to R102.93 -R35.65 to R485.22 Ref 9 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 15
16.7.2 CHRONIC PSYCHOSIS Other considerations Risperidone associated with more weight gain vs. haloperidol 1.7 (0.9 to 2.4); p < 0.0001. Meta-analyses included older studies that used higher doses of FGAs resulting in definitive EPSE. However, EPSE also associated with second generation antipsychotics (SGAs), that is dose-dependent. Tardive dyskinesia associated with antipsychotics is often diagnosed late, & the condition is mostly irreversible. The condition commonly presents at primary level, warranting continuous availability of an agent. Ref 10 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 16
16.7.2 CHRONIC PSYCHOSIS Recommendations 1. 2. Haloperidol, oral 5 mg as first line option. If associated side-effects occur with haloperidol, switch to risperidone rather than adding an anticholinergic. A note be included that anticholinergic therapy not be routinely added to antipsychotics to prevent EPSE. 3. Rationale: Anticholinergics are toxic & switching from low dose FGA to SGA preferred to adding an anticholinergic (to manage EPSE associated with FGAs). Haloperidol was as efficacious as risperidone for management of chronic schizophrenia. Although haloperidol is associated with a higher incidence of EPSE, risperidone is associated with a higher incidence of weight gain and metabolic complications/syndrome. Both agents are affordable & available on the current contract. The condition commonly presents at primary level & warrants continuous availability of an agent. Level of Evidence: I Meta-analysis Ref 11 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: CENTRAL NERVOUS SYSTEM 17
16.7.2 CHRONIC PSYCHOSIS Schizophrenia where a more sedating agent is required: Chlorpromazine: amended Chlorpromazine 100 mg is the gold standard & reported to be more sedating than haloperidol. New patients would not be initiated on chlorpromazine at primary level of care. Those patients stabilised on chlorpromazine should continue therapy. Maximum maintenance dose was amended to 800 mg daily. Level of Evidence: III Expert opinion, Guidelines Ref 12 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 18
16.7.2 CHRONIC PSYCHOSIS Long-term therapy: Fluphenazine decanoate: amended Flupenthixol decanoate: amended Zuclopenthixol decanoate: amended Doses were aligned with the SAMF 10th edition, 2012. Guidance provided on the weaning off of oral antispsychotics when changing to a depot preparation. Guidance on the addition of oral risperidone 2 mg for break through episodes whilst on the long acting depot. Ref 13 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 19 Level of Evidence: III Guidelines
16.7.2 CHRONIC PSYCHOSIS Long-term therapy (cont d): Risperidone: added Guidance provided on the addition of oral risperidone 2 mg for break through episodes whilst on long acting depot. For acute dystonic reaction: Biperiden, IM: deleted Text was amended with cross referral to Section 16.5 Acute dystonic reaction. Level of Evidence: III Expert opinion, Guidelines Ref 14 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 20
16.8 SUBSTANCE RELATED DISORDERS Scope of the primary healthcare worker: Probably not in the scope of the primary healthcare practitioner to manage substance related disorders according to the DSM V criteria - possibly too complex. However, alcohol withdrawal should be considered, as this commonly presents at primary level of care. Level of evidence: III Expert opinion Ref 15 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 21
16.8.1 SUBSTANCE USE DISORDERS Diazepam, oral: added Diazepam, IV: added DSM V has combined substance abuse & substance dependent (substance- induced) disorders under substance use disorders. Guidelines: The STG includes a statement to refer to National Policy guidelines on detoxification of psychoactive substances. Aligned with Adult Hospital level STG, 2012 & National Policy guidelines on detoxification of psychoactive substances. STG describes general management with benzodiazepines and referral to secondary level. Level of Evidence: III Guidelines Ref 16 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 22
16.8.2 SUBSTANCE-INDUCED PSYCHOSIS Diazepam, oral: added Midazolam, buccal & IM: added Haloperidol, IM: added Promethazine, IM: added Aligned with Adult Hospital level STG, 2012 & National Policy guidelines on detoxification of psychoactive substances. Sedation algorithm included in the STG. Level of Evidence: III Guidelines Ref 17 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 23
16.8.4 ALCOHOL WITHDRAWAL (UNCOMPLICATED) Thiamine, oral: added Diazepam, oral: added Aligned with the Adult Hospital level STG, 2012. However, dose of thiamine, oral was amended to 300 mg daily x 14 days. As recommended by the British Association of Psychopharmacology guidelines (2013). Cochrane review: Evidence from RCTs insufficient to guide clinicians in determining the dose, frequency, route or duration of thiamine treatment for prophylaxis against or treatment of Wernicke syndrome due to alcohol abuse. Available data of low quality: 100 mg daily is insufficient. Level of Evidence: III Guidelines, low quality RCTs Ref 18 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 24
