Cataracts: Causes, Effects, and Treatment



Cataract
It is a clouding or opaqueness of the crystalline
lens which leads gradual painless blurring and
eventual loss of vision

A cause of blindness and is conventionally
treated with surgery
Vision loss occurs because opacification of
the lens obstructs light from passing and
being focused on the retina
3
rd
leading cause of preventable blindness
D
u
e
t
o
e
t
i
o
l
o
g
i
c
a
l
f
a
c
t
o
r
s
D
e
c
r
e
a
s
e
i
n
t
h
e
f
u
n
c
t
i
o
n
o
f
a
c
t
i
v
e
t
r
a
n
s
p
o
r
t
o
f
p
u
m
p
m
e
c
h
a
n
i
s
m
o
f
l
e
n
s
R
e
v
e
r
s
a
l
o
f
s
o
d
i
u
m
/
p
o
t
a
s
s
i
u
m
r
a
t
i
o
H
y
d
r
a
t
i
o
n
o
f
l
e
n
s
f
i
b
e
r
s
D
e
n
a
t
u
r
a
t
i
o
n
o
f
l
e
n
s
p
r
o
t
e
i
n
s
O
p
a
c
i
f
i
c
a
t
i
o
n
o
f
c
o
r
t
i
c
a
l
l
e
n
s
f
i
b
e
r
s
A
l
t
e
r
e
d
o
x
i
d
a
t
i
v
e
r
e
a
c
t
i
o
n
s
D
e
c
r
e
a
s
e
d
l
e
v
e
l
o
f
a
m
i
n
o
a
c
i
d
s
D
e
c
r
e
a
s
e
d
s
y
n
t
h
e
s
i
s
o
f
p
r
o
t
e
i
n
s
i
n
l
e
n
s
f
i
b
e
r
s
Causes
Aging
Loss of lens transparency
Decreased oxygen uptake
Denaturation of proteins in lens
Accumulation of a yellow brown pigment
due to the break down of lens protein
T
r
a
u
m
a
Blunt trauma causes swelling, thickening
and whitening of the lens fibers
Swelling resolves but white color remains
Or
Capsule can be damaged and allows water
from other parts to enter the lens,
obstructing light from reaching the retina
Associated ocular conditions
Retinitis pigmentosa – degenerative
disorder caused by abnormalities of the
photoreceptors
Myopia
Retinal detachment and retinal surgery
Infection
Toxic factors
Corticosteroids
Chemical eye burns or poisoning
Cigarette smoking
Reduced levels of antioxidants – antioxidants
helps to prevent oxidative changes in proteins
and fat
Poor nutrition
Obesity
Nutritional factors
Physical factors
Perforation of lens with sharp object or
foreign body
Electric shock
Ultraviolet radiation
R
i
s
k
f
a
c
t
o
r
s
–
a
g
e
,
u
l
t
r
a
v
i
o
l
e
t
l
i
g
h
t
e
x
p
o
s
u
r
e
,
h
i
g
h
d
o
s
e
o
f
r
a
d
i
a
t
i
o
n
e
x
p
o
s
u
r
e
,
d
r
u
g
e
f
f
e
c
t
s
,
t
r
a
u
m
a
Diabetes mellitus
Down syndrome
Renal disorders
Musculoskeletal disorders
Systemic diseases and syndromes
Classification
Age related cataracts
(senile cataract)
Congenital cataract
Secondary cataract
Traumatic
B
a
s
e
d
o
n
t
h
e
c
h
a
r
a
c
t
e
r
i
s
t
i
c
s
Partial or complete
Stationary or
progressive
Hard or soft
B
a
s
e
d
o
n
t
h
e
a
r
e
a
o
f
l
e
n
s
Nuclear, cortical and
posterior subcapsular
cataracts
Nuclear cataract
Central opacity in the lens
It is associated with myopia
Cortical cataract involves the anterior, posterior or equatorial
(peripheral) cortex of the lens
People with highest levels of sunlight exposure have twice the
risk
Posterior subcapsular cataract occur in front of the posterior
capsule.
