CalPERS Pilot ACO Experience & Learnings Summary



CalPERS Pilot ACO
Experience & Learnings
Scott Whyte, Vice President IT Connectivity
Mary Carol Todd, Senior Vice President Clinical Efficiency
Steve Foerster, Senior Director Managed Care



2
•
Background
•
Virtual Integration & Management Structure
•
The Financial Model
•
IT Connectivity
•
Care Management/Clinical Efforts
•
Lessons Learned
•
Q & A
Outline
3
•
The Population:
~42,000 CalPERS Members assigned to Hill Physicians
Medical Group.
•
The Model:
Virtual Integration between 4 Sacramento CHW hospitals, Blue
Shield, and Hill Physicians conceived early in CY ’07.
•
CalPERS:
The California Public Employees’ Retirement System (CalPERS)
provides retirement and health benefits to more than 1.6 million public
employees, retirees, and their families.
•
Dignity Health:
formerly named Catholic Heathcare West, operates
more than 40 hospitals and care centers serving communities across
California, Arizona, and Nevada.
•
Blue Shield of California:
Blue Shield of California, an indepedent
member of the Blue Shield Association, is a not-for-profit health plan
dedicated to providing Californians with access to high-quality care at an
affordable price.
•
Hill Physicians Medical Group:
Hill Physicians is a medical group of more
than 3,500 primary care physicians, specialists, sub-specialists, and
consultants serving the Northern California region.
Sacramento Pilot ACO Background
4
•
In 2007, Dignity Health, Hill Physicians, and Blue Shield began
planning for the CalPERS Pilot with the following strategic objectives:
–
Reduce the cost of healthcare via care management (utilization) in order to
provide a zero percent trend in price to CalPERS while enabling the providers
to receive rate increases.
–
Continue the existing CalPERS network in Sacramento.
–
Compete with Kaiser for market share.
–
Enhance collaboration amongst Dignity Health, Hill, and Blue Shield
–
Improve quality and access to care.
•
The Delivery System
–
4 Dignity Health Sacramento Hospitals
–
Hill Physicians Medical Group
–
Other Blue Shield HMO Contracted Providers
CalPERS Pilot ACO Background
ACO Goals
Deliver Cost
Savings
Grow
Membership
Reduce cost of healthcare trend in
aggregate for members in the pilot
Develop way to work together that aligns parties to
drive continuous improvement (cost, quality, service)
and allows for expansion to other geographic areas
Attract new members
Create
Sustainable
Model for
Expansion
5
The Virtual Integration Vision
•
Vision: Providing affordable healthcare while ensuring the optimal health of members.
•
We will achieve our vision through a commitment to quality and an integrated, holistic and
collaborative approach to healthcare delivery that engages the member as an active participant
in their healthcare and supports them in making
healthy lifestyle choices.
Integrated Delivery Network
B
l
u
e
S
h
i
e
l
d
o
f
C
a
l
i
f
o
r
n
i
a
D
i
g
n
i
t
y
H
e
a
l
t
h
H
i
l
l
P
h
y
s
i
c
i
a
n
s
M
e
d
i
c
a
l
G
r
o
u
p
clinical best practices
data integration
quality metrics and reporting
integrated processes
Aligned Incentives:
each partner contributes to cost savings and
together share risk for targeted cost reduction goals
member and physician engagement
6
7
•
Pilot Board
–
Core Team
–
Finance Committee
–
Legal/Contracting Committee
–
Cost Of Health Care Committee w/ Strategy Work Groups (Constant
Evolution)
•
Facilities
•
Population Management
•
Electronic Connectivity
•
Physician Variability
•
Pharmacy
Virtual Management Structure
8
•
Dignity Health Hospitals are paid Fee For Service (except for
outpatient surgery capitation) and receive annual rate increases.
•
Hill Physicians is paid professional services capitation and likely
receive annual rate increases.
•
Physician are incentivized via Hill Physicians Participation
Agreements.
•
All other providers are paid consistent with the Blue Shield of CA
HMO provider agreements.