AMENDMENTS PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 25
16.1 AGGRESSIVE DISRUPTIVE BEHAVIOUR IN ADULTS Diazepam, oral: added Midazolam, buccal & IM: added Haloperidol, IM: added Promethazine, IM: added Sedation algorithm included in the STG. Biperiden for acute dystonia: Although a S21 application had been utilised to circumvent local supply issues, there is a global shortage of biperiden. As parenteral atropine has no supporting data in this clinical setting; promethazine, IM, retained for acute dystonia induced by antipsychotics. Level of Evidence: II, III Systematic review of low quality evidence, Guidelines Ref 19 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 26
16.2 ANXIETY AND STRESS AND RELATED DISORDERS IN ADULTS Diazepam, oral: added Citalopram, oral: added Fluoxetine, oral: not added Aligned with the Adult Hospital level STG, 2012. Short course of benzodiazepines (5-10 days) considered for the acute management of anxiety. Some doctors at primary level would be able to diagnose chronic anxiety, managed with SSRIs - SSRIs are considered safer & less sedating than tricyclic antidepressants. Level of Evidence: III Guidelines Ref 20 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 27
16.2 ANXIETY AND STRESS AND RELATED DISORDERS IN ADULTS Diazepam, oral: added Aligned with the Adult Hospital level STG, 2012. Short course of benzodiazepines (5-10 days) considered for the acute management of anxiety. Level of Evidence: III Guidelines Ref 21 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 28
16.2 ANXIETY AND STRESS AND RELATED DISORDERS IN ADULTS Fluoxetine: not added Citalopram: added Guidelines supports SSRIs as 1st line pharmacotherapy - chronic management of GAD in adults. Paucity of robust data comparing various SSRIs for GAD. RCTs generally show comparable efficacy & selection further guided by side effect profile of specific SSRIs. 1 small RCT (n=34) showed that by 8 weeks, for the treatment of anxiety disorders in the elderly ( 60 years of age): 65% [(11/17); 95% CI 42 to 87%] in the citalopram group vs. 24% [(4/17); 95% CI 3 to 44%] the placebo group. Lack of available data to support fluoxetine in preventing relapse of generalised anxiety disorders (chronic management of anxiety). RCT by Allgulander et al (2004): Remission rate (Hamilton anxiety scale 7) higher with sertraline vs. placebo, (37% vs. 23%, p=0.006) at 12 weeks analysis & endpoint analysis with the last observation carried forward (31% vs. 18%, p=0.002). Response rates (Clinical Global Impression 2) higher for sertraline (63%) vs. placebo (37%). Sertraline was better tolerated vs. placebo. Level of Evidence: III, Guidelines, Low quality RCT Ref 22 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 29
16.2 ANXIETY AND STRESS AND RELATED DISORDERS IN ADULTS Price: Current contract price for citalopram cheaper than sertraline. Comparative costs for 30 days supply R10.00 R8.00 BASED ON WHO/ATC DDD (MG): Sertraline: 50 mg Citalopram: 20 mg Sertraline 50 mg R6.00 R4.00 Citalopram 20 mg R2.00 R- Ref 23 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 30
16.6.1 MAJOR DEPRESSIVE DISORDER Availability: Fluoxetine, oral is currently only available as a 20 mg capsule on tender; and doses of 10 mg per day would not be possible. Fluoxetine & not amitryptilline considered for the elderly in this clinical setting. Level of Evidence: III Expert opinion Ref 24 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 31
16.6.1 MAJOR DEPRESSIVE DISORDER Duration of SSRI therapy: The duration of 9 months appears to be consistent with the literature. Guidelines recommend a continuation phase of therapy ranging from 6 months to 9 months: American Psychiatric Association (2010): 4 - 9 months. NICE 2009: 6 months. NEJM 2005: 6 - 9 months. Evidence-based guidelines for treating depressive disorders with antidepressants: a revision of the 2000 British Association for Psychopharmacology guidelines: 6 to 9 months. Texas Medication Algorithm Project 1999: 6 to 9 months. Recommendation: Continuation phase of SSRI therapy for a period of 6 months, once a patient has been stabilised. Rationale:This pragmatic approach consistent with most guidelines. Level of Evidence: III Guidelines PRIMARY HEALTHCARE 2014 IMPLEMENTATION SLIDES: RESPIRATORY Ref 25 PRIMARY HEALTHCARE IMPLEMENTATION SLIDES 2014: MENTAL HEALTH CONDITIONS 32
CASE STUDY Which of the following can be considered as appropriate primary health care management of chronic anxiety in an adult patient? A. Fluoxetine, oral, Initial dose: 20mg, increased to 40mg if there is only a partial response after weeks. If no response after 4 weeks, refer patient to secondary level B. Tricyclic antidepressants, e.g. Amitriptyline, oral, at bedtime. Initial dose: 25mg per day. Increase by 25 mg per day at 3 5 day intervals to a maximum dose of 150 mg per day. C. Citalopram, oral (Doctor initiated). Initiate at 10 mg daily for the 1st week. Then increase to 20 mg daily. PRIMARY HEALTHCARE 2014 IMPLEMENTATION SLIDES: RESPIRATORY 33