Typically develop in younger people
Associated with prolonged corticosteroid use, diabetic and
ocular trauma
Cortical
cataract
Posterior
subcapsular
cataract
Signs and symptoms
Painless, blurry vision
Reduced visual acuity
Myopic shift – return of ability to read without
glasses
Astigmatism - optical defect in which vision is
blurred due to the inability of the optics of the
eye to focus a point object into a sharp focused
image on the retina
Visible opaqueness
Diplopia
Abnormal color perception, glare (due
to light scatter caused by lens opacities
and significantly worse at night and in
bright light when th pupil dilates )
Brunescence – color shift from yellow
to brown
Reduced light transmission
Color of pupil will be yellowish, gray or
white
Develop in both eyes
Diagnostic findings
Visual acuity measurements
Snellen visual acuity test
Ophthalmoscopy
Slit lamp microscopic examination
Blood test
Visual field perimetry
A – scan ultrasound
Prevention
Avoid the risk factors – UV rays, x
rays, smoking
Wear sunglasses
Regular intake of antioxidants
(vitamins A,C AND E) would protect
against risks
Prevent accidents
Treat underlying disorders properly
Management
Non surgical treatment will not cure cataract
Surgery is performed as outpatient basis
usually takes less than 1 hour and
discharged in 30 minutes
Topical and intra ocular anesthesia – 1%
lidocaine gel is used
Patient can communicate and cooperate
during surgery
IV moderate sedation – to minimize anxiety
When both eyes have cataracts – one eye is
treated first, after several weeks the other
cataracts is been managed.
This will help one eye to heal properly and
the doctor can check the surgical procedure
is effective or not
The doctor can also check the presence of
any complications due to surgery.
Phacoemulsification
Most widely used cataract surgery
Through a very small incision in the surface of the
eye
An ultrasound probe is then inserted
This uses ultrasonic vibrations to dissolve
(phacoemulsify) the clouded lens
These tiny fragmented pieces are then suctioned
out through the same ultrasound probe
Once the cataract is removed, an artificial lens is
placed into the thin capsular bag
Steps of phacoemulsification
Anesthesia
Exposure of the eyeball using a lid speculum
Entry into the eye through a minimal incision
Viscoelastic injection to stabilize the anterior chamber
Capsulorhexis -Ultrasonic destruction or emulsification
and aspiration of the fragments
Implantation of the intra ocular lens
Viscoelastic removal
Wound sealing
Extra capsular cataract extraction
ECCE
Only uses in very advanced cataracts where the lens
is too dense to dissolve into fragments
This technique requires a larger incision so that the
cataract can be removed in one piece without being
fragmented inside the eye
The posterior capsule is left intact.
An artificial lens is place in the same capsular bag
An eye patch after the surgery is needed.
Intracapsular cataract extraction
ICCE
This surgical technique requires an even
larger wound than extracapsular surgery
In this the entire lens and the surrounding
capsule is removed
Intra ocular lens is placed in front of the iris.
Lens replacement
After removal of the crystalline lens, the
patient is referred to as aphakic (without lens)
Three lens replacement options – aphakic eye
glasses, contact lens, and IOL implants
IOL -It is permanently placed, no maintenance
or handling and neither felt by the patient nor
noticed by others
Made of silicone or acrylic material
M
o
n
o
f
o
c
a
l
l
e
n
s
–
c
o
m
m
o
n
l
y
i
m
p
l
a
n
t
e
d
l
e
n
s
e
s
They have equal power in all regions of the
lens and can provide high quality distance
vision
It have sharpest focus at only one distance
Usually a pair of spectacles is need for
better quality
T
o
r
i
c
l
e
n
s
–
i
t
h
a
v
e
m
o
r
e
p
o
w
e
r
i
n
o
n
e
s
p
e
c
i
f
i
c
r
e
g
i
o
n
i
n
t
h
e
l
e
n
s
M
u
l
t
i
f
o
c
a
l
l
e
n
s
–
l
a
t
e
s
t
a
d
v
a
n
c
e
m
e
n
t
s
It have variety of regions with different power
that allows individuals to see at a variety of
distances, including distance and near
BUT They can cause more glare than
monofocal or toric lenses
Preoperative care
Eye examination by surgeon to confirm the
presence of cataract and to determine the
patient is suitable candidate for surgery
Eyes should have normal pressure. If
increased pressure is there it should be
controlled with medication before surgery
In some cases a combined cataract –
glaucoma procedure (phaco trabeculectomy)
can be planned
Pupil should be adequately dilated
Retinal detachment should be ruled
NPO – 6- 8 HOURS BEFORE in selected cases
Pre operative antibiotic eye drops
NSAIDS eye drops
Mydriatics – phenylephrine HCL acid
Every 10 min for four doses atleast 1 hour
before surgery
cycloplegics (paralyses the ciliary muscles thus
losing the accommodation of lens) -
tropicamide, atropine, cyclopentolate HCL
Post operative care
Discharged within few hours
Eye patch should be done – the dressing is
removed a day after surgery
Position the patient on back or up operated side to
prevent pressure in operated eye
Eye protective shields should be provided for 2-3
weeks for avoiding accidental injury
Proper follow up – 4-5 visit in a period of 5 to 6
weeks
Tell the patient to avoid situation that IOP can
increases (sneezing, coughing, vomiting, straining,
or sudden bending)
Instruct the patient
Avoid touching the operative eye
Take care to prevent soap or water from entering the
operative eye during face or hair washing
Avoid heavy lifting
Exercise in moderation
Wash hands before instilling eye medications