•
Dignity Health, Blue Shield of California, and Hill Physicians
participate in a 3-Way Risk Share Agreement with a philosophical
commitment to shared risk for all healthcare services.
The Financial Model
9
3 Way Risk Share Agreement
10
The Impact to CalPERS Employees in CY ’10
(Employees see significant Paycheck Savings)
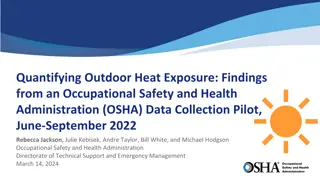
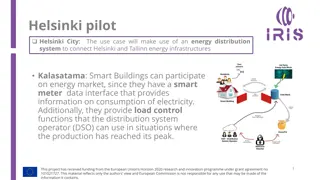
HIE Conceptual Overview
11
Major Findings - IT
A very significant finding is that even advanced HIE (as is
currently defined with orders, results, med lists, CCDs, etc.) is
completely inadequate for a functioning ACO.
Current regulations for Privacy and Security do not fully
take into account changes that need to occur in information
technology and information sharing in order to implement the
model of a functioning ACO.
You’ll note a theme of multiple channels to access
information (e.g., remote EMR access, batch files, HIE) and an
emphasis on workflow optimization.
12
IT Challenges
Physician EMR Adoption Acceptance – Most physicians using HIE portal since they
don’t have an EMR. Physician groups have one HIE solution and the hospital may
another HIE solution.
Current Regulations do not fully anticipate the sharing of information as needed
for real time interventions into medical management and population management
Master Patient Index (MPI) – Hospitals, physicians and payers all have different
patient identifiers. Not common database of ACO members.
Registry Integration - identify all active registries and develop automatic updates
from program enrollment and disenrollment to support seamless patient
communication
Personal Health Record (PHR) - Limited deployment of PHR. Who’s PHR should be
used or should a ‘neutral’ PHR be used?
13
Pilot and CHW Success to Date - IT
Allow multiple hospital to hospital viewing of hospital EMRs
Remote access to hospital EMRs from physician administrative offices
Option for clerical staff to be able to print and fax elements of the clinical record
Shared census information with other organizations
ER data by time of day patient was treated
Real time notification of office staff of patient’s status (admitted or discharged)
Monthly Data dump of all hospital events with other organizations
14
Pilot and CHW Success to Date - HIE
Pre-surgical assessments intended to capture full health condition summaries are
sent from physician to hospital via HIE
Early attempts at intervention were problematic without HIE solution (faxes, etc.)
Sending hospital clinical results, discharge summary and face sheets to physicians
and medical management staff via HIE
Providing real time alerts to PCP when patient is being evaluated in the Emergency
room
Sending hospital Pre-admission Discharge Plan into HIE portal
Early attempts at intervention were problematic without HIE solution (hospitals have no
receptacle until the admission occurs – records are account or event driven)
Access to Health Information Exchange (HIE) for medical management staff
15
16
Blue Shield of
is considering expanding its
Sacramento-based ACO pilot program statewide. The
pilot program—which was launched earlier this year
with
Catholic Healthcare West
and
Hill Physicians
Medical Group
—helps coordinate care for about
38,000 retired government workers who receive
coverage through CalPERS. Project organizers say the
program has led to a 4% drop in hospital admissions,
a 9% reduction in average length of hospital stay and
a 24% decline in readmissions (
Payers & Providers
,
9/30).
“Typical example happened just today. A patient came in
for a 5:30 appointment today in follow up to a hospitalization from
Mercy General where I do not have privileges. He was cared for by
a hospitalist, but nothing has come by fax about his hospitalization
except for a note just today saying he
was admitted. I was able to read in my EMR his history
and physical, his discharge summary, and all his lab data.
I was able to care for his needs efficiently tonight, something
I would not have been able to do without the [mobile EMR] system.
Please continue this. DO NOT EVER
TURN IT OFF.”