CASE STUDY: SOLUTION A. Fluoxetine, oral, Initial dose: 20mg, increased to 40mg if there is only a partial response after weeks. If no response after 4 weeks, refer patient to secondary level B. Tricyclic antidepressants, e.g. Amitriptyline, oral, at bedtime. Initial dose: 25mg per day. Increase by 25 mg per day at 3 5 day intervals to a maximum dose of 150 mg per day. C. Citalopram, oral. Initiate at 10 mg daily for the 1st week. Then increase to 20 mg daily. Note: Citalopram must be doctor initiated. PRIMARY HEALTHCARE 2014 IMPLEMENTATION SLIDES: RESPIRATORY 34
Slide Ref # Reference RAPID TRANQUILISATION IN PSYCHIATRY TREC I: TREC Collaborative Group. Rapid tranquillisation for agitated patients in emergency psychiatric rooms: a randomised trial of midazolam versus haloperidol plus promethazine. BMJ. 2003 Sep 27;327(7417):708-13. http://www.ncbi.nlm.nih.gov/pubmed/14512476 TREC II: Alexander J, Tharyan P, Adams C, John T, Mol C, Philip J. Rapid tranquillisation of violent or agitated patients in a psychiatric emergencysetting. Pragmatic randomised trial of intramuscular lorazepam v. haloperidol plus promethazine. Br J Psychiatry. 2004 Jul;185:63-9. http://www.ncbi.nlm.nih.gov/pubmed/15231557 TREC III: Huf G, Coutinho ES, Adams CE; TREC Collaborative Group. Rapid tranquillisationin psychiatric emergency settings in Brazil: pragmatic randomisedcontrolledtrial of intramuscular haloperidol versus intramuscular haloperidol plus promethazine. BMJ. 2007 Oct 27;335(7625):869. http://www.ncbi.nlm.nih.gov/pubmed/17954515 TREC IV: Raveendran NS, Tharyan P, Alexander J, Adams CE; TREC-India II Collaborative Group. Rapid tranquillisation in psychiatric emergency settings in India: pragmatic randomised controlled trial of intramuscular olanzapine versus intramuscular haloperidol plus promethazine. BMJ. 2007 Oct 27;335(7625):865. http://www.ncbi.nlm.nih.gov/pubmed/17954514 2 1 Gillies D, Sampson S, Beck A, Rathbone J. Benzodiazepines for psychosis-induced aggression or agitation. Cochrane Database Syst Rev. 2013 Apr 30;4:CD003079. http://www.ncbi.nlm.nih.gov/pubmed/23633309 Alexander J, Tharyan P, Adams C, John T, Mol C, Philip J. Rapid tranquillisation of violent or agitated patients in a psychiatric emergency setting. Pragmatic randomised trial of intramuscular lorazepam v. haloperidol plus promethazine. Br J Psychiatry. 2004 Jul;185:63-9. TREC Collaborative Group. Rapid tranquillisation for agitated patients in emergency psychiatric rooms: a randomised trial of midazolam versus haloperidol plus promethazine. BMJ. 2003 Sep 27;327(7417):708-13. SAMF 2012, 10th edition. 3 2 4 3 MIDAZOLAM Taylor D, Okocha C, Paton C, Smith S, Connolly A. Buccal midazolam for agitation on psychiatric intensive care wards. Int J Psychiatry ClinPract.2008;12(4):309-11. http://www.ncbi.nlm.nih.gov/pubmed/24937720 Taylor D, Okocha C, Paton C, Smith S, Connolly A. Buccal midazolam for agitation on psychiatric intensive care wards. Int J Psychiatry ClinPract.2008;12(4):309-11. http://www.ncbi.nlm.nih.gov/pubmed/24937720 5 4 PRIMARY HEALTHCARE 2014 IMPLEMENTATION SLIDES: RESPIRATORY 35
Slide Ref # Reference RAPID TRANQUILISATION IN PSYCHIATRY Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012 Feb;13(1):26-34. http://www.ncbi.nlm.nih.gov/pubmed/22461918 NICE. The short-term management of disturbed/violent behaviour in in-patient psychiatric settings and emergency departments, NICE clinical guideline 25, February 2005. Available at: www.nice.org.uk/cg25 8 5 16.4 MENTAL HEALTH CONDITIONS IN CHILDREN AND ADOLESCENTS 10 6 MIDAZOLAM Paediatric Hospital level STG, 2013. SAMF 10th edition, 2012. Section 16.6: Acute dystonic reactions 10 6 HALOPERIDOL Paediatric Hospital level STG, 2013. SAMF 10th edition, 2012. Section 16.6: Acute dystonic reactions 10 6 ORPHENADRINE Paediatric Hospital level STG, 2013. SAMF 10th edition, 2012. Section 16.6: Acute dystonic reactions 16.5 ACUTE DYSTONIC REACTION 11 7 BIPERIDEN Adult Hospital level STG ,2012. Paediatric Hospital level STG, 2013. SAMF 10th edition, 2012. 11 7 PROMETHAZINE Adult Hospital level STG ,2012. Paediatric Hospital level STG, 2013. SAMF 10th edition, 2012. 36
