Best Practices for Racial Equity Rapid Response Outreach

R
a
c
i
a
l
E
q
u
i
t
y
R
a
p
i
d
R
e
s
p
o
n
s
e
O
u
t
r
e
a
c
h
:
S
u
g
g
e
s
t
e
d
P
r
a
c
t
i
c
e
s
April 30, 2020
Suggested Outreach Workflow
2
Priority
patient list
Outreach team
performs
patient
outreach by phone
Did
patient
answer?
Outreach team
documents
outreach and
returns patient to
work queue
No
Yes
Did
screening
identify
issues?
No
P
a
t
i
e
n
t
i
s
r
e
f
e
r
r
e
d
t
o
c
o
m
m
u
n
i
t
y
r
e
s
o
u
r
c
e
s
a
n
d
/
o
r
p
r
o
v
i
d
e
r
c
a
r
e
t
e
a
m
s
f
o
r
f
o
l
l
o
w
-
u
p
Yes
Outreach team
completes
screening
P
a
t
i
e
n
t
c
o
n
t
i
n
u
e
s
t
o
r
e
c
e
i
v
e
o
u
t
r
e
a
c
h
o
n
a
r
e
g
u
l
a
r
c
a
d
e
n
c
e
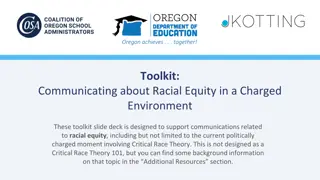
The workflow illustrated below can be customized to align with a provider’s specific
operating model
Priority Patient List: Suggested Criteria
3
F
i
l
t
e
r
f
o
r
a
l
l
p
a
t
i
e
n
t
s
w
i
t
h
p
r
i
o
r
i
t
y
p
r
o
f
i
l
e
:
R
a
c
e
/
E
t
h
n
i
c
i
t
y
o
B
l
a
c
k
o
L
a
t
i
n
X
A
g
e
o
6
5
+
C
h
r
o
n
i
c
u
n
d
e
r
l
y
i
n
g
c
o
n
d
i
t
i
o
n
s
*
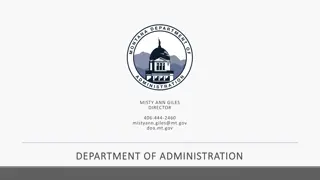
A prioritized list of patients for outreach can be developed by filtering each provider’s patient
population by specific criteria
S
e
l
e
c
t
p
a
t
i
e
n
t
s
i
n
t
o
p
3
-
5
z
i
p
c
o
d
e
s
(
w
i
t
h
h
i
g
h
e
s
t
n
u
m
b
e
r
o
f
p
r
i
o
r
i
t
y
p
a
t
i
e
n
t
s
)
*
*
:
Z
i
p
c
o
d
e
#
1
Z
i
p
c
o
d
e
#
2
Z
i
p
c
o
d
e
#
3
Z
i
p
c
o
d
e
#
4
Z
i
p
c
o
d
e
#
5
P
R
I
O
R
I
T
Y
P
A
T
I
E
N
T
L
I
S
T
F
O
R
O
U
T
R
E
A
C
H
*Underlying conditions include diabetes, hypertension, chronic lung disease, asthma,
heart disease, kidney disease, liver disease, obesity, and immunosuppression
**Once outreach in those top zip codes has been completed, providers move on to patients in other Chicago zip codes and zip codes
outside Chicago.
Note: Sources for patient list may include EMR, Medicare lists, ER visits, etc.
Suggested Components of Screening
4
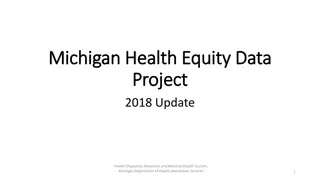
Wellness and chronic medical condition checks are most critical; SDoH screening should be
included, but may be limited
Components of Screening
COVID-19 symptom check
COVID-19 education
o
How to reduce risk of infection
o
Recognizing symptoms
o
Appropriate response to symptoms, including
when/how to contact their PCP
Medication check
o
Refilling chronic medications, including behavioral
health medications
Home management of chronic conditions, e.g.,
o
Supplies: Home BP monitor; glucometer
o
Follow-up: Internet; phone
Screening for depression, anxiety, and
domestic violence
SDoH screening (may be limited)
Sample Comprehensive SDoH Screening
Suggested Roles and Responsibilities
5
O
u
t
r
e
a
c
h
L
e
a
d
Outreach lead is main RERR point of contact and coordinates outreach efforts across teams. As POC, outreach lead
provides regular reporting on agreed-upon metrics, as well as key trends and concerns identified during outreach.
O
u
t
r
e
a
c
h
T
e
a
m
Outreach team – comprised of MAs, care managers, CHWs, care coordinators, etc. – conducts preliminary outreach to
priority patients; once contact has been made, outreach team conducts screening. Based on screening, outreach team
provides patients with referrals to other care team members and connects patients to community resources.
