Long COVID and Disability Research Program: Empowering Patients through Data



Long COVID, Disability, and
All of Us
Research Program
Lisa McCorkell, MPP
Cofounder of Patient-Led Research Collaborative

Our Team
(all with Long COVID and associated conditions)
●
Jointly co-led by
seven
women
●
50+ patient-researchers and advocates across 10 countries (US, Brazil, Canada, India, UK, Italy, Egypt,
Cyprus, Mexico, Australia).
●
26% of PLRC members identified as LGBTQ+
●
61% are women, 26% men, 13% another gender
●
26% are people of color
●
70% identified as disabled, additional 17% identifying as episodically disabled

Our
Work
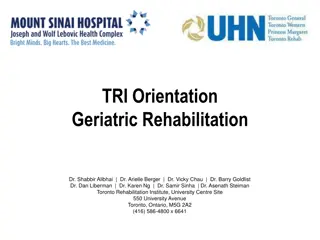
Demographics
Currently experiencing Long COVID, as a percentage of all adults (from CDC Household
Pulse Survey)
Age:
Race:
Gender:
Pre-existing Disability:
Impact of Long COVID
●
Additional risk factors: lower income and inability to rest in first two weeks
(Williamson,
A.E., et al.
BMJ Open
; Ziauddeen, N., et al. 2022.
Plos One
.)
●
Up to 4 million out of work in US as of Jan 2022
(Bach, K. 2022.
Brookings
.)
●
1 in 4 limit activities outside of work to continue working
(Karpman, M. 2023. Urban Institute)
○
Childcare, chores, errands, hobbies
●
Decreased quality of life
○
Even socializing, listening to music, watching TV
●
42% report food insecurity
(Karpman, M. 2023.
Urban Institute
);
twice as likely to experience
housing insecurity
(Packard, S. 2023.
medRxiv
)
●
Increased medical costs -
estimated average of $8,731/year
(Cutler 2022)
●
Lack of clinical care – only 7% of providers are very confident diagnosing LC; 4%
very confident treating the condition
(de Beaumont 2023)
○
When we do not have FDA-approved treatment for Long COVID, having access to care is still important
for accessing disability benefits, SNAP, work accommodations, etc. and for some symptom
management, largely learning from conditions like ME/CFS and POTS and/or patient anecdote
Importance of participating in research on Long COVID
●
Recruitment can be very time intensive
●
Learning more about your own illness
●
Helping the community at large, getting us to answers faster
●
Your hypotheses and input on study design makes research more effective and efficient
Risks/downsides:
●
surveys, tests, travel, exam rooms can trigger post-exertional malaise
●
side effects from new treatment or getting placebo
●
time and money constraints
●
COVID reinfection
Key Points to Consider in Long COVID research
●
Build off existing infection-associated chronic condition research
●
Conduct
cross-illness research
; include cohorts of people with ME/CFS, POTS, etc.; measure who in your LC
cohorts have these conditions
●
Create a
safe environment
(e.g. masking, virtual when possible, rooms for rest)
●
Need comprehensive selection of patients:
○
Most LC patients were not hospitalized; many had mild acute cases; never had low oxygen levels
;
many
didn’t experience respiratory symptoms
○
Many were not PCR positive/antibody positive (must at least include clinical diagnosis subset)
○
Reflective of populations most impacted – consider gender, sex, race, socioeconomic status, age
●
Account for the
nature of the illness
in study design
. Patient engagement helps ensure of this
○
Post-exertional malaise
– are you triggering PEM? When are you taking samples?
○
Exacerbation around menstrual cycle & hormonal impact
– track where people are in menstrual cycle
○
Be careful with questionnaires
– anxiety/depression need mood component
○
Illness duration
– conduct analyses by illness duration
○
Phenotypes
– ongoing but can separate out by diagnoses, symptom clusters to start as sensitivity
analysis
○
What
treatments
patients are on – is that impacting results?
Patient-Led Research
Scorecards
https://cmss.org/patient-led-research-integration/
Patient Burden Scorecard
Integration into Research
Process Scorecard
Thank You
Thank you!
Contact our team:
team@patientledresearch.com
Contact me:
lisa@patientledresearch.com
The Long COVID and Disability Research Program, led by a diverse team of patient-researchers, has made significant contributions to understanding Long COVID's impact and informing public health guidelines and policy. Their work has shed light on the demographics affected by Long COVID, highlighting additional risk factors and the profound impact on individuals' lives. The program emphasizes the importance of access to care for managing symptoms and accessing support services.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Long COVID, Disability, and All of Us Research Program Lisa McCorkell, MPP Cofounder of Patient-Led Research Collaborative
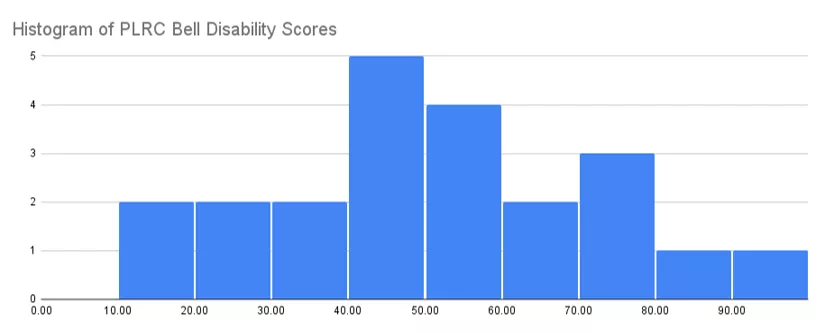
