Improving Access to Malaria Control Services in Odisha through Community Volunteers


Improving access to malaria control services at
community level through the community
volunteers :
Accredited Social Health Activist (ASHA) & Others



Presentation by:
Dr M M Pradhan
Jt. Director, NVBDCP, Odisha
ODISHA
Odisha- at a glance
Area:
•
156,000 sq. km. (4% of India’s land
area)
•
34% forest areas
•
Diverse ecology
•
Rapid urbanization &
industrialization
Population:
•
44 million (3% of India’s total
population)
•
Rural- 82%; Urban- 18%
•
ST- 22%; SC- 16 %
Reported malaria cases:
•
0.4 million (26% of the country)
Health Infrastructure in Odisha
29 SDH
Malaria Problem
•
Hilly, forest, forest fringed areas
•
Favourable climate and geo-ecotypes,
•
Complex vector bionomic and High falciparum proportion ( >90%)
Stratification of districts-based on API, 2016
Source: Epidemiological data of Odisha , 2016
•
8 coastal
districts are
very low
endemic
(API<0.5).
•
Population-
27% of state’s
pop. (1.12
crore)
Function of community volunteers (ASHA and others) in
Malaria control activities
Under NVBDCP (central sponsored under
NHM)
•
Early Diagnosis and Complete treatment
(EDCT)
•
Vector Control Interventions (Long
Lasting Insecticidal Net (LLIN and Indoor
Residual Spray)
•
IEC/ BCC/ IPC
State specific
•
DAMaN
– Special activities in
inaccessible villages
•
Special IEC – BCC campaign (under
MDD)
and LLIN specific (
Nidhi Ratha
campaign)
Capacity Building of ASHAs by the State
•
2007: ASHAs were trained as Fever
Treatment Depot (FTD) for diagnosis and
treatment of malaria cases with
Appropriate Anti-malaria drugs
•
In 2007 around 30000 ASHAs and 2016
more than 45, 000 ASHAs are trained
and engaged as FTD
•
2010- Started with Mono-valent RDT
and shifted to use bivalent RDT for use
at point of contact in community.
•
Strict alignment to National guidelines
(for drug, diagnosis, and record keeping)
for capacity building of ASHAs
ASHA conducting RDT
Champion ASHA appraised by Hon’ble
PM
EDCT by ASHA & Community Volunteers at far-off hamlets
•
ASHA- the first point of contact for malaria
diagnosis and treatment at the village level.
•
ASHA is involved in the community platform
(Gaon Kalyan Samiti /Village Health Sanitation
and Nutrition Committee) for malaria
programme related and other activities.
•
ASHA links with AWW and non-ASHA
volunteers engaged for malaria service in
remote areas.
•
Approximately 3000 Non-ASHA community
volunteers trained in EDCT in hard-to-reach
areas– supported by respective ASHA.
•
Non ASHA volunteers are supported by the
programme (incentive based) and by CARITAS
India consortium and TATA Trust
•
Principal investigators: NIMR,
NVBDCP – Odisha
•
Support: MMV&WHO
•
Project areas :4 intervention and 4
control blocks each in four districts
of different malaria endemicity
•
Diagnosis and treatment by ASHA
(473) alternative volunteers (239)
in all villages
•
ASHA ensure completion of
treatment by following up patients
diagnosed by her as well as by
other higher facility
•
ASHAs are trained
to identify PQ-
related haemolytic adverse events
Comprehensive Case Management Project (CCMP) in Odisha
Improved access to 3Ts: test, treat, & track
Addressing Malaria in VHND sessions
•
Guidelines have been rolled out by state
to
address Malaria in vulnerable population
groups (pregnant mothers and under-5
children) in monthly Village Health & Nutrition
Day (VHND) sessions.
•
VHND is conducted at
Anganwadi Centre.
•
VHND -
once in a month (TUESDAY or FRIDAY)
•
Malaria screening
is being done in VHND
sessions by
bivalent RDT
.
•
Malaria positive cases are
treated with
appropriate Antimalarials.