– Dr. David Kosh,
Family Physician
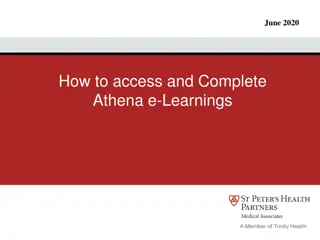
Community Interoperability Results
Care Management/Clinical Efforts
•
Develop CalPERS specific
utilization management
through coordinated operational
infrastructure and clinical processes:
reduce fragmentation and duplication related to
inpatient services through integration of care delivery, processes and data
•
Eliminate unnecessary utilization and non-compliance through personalized
population
management
:
stratify specific member risks to enhance, leverage and integrate disease
management and case management programs
•
Facilitate the rapid and efficient communication of patient medical information through
IT
integration
: adoption and effective use of technologies and tools by all care providers
(physicians, hospital staff, and corporate medical management staff) – all the health care
providers who are working with the target patient population
17
Strategy: Utilization Management
1.
Enhanced inpatient clinical management:
Enhanced prior authorization – define enhanced evidence based guidelines for surgeries
targeting high volume, high cost MSDRG’s
LOS management – actively manage CalPERS Hill admissions through medical hospitalists,
clinical protocols and cross-hospital standardization
Integrated discharge planning
- Implement an aggressive and coordinated pre- and post-
discharge transition management program engaging both CHW and Hill
Dedicated Case Managers for ER Diversion
2.
Medical Access Planning: “
MAP their way home”
– collaborate to quickly move care delivery to
CHW and Hill aligned provider entities when CalPERS members are found to be outside the system
Initiatives
Expected Outcomes
Expected Outcomes:
Reduction in LOS, admissions and readmissions as a result of better patient care
delivered through the establishment and implementation of evidence-based, best
practices and improved, streamlined administrative processes
Reduction in OON spend – in both frequency and duration
18
Strategy: Population Management
1.
Targeted Chronic and Complex Care Management
: actively manage the highest risk and highest
cost patient through synchronized stratification, innovative outreach and coordinated processes
2.
Global Palliative Care
: develop a comprehensive palliative care program across hospital, physician
and care managers to proactively engage members and providers in options for end of life decisions
3.
Chronic Case Management
:
develop a new case management program focused on chronic pain to
reduce ER visits, questionable elective surgeries, and pharmacy costs
4.
Data Collection Process and Integration
: integrate, leverage and enhance participation in available
case and disease management programs through processes, tools (registries), information (phone
numbers) and reporting (non-compliance)
Initiatives
Expected Outcomes:
Better coordination and hand-off between programs, where appropriate, to ensure a
better member experience
Fewer members “falling through the cracks” and not being managed
19
Expected Outcomes
Strategy: IT Integration
1.
Physician Acceptance and Expanded Use of Technology:
increase the adoption and use of
existing technologies to facilitate the rapid and efficient communication of patient medical
information to care providers. Interconnect the organization’s technologies to streamline processes
and support consistent communication. Provide opportunities for two way electronic exchanges.
2.
Master Patient Index (MPI):
identify the appropriate patient identifier to support a common
database of members
3.
Registry Integration:
identify all active registries and develop automatic updates from program
enrollment and disenrollment to support seamless patient communication
4.