Our Team (all with Long COVID and associated conditions) Jointly co-led by seven women 50+ patient-researchers and advocates across 10 countries (US, Brazil, Canada, India, UK, Italy, Egypt, Cyprus, Mexico, Australia). 26% of PLRC members identified as LGBTQ+ 61% are women, 26% men, 13% another gender 26% are people of color 70% identified as disabled, additional 17% identifying as episodically disabled Wide range of disability severity; average score of 46 on the Bell Disability Scale
Our Work 21 PAPERS IN 4 YEARS 1000+ RESEARCH CITATIONS 6 patient-led papers, including an international study with 8,000+ Long COVID participants from 80+ countries in 9 languages. 15 co- authored papers with Yale, Scripps Institute, WHO, National COVID Cohort Collaborative, University of Toronto, Imperial College London, UCL. Authored two of the most cited Long COVID research papers. Over 1.1 million downloads; contributing to medical education. PUBLIC HEALTH GUIDELINES Co-created WHO Clinical Case Definition, CDC Long COVID guidelines, American Academy of Physical Medicine & Rehabilitation guidelines, influenced NIH $1.15Bfunding, & others. POLICY DOCUMENTS Our papers informed policy in the US, UK, Belgium, Spain, Council of the European Union, World Health Organization, & others.
Demographics Currently experiencing Long COVID, as a percentage of all adults (from CDC Household Pulse Survey) Age: Race: Gender: Hispanic or Latino Cis-gender male 8.5% 5.0% 18 -29 years 6.9% Non-Hispanic White, single race Cis-gender female 7.1% 8.8% 30 -39 years 7.2% Transgender 12.5% 40 -49 years 8.1% Non-Hispanic Black, single race 4.4% Pre-existing Disability: 50 -59 years 7.4% With disability Non-Hispanic Asian, single race 14.1% 3.6% 60 -69 years 6.2% Without disability 5.9% 70 -79 years 5.3% Non-Hispanic, other races and multiple races 7.0% 80 years and above 4.3%
Impact of Long COVID Additional risk factors: lower income and inability to rest in first two weeks (Williamson, A.E., et al. BMJ Open; Ziauddeen, N., et al. 2022.PlosOne.) Up to 4 million out of work in US as of Jan 2022 (Bach, K. 2022. Brookings.) 1 in 4 limit activities outside of work to continue working (Karpman, M. 2023. Urban Institute) Childcare, chores, errands, hobbies Decreased quality of life Even socializing, listening to music, watching TV 42% report food insecurity (Karpman, M. 2023. Urban Institute); twice as likely to experience housing insecurity (Packard, S. 2023. medRxiv) Increased medical costs -estimated average of $8,731/year (Cutler 2022) Lack of clinical care only 7% of providers are very confident diagnosing LC; 4% very confident treating the condition (de Beaumont 2023) When we do not have FDA-approved treatment for Long COVID, having access to care is still important for accessing disability benefits, SNAP, work accommodations, etc. and for some symptom management, largely learning from conditions like ME/CFS and POTS and/or patient anecdote
Importance of participating in research on Long COVID Recruitment can be very time intensive Learning more about your own illness Helping the community at large, getting us to answers faster Your hypotheses and input on study design makes research more effective and efficient Risks/downsides: surveys, tests, travel, exam rooms can trigger post-exertional malaise side effects from new treatment or getting placebo time and money constraints COVID reinfection
Key Points to Consider in Long COVID research Build off existing infection-associated chronic condition research Conduct cross-illness research; include cohorts of people with ME/CFS, POTS, etc.; measure who in your LC cohorts have these conditions Create a safe environment (e.g. masking, virtual when possible, rooms for rest) Need comprehensive selection of patients: Most LC patients were not hospitalized; many had mild acute cases; never had low oxygen levels;many didn t experience respiratory symptoms Many were not PCR positive/antibody positive (must at least include clinical diagnosis subset) Reflective of populations most impacted consider gender, sex, race, socioeconomic status, age Account for the nature of the illness in study design. Patient engagement helps ensure of this Post-exertional malaise are you triggering PEM? When are you taking samples? Exacerbation around menstrual cycle & hormonal impact track where people are in menstrual cycle Be careful with questionnaires anxiety/depression need mood component Illness duration conduct analyses by illness duration Phenotypes ongoing but can separate out by diagnoses, symptom clusters to start as sensitivity analysis What treatmentspatients are on is that impacting results?
Thank you! Contact our team: team@patientledresearch.com Contact me: lisa@patientledresearch.com