Slide Ref # Reference 16.7.1 ACUTE PSYCHOSIS 13 8 DIAZEPAM Gillies D, Sampson S, Beck A, Rathbone J. Benzodiazepines for psychosis-induced aggression or agitation. Cochrane Database Syst Rev. 2013 Apr 30;4:CD003079. NICE clinical guideline 25: The short-term management of disturbed/violent behaviour in in-patient psychiatric settings and emergency departments. Leucht S, Heres S, Kissling W, Davis JM.Evidence-based pharmacotherapy of schizophrenia.Int J Neuropsychopharmacol. 2011 Mar;14(2):269-84. Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012 Feb;13(1):26-34. Adult Hospital level STG, 2012. 13 8 MIDAZOLAM Gillies D, Sampson S, Beck A, Rathbone J. Benzodiazepines for psychosis-induced aggression or agitation. Cochrane Database Syst Rev. 2013 Apr 30;4:CD003079. TREC I: TREC Collaborative Group. Rapid tranquillisation for agitated patients in emergency psychiatric rooms: a randomised trial of midazolam versus haloperidol plus promethazine. BMJ. 2003 Sep 27;327(7417):708-13. TREC II: Alexander J, Tharyan P, Adams C, John T, Mol C, Philip J. Rapidtranquillisation of violent or agitated patients in a psychiatric emergencysetting. Pragmatic randomised trial of intramuscular lorazepam v. haloperidol plus promethazine. Br J Psychiatry. 2004 Jul;185:63-9. TREC III: Huf G, Coutinho ES, Adams CE; TREC Collaborative Group. Rapid tranquillisationin psychiatric emergency settings in Brazil: pragmatic randomisedcontrolledtrial of intramuscular haloperidol versus intramuscular haloperidol pluspromethazine. BMJ. 2007 Oct 27;335(7625):869. NICE clinical guideline 25: The short-term management of disturbed/violent behaviour in in-patient psychiatric settings and emergency departments. Leucht S, Heres S, Kissling W, Davis JM.Evidence-based pharmacotherapy of schizophrenia.Int J Neuropsychopharmacol. 2011 Mar;14(2):269-84. Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012 Feb;13(1):26-34. Adult Hospital level STG, 2012. PRIMARY HEALTHCARE 2014 IMPLEMENTATION SLIDES: RESPIRATORY 37
Slide Ref # Reference 16.7.1 ACUTE PSYCHOSIS 13 8 LORAZEPAM Gillies D, Sampson S, Beck A, Rathbone J. Benzodiazepines for psychosis-induced aggression or agitation. Cochrane Database Syst Rev. 2013 Apr 30;4:CD003079. NICE clinical guideline 25: The short-term management of disturbed/violent behaviour in in-patient psychiatric settings and emergency departments. Leucht S, Heres S, Kissling W, Davis JM.Evidence-based pharmacotherapy of schizophrenia.Int J Neuropsychopharmacol. 2011 Mar;14(2):269-84. Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012 Feb;13(1):26-34. Adult Hospital level STG, 2012. 16.7.2 CHRONIC PSYCHOSIS 13 8 HALOPERIDOL Gillies D, Sampson S, Beck A, Rathbone J. Benzodiazepines for psychosis-induced aggression or agitation. Cochrane Database Syst Rev. 2013 Apr 30;4:CD003079. TREC I: TREC Collaborative Group. Rapid tranquillisation for agitated patients in emergency psychiatric rooms: a randomised trial of midazolam versus haloperidol plus promethazine. BMJ. 2003 Sep 27;327(7417):708-13. TREC II: Alexander J, Tharyan P, Adams C, John T, Mol C, Philip J. Rapidtranquillisation of violent or agitated patients in a psychiatric emergencysetting. Pragmatic randomised trial of intramuscular lorazepam v. haloperidol plus promethazine. Br J Psychiatry. 2004 Jul;185:63-9. TREC III: Huf G, Coutinho ES, Adams CE; TREC Collaborative Group. Rapid tranquillisationin psychiatric emergency settings in Brazil: pragmatic randomisedcontrolledtrial of intramuscular haloperidol versus intramuscular haloperidol pluspromethazine. BMJ. 2007 Oct 27;335(7625):869. NICE clinical guideline 25: The short-term management of disturbed/violent behaviour in in-patient psychiatric settings and emergency departments. Leucht S, Heres S, Kissling W, Davis JM.Evidence-based pharmacotherapy of schizophrenia.Int J Neuropsychopharmacol. 2011 Mar;14(2):269-84. Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012 Feb;13(1):26-34. Adult Hospital level STG, 2012. 38
Slide Ref # Reference 16.7.1 ACUTE PSYCHOSIS 13 8 PROMETHAZINE Gillies D, Sampson S, Beck A, Rathbone J. Benzodiazepines for psychosis-induced aggression or agitation. Cochrane Database Syst Rev. 2013 Apr 30;4:CD003079. TREC I: TREC Collaborative Group. Rapid tranquillisation for agitated patients in emergency psychiatric rooms: a randomised trial of midazolam versus haloperidol plus promethazine. BMJ. 2003 Sep 27;327(7417):708-13. TREC II: Alexander J, Tharyan P, Adams C, John T, Mol C, Philip J. Rapidtranquillisation of violent or agitated patients in a psychiatric emergencysetting. Pragmatic randomised trial of intramuscular lorazepam v. haloperidol plus promethazine. Br J Psychiatry. 2004 Jul;185:63-9. TREC III: Huf G, Coutinho ES, Adams CE; TREC Collaborative Group. Rapid tranquillisationin psychiatric emergency settings in Brazil: pragmatic randomisedcontrolledtrial of intramuscular haloperidol versus intramuscular haloperidol pluspromethazine. BMJ. 2007 Oct 27;335(7625):869. NICE clinical guideline 25: The short-term management of disturbed/violent behaviour in in-patient psychiatric settings and emergency departments. Leucht S, Heres S, Kissling W, Davis JM.Evidence-based pharmacotherapy of schizophrenia.Int J Neuropsychopharmacol. 2011 Mar;14(2):269-84. Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012 Feb;13(1):26-34. Adult Hospital level STG, 2012. 13 8 ZUCLOPHENTHIXOL ACETATE Gillies D, Sampson S, Beck A, Rathbone J. Benzodiazepines for psychosis-induced aggression or agitation. Cochrane Database Syst Rev. 2013 Apr 30;4:CD003079. NICE clinical guideline 25: The short-term management of disturbed/violent behaviour in in-patient psychiatric settings and emergency departments. Leucht S, Heres S, Kissling W, Davis JM.Evidence-based pharmacotherapy of schizophrenia.Int J Neuropsychopharmacol. 2011 Mar;14(2):269-84. Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012 Feb;13(1):26-34. Adult Hospital level STG, 2012. 39