Personal Health Record (PHR):
enable patient focused healthcare and personalize care to
empower members with improved member access to information technology
Initiatives
Expected Outcomes
Expected Outcomes:
Strong technological framework to support clinical initiatives and replace manual
processes with automated processes
Limited implementation on initiatives one and two
20
21
Dashboard Element/Utilization
22
•
Hill net membership growth of 960 members
•
Final COHC. $10.15 pmpm or $5M <Target (Facility COHC
$16.54 pmpm <Target)
•
Reductions from CY2009 actual in the following areas:
–
(1%) admits per 1000
–
(14%) days per 1000
–
(15%) average length of stay (from 4.1 to 3.5)
–
(15%) readmissions
CY ’10 Results
CY ’11 Results being Finalized
•
Discharge Planning
•
Case Management / LOS
•
Expanded Health Information Exchange (HIE)
•
Options for robust electronic interchanges in addition to traditional HIE
activities and products (sharing assessments, authorizations and review points)
•
High-risk patient tracking
•
Monthly identify 30-day readmissions and variant days to collaboratively
define root cause and implement process changes
•
Educated hospital and IPA physicians and case managers on palliative care -
Physician Orders for Life-Sustaining Treatment (POLST)
•
Developed a set of comprehensive clinical, quality and financial leading and
lagging measurements
23
24
•
Length of Stay Management is low hanging fruit
•
Invest significantly in Admissions/1000 & Readmission Strategies
•
Develop a Care Management competency relative to benchmarks
•
Develop and use a shared Management Dashboard
•
Consider and communicate the wide range of possible utilization and financial
outcomes.
•
Support the reduction in cost of healthcare through utilization reduction while
negotiating appropriate rate increases.
•
Consider alternative approaches to shared information management
•
Encourage a culture of collaboration through:
•
Aligned, shared risk positions
•
Shared data (multi-lateral reciprocity)
•
Joint management and work tasking
•
Jointly articulate and execute on a path to market share growth at the provider
and plan level
Lessons Learned
The CalPERS Pilot ACO initiative involved Dignity Health, Hill Physicians, and Blue Shield aiming to reduce healthcare costs, enhance collaboration, and improve quality and access to care in Sacramento. The goals were to reduce healthcare costs, attract new members, and create a sustainable model for expansion through virtual integration and continuous improvement.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
CalPERS Pilot ACO Experience & Learnings Scott Whyte, Vice President IT Connectivity Mary Carol Todd, Senior Vice President Clinical Efficiency Steve Foerster, Senior Director Managed Care
Outline Background Virtual Integration & Management Structure The Financial Model IT Connectivity Care Management/Clinical Efforts Lessons Learned Q & A 2
Sacramento Pilot ACO Background Medical Group. The Model: Virtual Integration between 4 Sacramento CHW hospitals, Blue Shield, and Hill Physicians conceived early in CY 07. CalPERS: The California Public Employees Retirement System (CalPERS) provides retirement and health benefits to more than 1.6 million public employees, retirees, and their families. Dignity Health: formerly named Catholic Heathcare West, operates more than 40 hospitals and care centers serving communities across California, Arizona, and Nevada. Blue Shield of California: Blue Shield of California, an indepedent member of the Blue Shield Association, is a not-for-profit health plan dedicated to providing Californians with access to high-quality care at an affordable price. Hill Physicians Medical Group: Hill Physicians is a medical group of more than 3,500 primary care physicians, specialists, sub-specialists, and consultants serving the Northern California region. The Population: ~42,000 CalPERS Members assigned to Hill Physicians 3
CalPERS Pilot ACO Background In 2007, Dignity Health, Hill Physicians, and Blue Shield began planning for the CalPERS Pilot with the following strategic objectives: Reduce the cost of healthcare via care management (utilization) in order to provide a zero percent trend in price to CalPERS while enabling the providers to receive rate increases. Continue the existing CalPERS network in Sacramento. Compete with Kaiser for market share. Enhance collaboration amongst Dignity Health, Hill, and Blue Shield Improve quality and access to care. The Delivery System 4 Dignity Health Sacramento Hospitals Hill Physicians Medical Group Other Blue Shield HMO Contracted Providers 4