•
Counseling
for regular use of LLIN/ITN
•
HW(F), ASHA, AWW play crucial role
•
In 2015-16, a total
3067411 PW attended
VHND sessions and
178294 with fever have
been tested for malaria
(58%)
•
Malaria positive rate :
<3%.
Role of ASHA
•
Mobilizing pregnant women, lactating
mothers and under-5 children to VHND
session
•
Conducting mandatory malaria
screening using bi-valent RDT.
•
Treatment of positive cases as per
national guideline.
•
Follow up for treatment adherence &
any complication.
–
Counseling for better acceptance &
utilization of vector control
interventions
Role of ASHA in VHND Sessions For Malaria Prevention &
Management
Role of ASHA in LLIN Distribution In Community
Engages through GKS platform
Conducts Household survey
Distributes advance information slip
During distribution along with AWW and ward
member conducts coding
Demonstrate how to use LLIN at distribution
venue
Maintains LLIN register
Writes on the village health wall bulletin
(“Swasthy Kanth”)
Role of ASHA in scaling-up the use of LLIN
•
Organizing meetings for the villagers on LLIN
distribution and use
•
Folk arts and different IEC & BCC activities
•
Counseling to increase use
•
Night time monitoring
Role of ASHA in Malaria, Dengue and Diarrhoea (MDD)
Campaign
MDD is state funded activity to create
awareness on outbreak prone monsoon
influenced diseases- Malaria Dengue and
Diarrhoea.
Role of ASHA
•
Coordination with School
•
Delivering awareness messages
•
Engaging in Different IEC activities, e.g.
Nidhi Rath Campaign
•
Mobilizing community and increasing
participation of children
Role of ASHA in implementation of Indoor Residual
Spray (IRS)
•
Advance intimation to the
households regarding date and
time of spray
•
Counselling to increase
community acceptance
•
Accompanying the spray squad
during spray operation
•
Addressing the refusal cases
•
Household counselling on Do’s
and Don’ts regarding IRS
Problem of Inaccessibility in Hard-to-reach Areas
•
Inaccessible especially during transmission season in monsoon
hindering service delivery when it is most needed.
•
Non-availability of modern transport mechanism throughout the year
hindering referral.
•
Community is mostly tribal, marginalized and have poor literacy rate-
challenges of poverty, treatment seeking from informal healers, low
malaria awareness.
•
It is observed that in theses areas, around 20% of malaria cases in
these areas are asymptomatic.
DAMaN – Access the Inaccessible
Model initiative
by the
State of Odisha
from 2017
. FIRST OF ITS KIND IN INDIA.
Implementation through
camp approach
- two rounds annually.
Vulnerable centric approach.
ASHA, AWW and other community
volunteers and PRI members
are
involved.
Package of activities:
•
Mass malaria screening (both
symptomatic and asymptomatic).
•
Treating of all malaria positive cases.
•
Haemoglobin estimation of
Pregnant & lactating mothers
Growth assessment of
under-5 children.
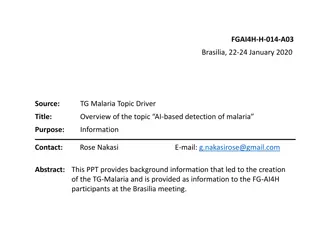
Impact of Different Malaria Control Interventions
N
e
w
i
n
p
u
t
s
:
R
D
T
&
L
L
I
N
B
i
v
a
l
e
n
t
R
D
T
&
2
n
d
P
h
a
s
e
L
L
I
N
Increased surveillance and complete treatment.
Proportionately, Case fatality rate is at lower level.
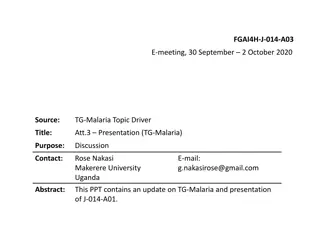
Program Outcome due to ASHA involvement
•
Deaths reduced by 187% in 2016
compared to 2007 in spite of increase in
case detection.