Slide Ref # Reference 16.7.2 CHRONIC PSYCHOSIS 13 8 CHLORPROMAZINE Gillies D, Sampson S, Beck A, Rathbone J. Benzodiazepines for psychosis-induced aggression or agitation. Cochrane Database Syst Rev. 2013 Apr 30;4:CD003079. NICE clinical guideline 25: The short-term management of disturbed/violent behaviour in in-patient psychiatric settings and emergency departments. Leucht S, Heres S, Kissling W, Davis JM.Evidence-based pharmacotherapy of schizophrenia.Int J Neuropsychopharmacol. 2011 Mar;14(2):269-84. Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012 Feb;13(1):26-34. Adult Hospital level STG, 2012. 13 8 ZUCLOPHENTHIXOL DECONATE Gillies D, Sampson S, Beck A, Rathbone J. Benzodiazepines for psychosis-induced aggression or agitation. Cochrane Database Syst Rev. 2013 Apr 30;4:CD003079. NICE clinical guideline 25: The short-term management of disturbed/violent behaviour in in-patient psychiatric settings and emergency departments. Leucht S, Heres S, Kissling W, Davis JM.Evidence-based pharmacotherapy of schizophrenia.Int J Neuropsychopharmacol. 2011 Mar;14(2):269-84. Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012 Feb;13(1):26-34. Adult Hospital level STG, 2012. 13 8 FLUPHENAZINE DECANOATE Gillies D, Sampson S, Beck A, Rathbone J. Benzodiazepines for psychosis-induced aggression or agitation. Cochrane Database Syst Rev. 2013 Apr 30;4:CD003079. NICE clinical guideline 25: The short-term management of disturbed/violent behaviour in in-patient psychiatric settings and emergency departments. Leucht S, Heres S, Kissling W, Davis JM.Evidence-based pharmacotherapy of schizophrenia.Int J Neuropsychopharmacol. 2011 Mar;14(2):269-84. Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012 Feb;13(1):26-34. Adult Hospital level STG, 2012. 40
Slide Ref # Reference 16.7.2 CHRONIC PSYCHOSIS Gillies D, Sampson S, Beck A, Rathbone J. Benzodiazepines for psychosis-induced aggression or agitation. Cochrane Database Syst Rev. 2013 Apr 30;4:CD003079. TREC I: TREC Collaborative Group. Rapid tranquillisation for agitated patients in emergency psychiatric rooms: a randomised trial of midazolam versus haloperidol plus promethazine. BMJ. 2003 Sep 27;327(7417):708-13. TREC II: Alexander J, Tharyan P, Adams C, John T, Mol C, Philip J. Rapid tranquillisation of violent or agitated patients in a psychiatric emergencysetting. Pragmatic randomised trial of intramuscular lorazepam v. haloperidol plus promethazine. Br J Psychiatry. 2004 Jul;185:63-9. Promethazine, IM: Huf G, Coutinho ES, Adams CE; TREC Collaborative Group. Rapid tranquillisationin psychiatric emergency settings in Brazil: pragmatic randomisedcontrolledtrial of intramuscular haloperidol versus intramuscular haloperidol plus promethazine. BMJ. 2007 Oct 27;335(7625):869. http://www.ncbi.nlm.nih.gov/pubmed/17954515 NICE clinical guideline 25: The short-term management of disturbed/violent behaviour in in-patient psychiatric settings and emergency departments. Leucht S, Heres S, Kissling W, Davis JM.Evidence-based pharmacotherapy of schizophrenia.Int J Neuropsychopharmacol. 2011 Mar;14(2):269-84. Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012 Feb;13(1):26-34. Adult Hospital level STG, 2012. SAMF 10th edition, 2012. 15 9 Leucht S, Corves C, Arbter D, Engel RR, Li C, Davis JM. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet. 2009 Jan 3;373(9657):31-41. http://www.ncbi.nlm.nih.gov/pubmed/19058842 Crespo-Facorro B, P rez-Iglesias R, Mata I, Ramirez-Bonilla M, Mart nez-Garcia O, Pardo-Garcia G, Caseiro O, Pelayo- Ter n JM, V zquez-Barquero JL. Effectiveness of haloperidol, risperidone and olanzapine in the treatment of first- episode non-affective psychosis: results of a randomized, flexible-dose, open-label 1-year follow-up comparison. J Psychopharmacol. 2011 Jun;25(6):744-54. http://www.ncbi.nlm.nih.gov/pubmed/21292922 16 10 Leucht S, Corves C, Arbter D, Engel RR, Li C, Davis JM. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet. 2009 Jan 3;373(9657):31-41. http://www.ncbi.nlm.nih.gov/pubmed/19058842 16 10 Leucht S, Corves C, Arbter D, Engel RR, Li C, Davis JM. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet. 2009 Jan 3;373(9657):31-41. http://www.ncbi.nlm.nih.gov/pubmed/19058842 PRIMARY HEALTHCARE 2014 IMPLEMENTATION SLIDES: RESPIRATORY 17 11 41
Slide Ref # Reference 16.7 PSYCHOSIS 18 12 CHLORPROMAZINE SAMF 10th edition, 2012. 19 13 FLUPHENAZINE DECANOATE SAMF 10th edition, 2012 19 13 FLUPENTHIXOL DECANOATE SAMF 10th edition, 2012 19 13 ZUCLOPENTHIXOL DECANOATE SAMF 10th edition, 2012 20 14 RISPERIDONE SAMF 10th edition, 2012 20 14 BIPERIDEN SAMF 10th edition, 2012 16.8 SUBSTANCE RELATED DISORDERS Substance use disorder defined as per the DSM V criteria as the presence of 2 of 11 criteria; and further clustered in four groups: Impaired control; Social impairment; Risky use; Pharmacologic dependence. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th edition. Available at: http://www.dsm5.org/Pages/Default.aspx 21 15 16.8.1 SUBSTANCE USE DISORDERS 22 16 DIAZEPAM American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th edition. Available at: http://www.dsm5.org/Pages/Default.aspx Adult Hospital level STG, 2012. National Department of Health. National Policy guidelines on detoxification of psychoactive substances. PRIMARY HEALTHCARE 2014 IMPLEMENTATION SLIDES: RESPIRATORY 42