ACO Goals Reduce cost of healthcare trend in aggregate for members in the pilot Attract new members Grow Deliver Cost Savings Membership Create Sustainable Model for Expansion Develop way to work together that aligns parties to drive continuous improvement (cost, quality, service) and allows for expansion to other geographic areas 5
The Virtual Integration Vision Vision: Providing affordable healthcare while ensuring the optimal health of members. collaborative approach to healthcare delivery that engages the member as an active participant in their healthcare and supports them in making healthy lifestyle choices. We will achieve our vision through a commitment to quality and an integrated, holistic and Integrated Delivery Network Blue Shield of California Hill Physicians Medical Group Dignity Health integrated processes clinical best practices data integration quality metrics and reporting member and physician engagement Aligned Incentives: each partner contributes to cost savings and together share risk for targeted cost reduction goals 6
Virtual Management Structure Pilot Board Core Team Finance Committee Legal/Contracting Committee Cost Of Health Care Committee w/ Strategy Work Groups (Constant Evolution) Facilities Population Management Electronic Connectivity Physician Variability Pharmacy 7
The Financial Model Dignity Health Hospitals are paid Fee For Service (except for outpatient surgery capitation) and receive annual rate increases. Hill Physicians is paid professional services capitation and likely receive annual rate increases. Physician are incentivized via Hill Physicians Participation Agreements. All other providers are paid consistent with the Blue Shield of CA HMO provider agreements. Dignity Health, Blue Shield of California, and Hill Physicians participate in a 3-Way Risk Share Agreement with a philosophical commitment to shared risk for all healthcare services. 8
3 Way Risk Share Agreement Risk Share Calculation 1/1/12- 12/31/12 Target 1/1/12- 12/31/12 Actual risk allocation % pmpm risk share CHW HPMG BSC CHW HPMG GSC Total Service Categories $xx.xx PMPM$xx.xx PMPM $xx.xx PMPM$xx.xx PMPM $xx.xx PMPM$xx.xx PMPM $xx.xx PMPM$xx.xx PMPM $xx.xx PMPM$xx.xx PMPM $xx.xx PMPM$xx.xx PMPM $xx.xx PMPM$xx.xx PMPM $xx.xx PMPM$xx.xx PMPM Total Facility x% x% x% x% x% x% x% y% y% y% y% y% y% y% z% z% z% z% z% z% z% $xx.xx PMPM$xx.xx PMPM$xx.xx PMPM$xx.xx PMPM $xx.xx PMPM$xx.xx PMPM$xx.xx PMPM$xx.xx PMPM $xx.xx PMPM$xx.xx PMPM$xx.xx PMPM$xx.xx PMPM $xx.xx PMPM$xx.xx PMPM$xx.xx PMPM$xx.xx PMPM $xx.xx PMPM$xx.xx PMPM$xx.xx PMPM$xx.xx PMPM $xx.xx PMPM$xx.xx PMPM$xx.xx PMPM$xx.xx PMPM $xx.xx PMPM$xx.xx PMPM$xx.xx PMPM$xx.xx PMPM CHW Facilities OOA ER (Non-CHW Facilities) All Other Non-CHW Professional Mental Health (capitated) Pharmacy Ancillary Dollars $ $ $ $ 9
The Impact to CalPERS Employees in CY 10 (Employees see significant Paycheck Savings) A B C D E F G State Employees CY 2011 Net Employee Monthly Premium Individual EE + 1 69 $ $ 170 $ $ 106 $ $ 88 $ $ 52 $ $ H I 4 13 14 15 16 17 18 19 20 21 22 23 24 25 46 State Employees CY 2010 Net Employee Monthly Premium Individual EE + 1 55 $ $ 124 $ $ 102 $ $ 94 $ $ 62 $ $ Health Plan Blue Shield Net Value Narrow Network Blue Shield Full Network Kaiser Anthem PERS Choice Anthem PERS Select EE +2 + $ $ $ $ $ EE +2 + $ $ $ $ $ 109 247 203 188 123 140 320 263 243 159 139 341 214 177 106 177 440 274 227 134 Incremental Cost for Employees Blue Shield Full Network vs. Net Value Blue Shield Full Network vs. Kaiser Kaiser vs. Blue Shield Net Value Anthem PERS Choice vs. Net Value Anthem PERS Select vs. Net Value Individual EE + 1 69 $ 22 $ 47 $ 39 $ 7 $ EE +2 + $ $ $ $ $ Individual $ $ $ $ $ EE + 1 $ $ $ $ $ EE +2 + $ $ $ $ $ $ $ $ $ $ 139 44 94 79 14 180 57 123 103 18 101 64 29 19 (17) 202 127 58 38 (33) 263 166 76 49 (43) 10
HIE Conceptual Overview Practice #1 Hospital #1 (Allscripts) CHWMF Hospital #2 Enterprise Master Patient Index Practice #2 Other AEMR Hospital #3 Results / Reports (HL7 Transactions) Results / Reports (HL7 Transactions) HIO A Mercy HIE Hospital #4 HIO B View Results / Reports, Place Outpatient Orders, Submit Practice Documentation Practice #3 No AEMR (Paper) Outpatient Orders, Practice Documentation Hospital #5 CHW Physician Web Access 11