•
Around 40 lakh LLINs could be distributed
smoothly through ASHAs- GKS mechanism
during 2010-2012 . This resulted
reduction of malaria incidence and deaths
by 73.54 % and 268.7% respectively in
2013 compared to 2010.
•
Early diagnosis and complete treatment,
mass screening in hard to reach areas and
Tribal Residential Schools averted
outbreaks
In 2017, >11.34 million LLINs are being distributed under GFATM support - already 7 million
have been distributed through ASHA- GKS mechanism within 2 months and most difficult
pockets have been protected before cut off by rains.
Increase in Passive Surveillance- ABER
increase from 12.24% in 2007 to 16.37%
in 2016
Scalability and Opportunity
•
Capacity Building:
With enhanced capacity building and increased nos. of
ASHAs/ other community volunteers in remote villages/ hamlets,
surveillance and EDCT services can be further improved.
•
Inclusive Approach:
Health NGOs and other players can support
community volunteers in remote inaccessible hamlets and service delivery
can be scaled up through inclusive approach.
•
Scale up of best practices:
The mass screening and simultaneous vector
control under DAMaN can avert deaths and lower malaria transmission
rate.
•
Inter-sectoral Coordination:
Convergence with other sectors, including
sanitation, tribal affairs, rural development, women & child development
etc. can add value to DAMaN efforts for alleviation of the problems of
malaria and malnutrition
Community Volunteers
remains critical in malaria
control/elimination
THANK YOU FOR KIND
ATTENTION
“End Malaria for Good”
Odisha faces a significant malaria burden, with a high proportion of cases reported in hilly and forested areas. The state's health infrastructure includes a network of medical facilities and community health centers. To combat malaria, community volunteers, including Accredited Social Health Activists (ASHAs), play a crucial role in early diagnosis, treatment, and vector control interventions. Capacity building initiatives have empowered ASHAs to effectively contribute to malaria control efforts in the state.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
ODISHA Improving access to malaria control services at community level through the community volunteers : Accredited Social Health Activist (ASHA) & Others Presentation by: Dr M M Pradhan Jt. Director, NVBDCP, Odisha
Odisha- at a glance Area: 156,000 sq. km. (4% of India s land area) 34% forest areas Diverse ecology Rapid urbanization industrialization Population: 44 million (3% of India s total population) Rural- 82%; Urban- 18% ST- 22%; SC- 16 % Reported malaria cases: 0.4 million (26% of the country) &
Health Infrastructure in Odisha Odisha- Medical Colleges-9 32 Districts- 30 DHs & 2 Capital Hospitals 314 Blocks- 377 CHCs 29 SDH PHCs- 1236 SCs- 6688 51,000 villages (no. of ASHAs- 47294; 45230 ASHAs are trained in malaria)
Malaria Problem Hilly, forest, forest fringed areas Favourable climate and geo-ecotypes, Complex vector bionomic and High falciparum proportion ( >90%)
Stratification of districts-based on API, 2016 Rayagada 70.32 Malkangiri 60.78 Kandhamal 38.15 Koraput 29.36 Kalahandi 28.60 Keonjhar 19.29 Nawarangpur 19.14 Malaria burden No. of Dists No. of CHCs Gajpati 18.71 Sundargarh 13.74 2015 2016 2015 2016 Sambalpur 13.61 Angul 12.90 API 10 14 13 105 122 Deogarh 11.21 State 10.24 Mayurbhanj 10.15 Nuapada 8.77 API 5-<10 3 4 33 48 8 districts very endemic (API<0.5). Population- 27% of state s pop. crore) coastal are low Boudh 8.50 Bolangir 5.28 Sonepur 5.26 API 2- <5 5 4 55 47 Nayagarh 4.34 Ganjam 3.18 Jharsuguda 2.66 Bargarh 2.29 API 1- <2 0 1 49 29 Dhenkanal 1.17 Jajpur 0.41 Khurda 0.32 API < 1 8 8 122 121 Bhadrak 0.26 Balasore 0.25 (1.12 Cuttack 0.23 Puri 0.16 J.S PUR 0.13 Source: Epidemiological data of Odisha , 2016 Kendrapada 0.10 0.00 10.00 20.00 30.00 40.00 50.00 60.00 70.00 80.00
Function of community volunteers (ASHA and others) in Malaria control activities Under NVBDCP (central sponsored under NHM) Early Diagnosis and Complete treatment (EDCT) Vector Control Interventions (Long Lasting Insecticidal Net (LLIN and Indoor Residual Spray) IEC/ BCC/ IPC State specific DAMaN Special inaccessible villages Special IEC BCC campaign (under MDD) and LLIN specific (Nidhi Ratha campaign) activities in