Slide Ref # Reference 16.8.2 SUBSTANCE-INDUCED PSYCHOSIS 23 17 DIAZEPAM American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th edition. Available at: http://www.dsm5.org/Pages/Default.aspx Adult Hospital level STG, 2012. National Department of Health. National Policy guidelines on detoxification of psychoactive substances. 23 17 MIDAZOLAM American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th edition. Available at: http://www.dsm5.org/Pages/Default.aspx Adult Hospital level STG, 2012. National Department of Health. National Policy guidelines on detoxification of psychoactive substances. 23 17 HALOPERIDOL American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th edition. Available at: http://www.dsm5.org/Pages/Default.aspx Adult Hospital level STG, 2012. National Department of Health. National Policy guidelines on detoxification of psychoactive substances. 23 17 PROMETHAZINE American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th edition. Available at: http://www.dsm5.org/Pages/Default.aspx Adult Hospital level STG, 2012. National Department of Health. National Policy guidelines on detoxification of psychoactive substances. PRIMARY HEALTHCARE 2014 IMPLEMENTATION SLIDES: RESPIRATORY 43
Slide Ref # Reference 16.8.4 ALCOHOL WITHDRAWAL (UNCOMPLICATED) 24 18 THIAMINE Lingford-Hughes AR, Welch S, Peters L, Nutt DJ; British Association for Psychopharmacology, Expert Reviewers Group. BAP updated guidelines: evidence-based guidelines for the pharmacological management of substance abuse, harmful use, addiction and comorbidity: recommendations from BAP. J Psychopharmacol. 2012 Jul;26(7):899-952. http://www.ncbi.nlm.nih.gov/pubmed/22628390 Day E, Bentham PW, Callaghan R, Kuruvilla T, George S. Thiamine for prevention and treatment of Wernicke- Korsakoff Syndrome in people who abuse alcohol. Cochrane Database Syst Rev. 2013 Jul 1;7:CD004033. http://www.ncbi.nlm.nih.gov/pubmed/23818100 Ambrose ML, Bowden SC, Wehan G. Thiamine treatment and working memory function of alcohol dependent people: preliminary findings. Alcohol Clin Exp Res 2001; 25: 112 16. http://www.ncbi.nlm.nih.gov/pubmed/11198705 Cook CC. Prevention and treatment of Wernicke-Korsakoff Syndrome. Alcohol Alcohol Suppl 2000; 35: 19 20. http://www.ncbi.nlm.nih.gov/pubmed/11304070 Thomson AD, Cook CCH, Touquet R, Henry JA. The Royal College of Physicians report on alcohol: guidelines for managing Wernicke s encephalopathy in the accident and emergency department. Alcohol Alcohol Suppl 2002; 37: 513 21. http://www.ncbi.nlm.nih.gov/pubmed/12414541 Cook CCH, Hallwood PM, Thomson AD. B-vitamin deficiency and neuro-psychiatric syndromes in alcohol misuse. Alcohol Alcohol Suppl 1998; 33: 317 36. http://www.ncbi.nlm.nih.gov/pubmed/9719389 Sechi G, Serra A. Wernicke's encephalopathy: new clinical settings and recent advances in diagnosis and management. Lancet Neurol. 2007 May;6(5):442-55. Review. http://www.ncbi.nlm.nih.gov/pubmed/17434099 24 18 DIAZEPAM Lingford-Hughes AR, Welch S, Peters L, Nutt DJ; British Association for Psychopharmacology, Expert Reviewers Group. BAP updated guidelines: evidence-based guidelines for the pharmacological management of substance abuse, harmful use, addiction and comorbidity: recommendations from BAP. J Psychopharmacol. 2012 Jul;26(7):899-952. http://www.ncbi.nlm.nih.gov/pubmed/22628390 Cook CC. Prevention and treatment of Wernicke-Korsakoff Syndrome. Alcohol Alcohol Suppl 2000; 35: 19 20. http://www.ncbi.nlm.nih.gov/pubmed/11304070 Thomson AD, Cook CCH, Touquet R, Henry JA. The Royal College of Physicians report on alcohol: guidelines for managing Wernicke s encephalopathy in the accident and emergency department. Alcohol Alcohol Suppl 2002; 37: 513 21. http://www.ncbi.nlm.nih.gov/pubmed/12414541 Sechi G, Serra A. Wernicke's encephalopathy: new clinical settings and recent advances in diagnosis and management. Lancet Neurol. 2007 May;6(5):442-55. Review. http://www.ncbi.nlm.nih.gov/pubmed/17434099 44 44