Major Findings - IT A very significant finding is that even advanced HIE (as is currently defined with orders, results, med lists, CCDs, etc.) is completely inadequate for a functioning ACO. Current regulations for Privacy and Security do not fully take into account changes that need to occur in information technology and information sharing in order to implement the model of a functioning ACO. You ll note a theme of multiple channels to access information (e.g., remote EMR access, batch files, HIE) and an emphasis on workflow optimization. 12
IT Challenges Physician EMR Adoption Acceptance Most physicians using HIE portal since they don t have an EMR. Physician groups have one HIE solution and the hospital may another HIE solution. Current Regulations do not fully anticipate the sharing of information as needed for real time interventions into medical management and population management Master Patient Index (MPI) Hospitals, physicians and payers all have different patient identifiers. Not common database of ACO members. Registry Integration - identify all active registries and develop automatic updates from program enrollment and disenrollment to support seamless patient communication Personal Health Record (PHR) - Limited deployment of PHR. Who s PHR should be used or should a neutral PHR be used? 13
Pilot and CHW Success to Date - IT Allow multiple hospital to hospital viewing of hospital EMRs Remote access to hospital EMRs from physician administrative offices Option for clerical staff to be able to print and fax elements of the clinical record Shared census information with other organizations ER data by time of day patient was treated Real time notification of office staff of patient s status (admitted or discharged) Monthly Data dump of all hospital events with other organizations 14
Pilot and CHW Success to Date - HIE Pre-surgical assessments intended to capture full health condition summaries are sent from physician to hospital via HIE Early attempts at intervention were problematic without HIE solution (faxes, etc.) Sending hospital clinical results, discharge summary and face sheets to physicians and medical management staff via HIE Providing real time alerts to PCP when patient is being evaluated in the Emergency room Sending hospital Pre-admission Discharge Plan into HIE portal receptacle until the admission occurs records are account or event driven) Early attempts at intervention were problematic without HIE solution (hospitals have no Access to Health Information Exchange (HIE) for medical management staff 15
Community Interoperability Results Blue Shield of is considering expanding its Sacramento-based ACO pilot program statewide. The pilot program which was launched earlier this year with Catholic Healthcare West and Hill Physicians Medical Group helps coordinate care for about 38,000 retired government workers who receive coverage through CalPERS. Project organizers say the program has led to a 4% drop in hospital admissions, a 9% reduction in average length of hospital stay and a 24% decline in readmissions (Payers & Providers, 9/30). Typical example happened just today. A patient came in for a 5:30 appointment today in follow up to a hospitalization from Mercy General where I do not have privileges. He was cared for by a hospitalist, but nothing has come by fax about his hospitalization except for a note just today saying he was admitted. I was able to read in my EMR his history and physical, his discharge summary, and all his lab data. I was able to care for his needs efficiently tonight, something I would not have been able to do without the [mobile EMR] system. Please continue this. DO NOT EVER TURN IT OFF. Dr. David Kosh, Family Physician 16
Care Management/Clinical Efforts Develop CalPERS specific utilization management through coordinated operational infrastructure and clinical processes: reduce fragmentation and duplication related to inpatient services through integration of care delivery, processes and data Eliminate unnecessary utilization and non-compliance through personalized population management: stratify specific member risks to enhance, leverage and integrate disease management and case management programs Facilitate the rapid and efficient communication of patient medical information through IT integration: adoption and effective use of technologies and tools by all care providers (physicians, hospital staff, and corporate medical management staff) all the health care providers who are working with the target patient population 17