Capacity Building of ASHAs by the State 2007: ASHAs were trained as Fever Treatment Depot (FTD) for diagnosis and treatment of malaria cases with Appropriate Anti-malaria drugs In 2007 around 30000 ASHAs and 2016 more than 45, 000 ASHAs are trained and engaged as FTD 2010- Started with Mono-valent RDT and shifted to use bivalent RDT for use at point of contact in community. Strict alignment to National guidelines (for drug, diagnosis, and record keeping) for capacity building of ASHAs ASHA conducting RDT Champion ASHA appraised by Hon ble PM
EDCT by ASHA & Community Volunteers at far-off hamlets ASHA- the first point of contact for malaria diagnosis and treatment at the village level. ASHA is involved in the community platform (Gaon Kalyan Samiti /Village Health Sanitation and Nutrition Committee) programme related and other activities. ASHA links with AWW and non-ASHA volunteers engaged for malaria service in remote areas. Approximately 3000 Non-ASHA community volunteers trained in EDCT in hard-to-reach areas supported by respective ASHA. Non ASHA volunteers are supported by the programme (incentive based) and by CARITAS India consortium and TATA Trust for malaria
Comprehensive Case Management Project (CCMP) in Odisha Improved access to 3Ts: test, treat, & track Principal NVBDCP Odisha Support: MMV&WHO Project areas :4 intervention and 4 control blocks each in four districts of different malaria endemicity Diagnosis and treatment by ASHA (473) alternative volunteers (239) in all villages ASHA ensure treatment by following up patients diagnosed by her as well as by other higher facility ASHAs are trained to identify PQ- related haemolytic adverse events investigators: NIMR, completion of
Addressing Malaria in VHND sessions Guidelines have been rolled out by state to address Malaria in vulnerable population groups (pregnant mothers and under-5 children) in monthly Village Health & Nutrition Day (VHND) sessions. VHND is conducted at Anganwadi Centre. VHND - once in a month (TUESDAY or FRIDAY) Malaria screening is being done in VHND sessions by bivalent RDT. Malaria positive cases are treated with appropriate Antimalarials. Counseling for regular use of LLIN/ITN HW(F), ASHA, AWW play crucial role In 3067411 PW attended VHND sessions 178294 with fever have been tested for malaria (58%) Malaria positive rate : <3%. 2015-16, a total and
Role of ASHA in VHND Sessions For Malaria Prevention & Management Role of ASHA Mobilizing pregnant women, lactating mothers and under-5 children to VHND session Conducting mandatory screening using bi-valent RDT. Treatment of positive cases as per national guideline. Follow up for treatment adherence & any complication. Counseling for better acceptance & utilization of interventions malaria vector control
Role of ASHA in LLIN Distribution In Community Engages through GKS platform Conducts Household survey Distributes advance information slip During distribution along with AWW and ward member conducts coding Demonstrate how to use LLIN at distribution venue Maintains LLIN register Writes on the village health wall bulletin ( Swasthy Kanth )
Role of ASHA in scaling-up the use of LLIN Organizing meetings for the villagers on LLIN distribution and use Folk arts and different IEC & BCC activities Counseling to increase use Night time monitoring
Role of ASHA in Malaria, Dengue and Diarrhoea (MDD) Campaign MDD is state funded activity to create awareness on outbreak prone monsoon influenced diseases- Malaria Dengue and Diarrhoea. Role of ASHA Coordination with School Delivering awareness messages Engaging in Different IEC activities, e.g. Nidhi Rath Campaign Mobilizing community and increasing participation of children
Role of ASHA in implementation of Indoor Residual Spray (IRS) Advance households regarding date and time of spray Counselling community acceptance Accompanying the spray squad during spray operation Addressing the refusal cases Household counselling on Do s and Don ts regarding IRS intimation to the to increase
Problem of Inaccessibility in Hard-to-reach Areas Inaccessible especially during transmission season in monsoon hindering service delivery when it is most needed. Non-availability of modern transport mechanism throughout the year hindering referral. Community is mostly tribal, marginalized and have poor literacy rate- challenges of poverty, treatment seeking from informal healers, low malaria awareness. It is observed that in theses areas, around 20% of malaria cases in these areas are asymptomatic.