Slide Ref # Reference 16.1 AGGRESSIVE DISRUPTIVE BEHAVIOUR IN ADULTS 26 19 DIAZEPAM Gillies D, Sampson S, Beck A, Rathbone J. Benzodiazepines for psychosis-induced aggression or agitation. Cochrane Database Syst Rev. 2013 Apr 30;4:CD003079. NICE clinical guideline 25: The short-term management of disturbed/violent behaviour in in-patient psychiatric settings and emergency departments. Leucht S, Heres S, Kissling W, Davis JM.Evidence-based pharmacotherapy of schizophrenia.Int J Neuropsychopharmacol. 2011 Mar;14(2):269-84. Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012 Feb;13(1):26-34. Adult Hospital level STG, 2012. 16.1 AGGRESSIVE DISRUPTIVE BEHAVIOUR IN ADULTS 26 19 MIDAZOLAM Gillies D, Sampson S, Beck A, Rathbone J. Benzodiazepines for psychosis-induced aggression or agitation. Cochrane Database Syst Rev. 2013 Apr 30;4:CD003079. TREC I: TREC Collaborative Group. Rapid tranquillisation for agitated patients in emergency psychiatric rooms: a randomised trial of midazolam versus haloperidol plus promethazine. BMJ. 2003 Sep 27;327(7417):708-13. TREC II: Alexander J, Tharyan P, Adams C, John T, Mol C, Philip J. Rapidtranquillisation of violent or agitated patients in a psychiatric emergencysetting. Pragmatic randomised trial of intramuscular lorazepam v. haloperidol plus promethazine. Br J Psychiatry. 2004 Jul;185:63-9. TREC III: Huf G, Coutinho ES, Adams CE; TREC Collaborative Group. Rapid tranquillisationin psychiatric emergency settings in Brazil: pragmatic randomised controlled trial of intramuscular haloperidol versus intramuscular haloperidol pluspromethazine. BMJ. 2007 Oct 27;335(7625):869. http://www.ncbi.nlm.nih.gov/pubmed/17954515 NICE clinical guideline 25: The short-term management of disturbed/violent behaviour in in-patient psychiatric settings and emergency departments. Leucht S, Heres S, Kissling W, Davis JM.Evidence-based pharmacotherapy of schizophrenia.Int J Neuropsychopharmacol. 2011 Mar;14(2):269-84. Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012 Feb;13(1):26-34. Adult Hospital level STG, 2012. 45
Slide Ref # Reference 16.1 AGGRESSIVE DISRUPTIVE BEHAVIOUR IN ADULTS 26 19 HALOPERIDOL Gillies D, Sampson S, Beck A, Rathbone J. Benzodiazepines for psychosis-induced aggression or agitation. Cochrane Database Syst Rev. 2013 Apr 30;4:CD003079. TREC I: TREC Collaborative Group. Rapid tranquillisation for agitated patients in emergency psychiatric rooms: a randomised trial of midazolam versus haloperidol plus promethazine. BMJ. 2003 Sep 27;327(7417):708-13. TREC II: Alexander J, Tharyan P, Adams C, John T, Mol C, Philip J. Rapidtranquillisation of violent or agitated patients in a psychiatric emergencysetting. Pragmatic randomised trial of intramuscular lorazepam v. haloperidol plus promethazine. Br J Psychiatry. 2004 Jul;185:63-9. TREC III: Huf G, Coutinho ES, Adams CE; TREC Collaborative Group. Rapid tranquillisationin psychiatric emergency settings in Brazil: pragmatic randomised controlled trial of intramuscular haloperidol versus intramuscular haloperidol pluspromethazine. BMJ. 2007 Oct 27;335(7625):869. http://www.ncbi.nlm.nih.gov/pubmed/17954515 NICE clinical guideline 25: The short-term management of disturbed/violent behaviour in in-patient psychiatric settings and emergency departments. Leucht S, Heres S, Kissling W, Davis JM.Evidence-based pharmacotherapy of schizophrenia.Int J Neuropsychopharmacol. 2011 Mar;14(2):269-84. Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012 Feb;13(1):26-34. Adult Hospital level STG, 2012. PRIMARY HEALTHCARE 2014 IMPLEMENTATION SLIDES: RESPIRATORY 46
Slide Ref # Reference 16.1 AGGRESSIVE DISRUPTIVE BEHAVIOUR IN ADULTS 26 19 PROMETHAZINE Gillies D, Sampson S, Beck A, Rathbone J. Benzodiazepines for psychosis-induced aggression or agitation. Cochrane Database Syst Rev. 2013 Apr 30;4:CD003079. TREC I: TREC Collaborative Group. Rapid tranquillisation for agitated patients in emergency psychiatric rooms: a randomised trial of midazolam versus haloperidol plus promethazine. BMJ. 2003 Sep 27;327(7417):708-13. TREC II: Alexander J, Tharyan P, Adams C, John T, Mol C, Philip J. Rapidtranquillisation of violent or agitated patients in a psychiatric emergencysetting. Pragmatic randomised trial of intramuscular lorazepam v. haloperidol plus promethazine. Br J Psychiatry. 2004 Jul;185:63-9. TREC III: Huf G, Coutinho ES, Adams CE; TREC Collaborative Group. Rapid tranquillisationin psychiatric emergency settings in Brazil: pragmatic randomised controlled trial of intramuscular haloperidol versus intramuscular haloperidol pluspromethazine. BMJ. 2007 Oct 27;335(7625):869. http://www.ncbi.nlm.nih.gov/pubmed/17954515 NICE clinical guideline 25: The short-term management of disturbed/violent behaviour in in-patient psychiatric settings and emergency departments. Leucht S, Heres S, Kissling W, Davis JM.Evidence-based pharmacotherapy of schizophrenia.Int J Neuropsychopharmacol. 2011 Mar;14(2):269-84. Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012 Feb;13(1):26-34. Adult Hospital level STG, 2012. 16.2 ANXIETY AND STRESS AND RELATED DISORDERS IN ADULTS 27 20 DIAZEPAM Adult Hospital level STG, 2012. Batelaan NM, Van Balkom AJ, Stein DJ. Evidence-based pharmacotherapy of panic disorder: an update. Int J Neuropsychopharmacol. 2012 Apr;15(3):403-15. http://www.ncbi.nlm.nih.gov/pubmed/21733234 Baldwin DS, Anderson IM, Nutt DJ, Allgulander C, Bandelow B, den Boer JA, Christmas DM, Davies S, Fineberg N, Lidbetter N, MaliziaA, McCrone P, Nabarro D, O'Neill C, Scott J, van der Wee N, Wittchen HU. Evidence-based pharmacological treatment of anxiety disorders, post-traumatic stress disorder and obsessive-compulsive disorder: a revision of the 2005 guidelines from the British Association for Psychopharmacology. J Psychopharmacol. 2014 May;28(5):403-39 http://www.ncbi.nlm.nih.gov/pubmed/24713617 47