Wear sunglasses to prevent bright lights
Wait 2 -3 min between administration of different eye
medications (antibiotics and corticosteroids)
Administer eye ointments last
Avoid smoking, driving
Complications of cataract surgery
Immediate preoperative complications
Retrobulbar hemorrhage – can result due to
anesthesia injection
Effects – increased IOP, lid tightness, and
subconjunctival hemorrhage
Management
Canthotomy – slitting of canthus to reduce the
IOP
Puncture of anterior chamber
Intraoperative complications
Rupture of posterior capsule and
Suprachoroidal hemorrhage
Management is vitrectomy
Post operative complications
Early
Acute bacterial endophthalmitis – antibiotic therapy
Toxic anterior segment syndrome (TASS) – non
infectious inflammation caused by toxic agent used
to sterilize surgical instruments
Late
Suture related problems
Malposition of IOL
Opacification of posterior capsule
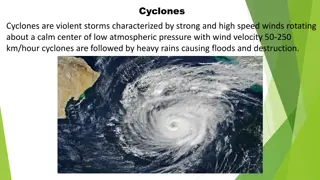
Cataract is a common eye condition characterized by clouding of the lens, leading to gradual vision loss. It is the third leading cause of preventable blindness and is typically treated with surgery. Various factors, such as aging, trauma, and toxic exposures, contribute to the development of cataracts. Understanding the causes and associated conditions can help in prevention and early detection of this vision impairment.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Cataract It is a clouding or opaqueness of the crystalline lens which leads gradual painless blurring and eventual loss of vision
A cause of blindness and is conventionally treated with surgery Vision loss occurs because opacification of the lens obstructs light from passing and being focused on the retina 3rdleading cause of preventable blindness
Due to etiological factors Altered oxidative reactions Decrease in the function of active transport of pump mechanism of lens Decreased level of amino acids Reversal of sodium /potassium ratio Hydration of lens fibers Decreased synthesis of proteins in lens fibers Denaturation of lens proteins Opacification of cortical lens fibers
Causes Aging Loss of lens transparency Decreased oxygen uptake Denaturation of proteins in lens Accumulation of a yellow brown pigment due to the break down of lens protein
Trauma Blunt trauma causes swelling, thickening and whitening of the lens fibers Swelling resolves but white color remains Or Capsule can be damaged and allows water from other parts to enter the lens, obstructing light from reaching the retina
Associated ocular conditions Retinitis pigmentosa degenerative disorder caused by abnormalities of the photoreceptors Myopia Retinal detachment and retinal surgery Infection
Toxic factors Corticosteroids Chemical eye burns or poisoning Cigarette smoking Nutritional factors Reduced levels of antioxidants antioxidants helps to prevent oxidative changes in proteins and fat Poor nutrition Obesity
Physical factors Perforation of lens with sharp object or foreign body Electric shock Ultraviolet radiation Risk factors age, ultraviolet light exposure, high dose of radiation exposure, drug effects, trauma
Systemic diseases and syndromes Diabetes mellitus Down syndrome Renal disorders Musculoskeletal disorders
Classification Age related cataracts (senile cataract) Congenital cataract Secondary cataract Traumatic Based on the characteristics Partial or complete Stationary or progressive Hard or soft Based on the area of lens Nuclear, cortical and posterior subcapsular cataracts
Nuclear cataract Central opacity in the lens It is associated with myopia Cortical cataract Cortical cataract involves the anterior, posterior or equatorial (peripheral) cortex of the lens People with highest levels of sunlight exposure have twice the risk Posterior subcapsular cataract Posterior subcapsular cataract occur in front of the posterior capsule. Typically develop in younger people Associated with prolonged corticosteroid use, diabetic and ocular trauma
Signs and symptoms Painless, blurry vision Reduced visual acuity Myopic shift return of ability to read without glasses Astigmatism - optical defect in which vision is blurred due to the inability of the optics of the eye to focus a point object into a sharp focused image on the retina Visible opaqueness
Diplopia Abnormal color perception, glare (due to light scatter caused by lens opacities and significantly worse at night and in bright light when th pupil dilates ) Brunescence color shift from yellow to brown Reduced light transmission Color of pupil will be yellowish, gray or white Develop in both eyes
Diagnostic findings Visual acuity measurements Snellen visual acuity test Ophthalmoscopy Slit lamp microscopic examination Blood test Visual field perimetry A scan ultrasound
Prevention Avoid the risk factors UV rays, x rays, smoking Wear sunglasses Regular intake of antioxidants (vitamins A,C AND E) would protect against risks Prevent accidents Treat underlying disorders properly
Management Non surgical treatment will not cure cataract Surgery is performed as outpatient basis usually takes less than 1 hour and discharged in 30 minutes Topical and intra ocular anesthesia 1% lidocaine gel is used Patient can communicate and cooperate during surgery IV moderate sedation to minimize anxiety
When both eyes have cataracts one eye is treated first, after several weeks the other cataracts is been managed. This will help one eye to heal properly and the doctor can check the surgical procedure is effective or not The doctor can also check the presence of any complications due to surgery.