DAMaN Access the Inaccessible Model initiative by the State of Odisha from 2017. FIRST OF ITS KIND IN INDIA. Implementation through camp approach - two rounds annually. Vulnerable centric approach. ASHA, AWW and other community volunteers and PRI members are involved. Package of activities: Mass malaria symptomatic and asymptomatic). Treating of all malaria positive cases. Haemoglobin estimation of Pregnant & lactating mothers Growth assessment of under-5 children. Inaccessi ble villages / hamlets Accessible villages/ hamlets screening (both
Impact of Different Malaria Control Interventions 18 300 In 2002, 433 deaths then avg. 250/ yr till 2010 New inputs : RDT & LLIN 16 250 14 Bivalent RDT & 2nd Phase LLIN 12 200 10 150 8 6 100 4 50 2 0 0 2008 12.23 9.13 239 7.46 0.06 2009 12 9.12 198 7.59 0.05 2010 12.3 9.29 247 7.55 0.06 2011 10.92 7.25 100 6.64 0.03 2012 10.83 6.17 79 5.69 0.03 2013 11.81 5.3 67 4.49 0.03 2014 14.6 9.08 89 6.22 0.02 2015 15.14 9.97 80 6.61 0.02 2016 16.37 10.24 77 6.26 0.02 ABER API Deaths TPR CFR Increased surveillance and complete treatment. Proportionately, Case fatality rate is at lower level.
Program Outcome due to ASHA involvement Deaths reduced by 187% in 2016 compared to 2007 in spite of increase in case detection. Around 40 lakh LLINs could be distributed smoothly through ASHAs- GKS mechanism during 2010-2012 reduction of malaria incidence and deaths by 73.54 % and 268.7% respectively in 2013 compared to 2010. Early diagnosis and complete treatment, mass screening in hard to reach areas and Tribal Residential outbreaks Increase in Passive Surveillance- ABER increase from 12.24% in 2007 to 16.37% in 2016 ASHA contribution to Surveillance Contribution By ASHA Contribution By Others . This resulted 41% 59% Schools averted In 2017, >11.34 million LLINs are being distributed under GFATM support - already 7 million have been distributed through ASHA- GKS mechanism within 2 months and most difficult pockets have been protected before cut off by rains.
Scalability and Opportunity Capacity Building: With enhanced capacity building and increased nos. of ASHAs/ other community volunteers in remote villages/ hamlets, surveillance and EDCT services can be further improved. Inclusive Approach: Health NGOs and other players can support community volunteers in remote inaccessible hamlets and service delivery can be scaled up through inclusive approach. Scale up of best practices: The mass screening and simultaneous vector control under DAMaN can avert deaths and lower malaria transmission rate. Inter-sectoral Coordination: Convergence with other sectors, including sanitation, tribal affairs, rural development, women & child development etc. can add value to DAMaN efforts for alleviation of the problems of malaria and malnutrition
Community Volunteers remains critical in malaria control/elimination THANK YOU FOR KIND ATTENTION End Malaria for Good





 in")


 in Odisha")




")