South San Antonio ISD 2020-2021 Benefits Enrollment

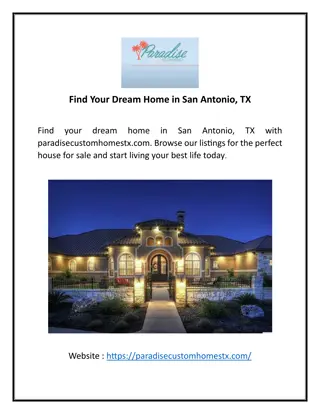
South San Antonio ISD is offering Aetna/HEB Rx Plan Options for the 2020-2021 benefits enrollment. Option 1 includes Aetna Whole Health ACO Baptist Providers, while Option 2 is a POS plan. Both options outline coverage details including deductibles, out-of-pocket maximums, physician services, hospital visits, emergency care, prescription drug coverage, and more.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
South San Antonio ISD 2020 - 2021 Benefits Enrollment 1
Aetna / HEB Rx Plan Benefits Option 1 Aetna Whole Health ACO Baptist Providers (Tier 1) 100% General All other Aetna network (Tier 2) Out-of-Network Preventive Care Services Calendar Year Deductible Individual Family (Embedded) Hospital Admission- Inpatient Coinsurance % Out-of-Pocket Maximum: Individual Family Policy Maximum Physician Services: Primary Care Physician: Office Co-pays Specialist / Urgent Care: Office Co-pays 100% N/A N/A N/A N/A N/A N/A N/A N/A N/A $5,000 $10,000 $5,000 $10,000 85% after deductible 85% 65% after deductible 65% $6,350 $12,700 Unlimited $6,350 $12,700 Unlimited $35 copay $70/$100 copay $35 copay $70/$100 copay $250 copay; deductible waived Covered 100%, deductible waived $35 PCP $70 Specialist 65% after deductible $70 copay N/A N/A $250 copay; deductible waived Hospital Visits Emergency Room Service $250 copay; ded. waived Maternity Prenatal Care 100%; ded. waived N/A Allergy Injections $35 PCP/$70 Specialist N/A In-Patient Psych. Out-Patient Psych. Hospital Services: Room & Board Inpatient Services Surgery Hospital Services- Out Patient: Surgery Emergency - Facility Emergency - Physician Other Services: Home Health Care Hospice Care Ambulance- Emergency Medical Transportation Diagnostic X-ray & Lab, PET,MRI, Pharmacy (ESI) Prescription Drug Coverage Mail Order Pharmacy 85% after deductible $70 copay N/A N/A 85% after deductible 85% after deductible 65% after deductible 65% after deductible N/A N/A 85% after deductible $250 copay; ded. waived 80% after deductible 65% after deductible $250 copay; ded. waived 80% after deductible N/A $250 copay; ded. waived N/A 85% after deductible 100% ; ded. waived 85% after deductible 85% after deductible In-Network $15/$35/$70 $37.50/$87.50/$175 65% after deductible 100%; ded. waived 85% after deductible 65% after deductible N/A N/A N/A N/A N/A N/A N/A 2
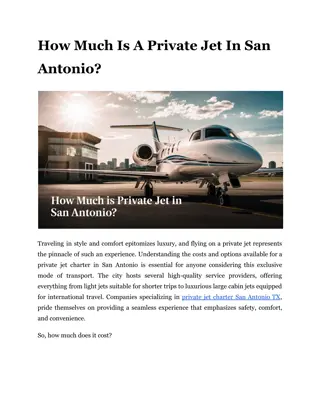
Aetna / HEB Rx Aetna Option 2 POS Plan Benefits In-Network 100% Out-of-Network General Preventive Care Services Calendar Year Deductible Individual Family (Embedded) Hospital Admission- Inpatient Coinsurance % Out-of-Pocket Maximum: Individual Family Policy Maximum Physician Services: Primary Care Physician: Office Co-pays Specialist / Urgent Care: Office Co-pays Hospital Visits Emergency Room Service $6,000 $12,000 $10,000 $30,000 80% after deductible 80% 50% after deductible 50% $7,150 $14,300 NA $13,000 $39,000 NA $40 copay $60/$100 copay 80% after deductible Covered 100%, deductible waived $40 PCP $60 Specialist 80% after deductible $40 copay 50% after deductible 50% after deductible 50% after deductible 50% after deductible Maternity Prenatal Care Allergy Injections 50% after deductible In-Patient Psych. Out-Patient Psych. Hospital Services: Room & Board Inpatient Services Surgery Hospital Services- Out Patient: Surgery Emergency - Facility Emergency - Physician Other Services: Home Health Care Hospice Care Ambulance- Emergency Medical Transportation Diagnostic X-ray & Lab, PET,MRI, Pharmacy (ESI) Prescription Drug Coverage Mail Order Pharmacy 50% after deductible 50% after deductible 80% after deductible 80% after deductible 50% after deductible 50% after deductible 80% after deductible 80% after $250 copay; ded. waived 80% after deductible 50% after deductible 80% after $250 copay; ded. waived 50% after deductible 80% after deductible 100%, ded. waived 80% after deductible 80% after deductible In-Network $20/$50/$80 $50/$125/$200 50% after deductible 70% after deductible 80% after deductible 70% after deductible Out of network No coverage NA 3
Aetna / HEB Rx Aetna Option 3 POS Plan Benefits In-Network Out-of-Network General 100% Preventive Care Services Calendar Year Deductible Individual Family (Embedded) Hospital Admission- Inpatient Coinsurance % Out-of-Pocket Maximum: Individual Family Policy Maximum Physician Services: Primary Care Physician: Office Co-pays Specialist / Urgent Care: Office Co-pays Hospital Visits Emergency Room Service $3,000 $6,000 $5,000 $10,000 80% after deductible 80% 50% after deductible 50% $6,000 $12,000 NA $10,000 $20,000 NA $35 copay $45/$75 copay 80% after deductible Covered 100%, deductible waived $35 PCP $45 Specialist 80% after deductible $35 copay 50% after deductible 50% after deductible 50% after deductible 50% after deductible Maternity Prenatal Care 50% after deductible Allergy Injections In-Patient Psych. Out-Patient Psych. Hospital Services: Room & Board Inpatient Services Surgery Hospital Services- Out Patient: Surgery Emergency - Facility Emergency - Physician Other Services: Home Health Care Hospice Care Ambulance- Emergency Medical Transportation Diagnostic X-ray & Lab, PET,MRI, Pharmacy (ESI) Prescription Drug Coverage Mail Order Pharmacy 50% after deductible 50% after deductible 80% after deductible 80% after deductible 50% after $250/admission ded. 50% after deductible 80% after deductible 80% after $200 copay; ded. waived 80% after deductible 50% after deductible 80% after $200 copay; ded waived 80% after deductible 80% after deductible 100%, ded. waived 80% after deductible 80% after deductible In-Network $25/$45/$80 $62.50/$112.50/$200 50% after deductible 70% after deductible 80% after deductible 70% after deductible Out of network No Coverage NA 4
MEDICAL EMPLOYEE PLAN PREMIUMS Base Plan: Option 1 Mid Plan: Option 2 High Plan: Option 3 2020-2021 Premium 2020-2021 Premium 2020-2021 Premium Monthly Bi-Weekly Monthly Bi-Weekly Monthly Bi-Weekly $0 $0 $65 $32.50 $240 $120 EE $284 $142 $430 $215 $1124 $562 EE/SP $212 $106 $335 $167.50 $985 $492.50 EE/CH $495 $247.50 $735 $367.50 $1562 $781 EE/FM SSAISD will contribute $402 towards all 3 group medical plans beginning November 2020.
VISION EMPLOYEE PREMIUM PLAN COMPARISON 2020- 2021 Low Plan Mid Plan High Plan Monthly Bi-Weekly Monthly Bi-Weekly Monthly Bi-Weekly $5.90 $2.95 $9.80 $4.90 $11.00 $5.50 EE $11.00 $5.50 $19.00 $9.50 $21.08 $10.54 Employee + 1 Dep. Employee + 2 or more $17.00 $8.50 $29.00 $14.50 $32.34 $16.17
DENTAL EMPLOYEE PREMIUMS 2020 - 2021 Dental Plan HIGH Plan Monthly Bi-Weekly $27.11 $13.56 EE Employee+ 1 Dependent $59.39 $29.70 $85.62 $42.81 Employee + 1 Family Dental Plan L Plan Monthly Bi-Weekly $19.36 $9.68 EE Employee+ 1 Dependent $38.33 $1917 $60.48 $30.24 Employee + 1 Family
Other Voluntary Benefits Accident Cancer Voluntary Term Life Disability Hospital Indemnity Heart & Stroke Plan Life Insurance (Term/Whole) Disability Income Protection Flexible Spending Account For more information visit the District Webpage: https://www.southsanisd.net/VOLUNTARYBENEFITS