N
u
r
s
i
n
g
T
e
a
m
Nursing team
receives referrals for medication refills and for patients with symptoms who are in need of telehealth or face-
to-face appointments. Nursing team may refer patients to primary care providers and others, particularly for patients who
have hypertension, diabetes, asthma, COPD, and heart disease.
S
o
c
i
a
l
W
o
r
k
T
e
a
m
Social work team receives referrals for
patients who score high for depression or anxiety, or who have very complex needs
that can’t be addressed by the initial caller. Social work team may refer patients to behavioral health providers and others.
Successful implementation of targeted outreach will require collaboration across multiple
care teams, with different roles and responsibilities
Metrics and Reporting
6
Outreach leads provide weekly progress reports* using metrics included in the chart below, in
addition to providing qualitative feedback on key trends and concerns identified during
outreach efforts
*Initial response to confirm participation in program is requested by May 8
th
. Weekly progress reports are requested
every Friday, starting on May 15
th
.
This document outlines suggested practices for a racial equity rapid response outreach program, focusing on a workflow for patient outreach, prioritizing patients based on specific criteria, and components of screening including wellness checks and screening for chronic medical conditions. The workflow involves patient referrals, outreach via phone, screening for issues, documenting outreach efforts, and continuous patient follow-up. Priority patients are identified based on zip codes with high-priority populations and specific demographic and health criteria. Screening components include COVID-19 symptom checks, medication management, home management of chronic conditions, and screening for mental health and domestic violence.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Racial Equity Rapid Response Outreach: Suggested Practices April 30, 2020
Suggested Outreach Workflow The workflow illustrated below can be customized to align with a provider s specific operating model Additional detail provided in following slides Did Patient is referred to community resources and/or provider care teams for follow-up Outreach team performs patient outreach by phone Did patient answer? Outreach team completes screening screening identify issues? Priority patient list Yes Yes No No Outreach team documents outreach and returns patient to work queue Patient continues to receive outreach on a regular cadence 2
Priority Patient List: Suggested Criteria A prioritized list of patients for outreach can be developed by filtering each provider s patient population by specific criteria Select patients in top 3-5 zip codes (with highest number of priority patients)**: Filter for all patients with priority profile: Race/Ethnicity o Black o LatinX Age o 65+ Chronic underlying conditions* PRIORITY PATIENT LIST FOR OUTREACH Zip code #1 Zip code #2 Zip code #3 Zip code #4 Zip code #5 *Underlying conditions include diabetes, hypertension, chronic lung disease, asthma, heart disease, kidney disease, liver disease, obesity, and immunosuppression **Once outreach in those top zip codes has been completed, providers move on to patients in other Chicago zip codes and zip codes outside Chicago. 3 Note: Sources for patient list may include EMR, Medicare lists, ER visits, etc.
Suggested Components of Screening Wellness and chronic medical condition checks are most critical; SDoH screening should be included, but may be limited Components of Screening Sample Comprehensive SDoH Screening COVID-19 symptom check COVID-19 education o How to reduce risk of infection o Recognizing symptoms o Appropriate response to symptoms, including when/how to contact their PCP Medication check o Refilling chronic medications, including behavioral health medications Home management of chronic conditions, e.g., o Supplies: Home BP monitor; glucometer o Follow-up: Internet; phone Screening for depression, anxiety, and domestic violence SDoH screening (may be limited) 4
Suggested Roles and Responsibilities Successful implementation of targeted outreach will require collaboration across multiple care teams, with different roles and responsibilities Outreach Lead Outreach lead is main RERR point of contact and coordinates outreach efforts across teams. As POC, outreach lead provides regular reporting on agreed-upon metrics, as well as key trends and concerns identified during outreach. Outreach Team Outreach team comprised of MAs, care managers, CHWs, care coordinators, etc. conducts preliminary outreach to priority patients; once contact has been made, outreach team conducts screening. Based on screening, outreach team provides patients with referrals to other care team members and connects patients to community resources. Nursing Team Nursing team receives referrals for medication refills and for patients with symptoms who are in need of telehealth or face- to-face appointments. Nursing team may refer patients to primary care providers and others, particularly for patients who have hypertension, diabetes, asthma, COPD, and heart disease. Social Work Team Social work team receives referrals for patients who score high for depression or anxiety, or who have very complex needs that can t be addressed by the initial caller. Social work team may refer patients to behavioral health providers and others. 5
Metrics and Reporting Outreach leads provide weekly progress reports* using metrics included in the chart below, in addition to providing qualitative feedback on key trends and concerns identified during outreach efforts As of MM/DD/YY Total By Race/Ethnicity By Zip Code (Top 3-5 zip codes for priority patients) Black LatinX Zip Code #1 Zip Code #2 Zip Code #3 Zip Code #4 Zip Code #5 # of Patients on Priority List # of Patients Reached (Cumulative) *Initial response to confirm participation in program is requested by May 8th. Weekly progress reports are requested every Friday, starting on May 15th. 6