Slide Ref # Reference 16.2 ANXIETY AND STRESS AND RELATED DISORDERS IN ADULTS 27 20 CITALOPRAM Adult Hospital level STG, 2012. Batelaan NM, Van Balkom AJ, Stein DJ. Evidence-based pharmacotherapy of panic disorder: an update. Int J Neuropsychopharmacol. 2012 Apr;15(3):403-15. http://www.ncbi.nlm.nih.gov/pubmed/21733234 Baldwin DS, Anderson IM, Nutt DJ, Allgulander C, Bandelow B, den Boer JA, Christmas DM, Davies S, Fineberg N, Lidbetter N, MaliziaA, McCrone P, Nabarro D, O'Neill C, Scott J, van der Wee N, Wittchen HU. Evidence-based pharmacological treatment of anxiety disorders, post-traumatic stress disorder and obsessive-compulsive disorder: a revision of the 2005 guidelines from the British Association for Psychopharmacology. J Psychopharmacol. 2014 May;28(5):403-39 http://www.ncbi.nlm.nih.gov/pubmed/24713617 27 20 FLUOXETINE Adult Hospital level STG, 2012. Batelaan NM, Van Balkom AJ, Stein DJ. Evidence-based pharmacotherapy of panic disorder: an update. Int J Neuropsychopharmacol. 2012 Apr;15(3):403-15. http://www.ncbi.nlm.nih.gov/pubmed/21733234 Baldwin DS, Anderson IM, Nutt DJ, Allgulander C, Bandelow B, den Boer JA, Christmas DM, Davies S, Fineberg N, Lidbetter N, MaliziaA, McCrone P, Nabarro D, O'Neill C, Scott J, van der Wee N, Wittchen HU. Evidence-based pharmacological treatment of anxiety disorders, post-traumatic stress disorder and obsessive-compulsive disorder: a revision of the 2005 guidelines from the British Association for Psychopharmacology. J Psychopharmacol. 2014 May;28(5):403-39 http://www.ncbi.nlm.nih.gov/pubmed/24713617 28 21 DIAZEPAM Adult Hospital level STG, 2012. Batelaan NM, Van Balkom AJ, Stein DJ. Evidence-based pharmacotherapy of panic disorder: an update. Int J Neuropsychopharmacol. 2012 Apr;15(3):403-15. http://www.ncbi.nlm.nih.gov/pubmed/21733234 Baldwin DS, Anderson IM, Nutt DJ, Allgulander C, Bandelow B, den Boer JA, Christmas DM, Davies S, Fineberg N, Lidbetter N, MaliziaA, McCrone P, Nabarro D, O'Neill C, Scott J, van der Wee N, Wittchen HU. Evidence-based pharmacological treatment of anxiety disorders, post-traumatic stress disorder and obsessive-compulsive disorder: a revision of the 2005 guidelines from the British Association for Psychopharmacology. J Psychopharmacol. 2014 May;28(5):403-39 http://www.ncbi.nlm.nih.gov/pubmed/24713617 PRIMARY HEALTHCARE 2014 IMPLEMENTATION SLIDES: RESPIRATORY 48
Slide Ref # Reference 16.2 ANXIETY AND STRESS AND RELATED DISORDERS IN ADULTS 29 22 SSRIS FOR CHRONIC ANXIETY: NICE. NICE clinical guideline CG113: Generalised anxiety disorder and panic disorder (with or without agoraphobia) in adults: Management in primary, secondary and community care, January 2011. http://www.nice.org.uk/guidance/cg113 Bereza BG, Machado M, Ravindran AV, Einarson TR. Evidence-based review of clinical outcomes of guideline- recommended pharmacotherapies for generalized anxiety disorder. Can J Psychiatry. 2012 Aug;57(8):470-8. Baldwin DS, Anderson IM, Nutt DJ, Allgulander C, Bandelow B, den Boer JA,Christmas DM, Davies S, Fineberg N, Lidbetter N, Malizia A, McCrone P, Nabarro D, O'Neill C, Scott J, van der Wee N, Wittchen HU. Evidence-based pharmacological treatment of anxiety disorders, post-traumatic stress disorder and obsessive-compulsive disorder: a revision of the 2005 guidelines from the British Association for Psychopharmacology. J Psychopharmacol. 2014 May;28(5):403-39. 29 22 FLUOXETINE: Baldwin D, Woods R, Lawson R, Taylor D. Efficacy of drug treatments for generalised anxiety disorder: systematic review and meta-analysis. BMJ. 2011 Mar 11;342:d1199. 30 23 Contract circular HP09-2014SD 16.6 MOOD DISORDERS 32 25 DURATION OF SSRI THERAPY: American Psychiatric Association (APA). Practice guideline for the treatment of patients with major depressive disorder. 3rd ed. Arlington (VA): American Psychiatric Association (APA); 2010 Oct. http://www.guideline.gov/content.aspx?id=24158 NICE clinical guideline 90. [Internet] Depression in adults. [Issued: October 2009; cited February 2014]. Available at: www.guidance.nice.org.uk/cg90 Malani AK, Ammar H. Medical management of depression. N Engl J Med. 2006 Feb 9;354(6):646-8; author reply 646-8. http://www.ncbi.nlm.nih.gov/pubmed/16470956 Anderson IM, Ferrier IN, Baldwin RC, Cowen PJ, Howard L, Lewis G, Matthews K, McAllister-Williams RH, Peveler RC, Scott J, Tylee A. Evidence-based guidelines for treating depressive disorders with antidepressants: a revision of the 2000 British Association for Psychopharmacology guidelines. J Psychopharmacol. 2008 Jun;22(4):343-96. http://www.ncbi.nlm.nih.gov/pubmed/18413657 Crismon ML, Trivedi M, Pigott TA, Rush AJ, Hirschfeld RM, Kahn DA, DeBattista C, Nelson JC, Nierenberg AA, Sackeim HA, Thase ME. The Texas Medication Algorithm Project: report of the Texas Consensus Conference Panel on Medication Treatment of Major Depressive Disorder. J Clin Psychiatry. 1999 Mar;60(3):142-56. http://www.ncbi.nlm.nih.gov/pubmed/10192589 49