Strategy: Utilization Management Initiatives 1. Enhanced inpatient clinical management: Enhanced prior authorization define enhanced evidence based guidelines for surgeries targeting high volume, high cost MSDRG s LOS management actively manage CalPERS Hill admissions through medical hospitalists, clinical protocols and cross-hospital standardization Integrated discharge planning- Implement an aggressive and coordinated pre- and post- discharge transition management program engaging both CHW and Hill Dedicated Case Managers for ER Diversion 2. CHW and Hill aligned provider entities when CalPERS members are found to be outside the system Medical Access Planning: MAP their way home collaborate to quickly move care delivery to Expected Outcomes Expected Outcomes: Reduction in LOS, admissions and readmissions as a result of better patient care delivered through the establishment and implementation of evidence-based, best practices and improved, streamlined administrative processes Reduction in OON spend in both frequency and duration 18
Strategy: Population Management Initiatives 1. cost patient through synchronized stratification, innovative outreach and coordinated processes Targeted Chronic and Complex Care Management: actively manage the highest risk and highest 2. and care managers to proactively engage members and providers in options for end of life decisions Global Palliative Care: develop a comprehensive palliative care program across hospital, physician 3. reduce ER visits, questionable elective surgeries, and pharmacy costs Chronic Case Management: develop a new case management program focused on chronic pain to 4. case and disease management programs through processes, tools (registries), information (phone numbers) and reporting (non-compliance) Data Collection Process and Integration: integrate, leverage and enhance participation in available Expected Outcomes Expected Outcomes: Better coordination and hand-off between programs, where appropriate, to ensure a better member experience Fewer members falling through the cracks and not being managed 19
Strategy: IT Integration Initiatives 1. existing technologies to facilitate the rapid and efficient communication of patient medical information to care providers. Interconnect the organization s technologies to streamline processes and support consistent communication. Provide opportunities for two way electronic exchanges. Physician Acceptance and Expanded Use of Technology: increase the adoption and use of 2. database of members Master Patient Index (MPI): identify the appropriate patient identifier to support a common 3. enrollment and disenrollment to support seamless patient communication Registry Integration: identify all active registries and develop automatic updates from program 4. empower members with improved member access to information technology Personal Health Record (PHR): enable patient focused healthcare and personalize care to Expected Outcomes Expected Outcomes: Strong technological framework to support clinical initiatives and replace manual processes with automated processes Limited implementation on initiatives one and two 20
CY 10 Results Hill net membership growth of 960 members Final COHC. $10.15 pmpm or $5M <Target (Facility COHC $16.54 pmpm <Target) Reductions from CY2009 actual in the following areas: (1%) admits per 1000 (14%) days per 1000 (15%) average length of stay (from 4.1 to 3.5) (15%) readmissions 22
CY 11 Results being Finalized Discharge Planning Case Management / LOS Expanded Health Information Exchange (HIE) activities and products (sharing assessments, authorizations and review points) Options for robust electronic interchanges in addition to traditional HIE High-risk patient tracking define root cause and implement process changes Monthly identify 30-day readmissions and variant days to collaboratively Physician Orders for Life-Sustaining Treatment (POLST) Educated hospital and IPA physicians and case managers on palliative care - lagging measurements Developed a set of comprehensive clinical, quality and financial leading and 23
Lessons Learned Length of Stay Management is low hanging fruit Invest significantly in Admissions/1000 & Readmission Strategies Develop a Care Management competency relative to benchmarks Develop and use a shared Management Dashboard Consider and communicate the wide range of possible utilization and financial outcomes. Support the reduction in cost of healthcare through utilization reduction while negotiating appropriate rate increases. Consider alternative approaches to shared information management Encourage a culture of collaboration through: Aligned, shared risk positions Shared data (multi-lateral reciprocity) Joint management and work tasking Jointly articulate and execute on a path to market share growth at the provider and plan level 24