Phacoemulsification Most widely used cataract surgery Through a very small incision in the surface of the eye An ultrasound probe is then inserted This uses ultrasonic vibrations to dissolve (phacoemulsify) the clouded lens These tiny fragmented pieces are then suctioned out through the same ultrasound probe Once the cataract is removed, an artificial lens is placed into the thin capsular bag
Steps of phacoemulsification Anesthesia Exposure of the eyeball using a lid speculum Entry into the eye through a minimal incision Viscoelastic injection to stabilize the anterior chamber Capsulorhexis -Ultrasonic destruction or emulsification and aspiration of the fragments Implantation of the intra ocular lens Viscoelastic removal Wound sealing
Extra capsular cataract extraction ECCE Only uses in very advanced cataracts where the lens is too dense to dissolve into fragments This technique requires a larger incision so that the cataract can be removed in one piece without being fragmented inside the eye The posterior capsule is left intact. An artificial lens is place in the same capsular bag An eye patch after the surgery is needed.
Intracapsular cataract extraction ICCE This surgical technique requires an even larger wound than extracapsular surgery In this the entire lens and the surrounding capsule is removed Intra ocular lens is placed in front of the iris.
Lens replacement After removal of the crystalline lens, the patient is referred to as aphakic (without lens) Three lens replacement options aphakic eye glasses, contact lens, and IOL implants IOL -It is permanently placed, no maintenance or handling and neither felt by the patient nor noticed by others Made of silicone or acrylic material
Monofocal lens commonly implanted lenses They have equal power in all regions of the lens and can provide high quality distance vision It have sharpest focus at only one distance Usually a pair of spectacles is need for better quality
Toric lens it have more power in one specific region in the lens Multifocal lens latest advancements It have variety of regions with different power that allows individuals to see at a variety of distances, including distance and near BUT They can cause more glare than monofocal or toric lenses
Preoperative care Eye examination by surgeon to confirm the presence of cataract and to determine the patient is suitable candidate for surgery Eyes should have normal pressure. If increased pressure is there it should be controlled with medication before surgery In some cases a combined cataract glaucoma procedure (phaco trabeculectomy) can be planned
Pupil should be adequately dilated Retinal detachment should be ruled NPO 6- 8 HOURS BEFORE in selected cases Pre operative antibiotic eye drops NSAIDS eye drops Mydriatics phenylephrine HCL acid Every 10 min for four doses atleast 1 hour before surgery cycloplegics (paralyses the ciliary muscles thus losing the accommodation of lens) - tropicamide, atropine, cyclopentolate HCL
Post operative care Discharged within few hours Eye patch should be done the dressing is removed a day after surgery Position the patient on back or up operated side to prevent pressure in operated eye Eye protective shields should be provided for 2-3 weeks for avoiding accidental injury Proper follow up 4-5 visit in a period of 5 to 6 weeks Tell the patient to avoid situation that IOP can increases (sneezing, coughing, vomiting, straining, or sudden bending)
Instruct the patient Avoid touching the operative eye Take care to prevent soap or water from entering the operative eye during face or hair washing Avoid heavy lifting Exercise in moderation Wash hands before instilling eye medications Wear sunglasses to prevent bright lights Wait 2 -3 min between administration of different eye medications (antibiotics and corticosteroids) Administer eye ointments last Avoid smoking, driving
Complications of cataract surgery Immediate preoperative complications Retrobulbar hemorrhage can result due to anesthesia injection Effects increased IOP, lid tightness, and subconjunctival hemorrhage Management Canthotomy slitting of canthus to reduce the IOP Puncture of anterior chamber
Intraoperative complications Rupture of posterior capsule and Suprachoroidal hemorrhage Management is vitrectomy
Post operative complications Early Acute bacterial endophthalmitis antibiotic therapy Toxic anterior segment syndrome (TASS) non infectious inflammation caused by toxic agent used to sterilize surgical instruments Late Suture related problems Malposition of IOL Opacification of posterior capsule