Understanding Client Motivation for Change in Motivational Interviewing

 undefined
undefined
M
o
t
i
v
a
t
i
o
n
a
l
I
n
t
e
r
v
i
e
w
i
n
g
O
v
e
r
v
i
e
w
Module 12
Blake Beecher, PhD
Eastern Washington University
Learning Objectives:
1.
Spirit of MI, DEARS
2.
OARS practice
3.
Stages of Change informed Intervention
4.
Eliciting, recognizing, and sustaining change talk
You would think . . .
that having had a heart attack would be enough to
persuade a man to quit smoking, change his
diet, exercise more, and take his medication
that hangovers, damaged relationships, an auto
crash, and memory blackouts would be enough
to convince a woman to stop drinking
losing one’s life savings and children’s inheritance
in slot machines would be enough to help a man
to quit gambling
You would think . . . (Cont’d)
that the very real threats of blindness,
amputations and other complications
from diabetes would be enough to
motivate weight loss and glycemic
control
that time spent in the dehumanizing
privations of prison would dissuade
people from re-offending
And yet so often it is not enough for
people to change: What is the Key to
change?
Client Motivation is a Key to Change
Successful treatment outcomes are predicted by:
Pretreatment motivation measures
Treatment attendance
Treatment adherence/compliance
Counselor ratings of motivation and
prognosis
That is, more “motivated” clients do better
Beliefs About Motivation
(True or False?)
1.
Until a person is motivated to change, there is not
much we can do.
2.
It usually takes a significant crisis (“hitting bottom”) to
motivate a person to change.
3.
Motivation is influenced by human connections.
4.
Resistance to change arises from deep-seated
defense mechanisms.
Beliefs About Motivation (Cont’d)
(True or False?)
5.
People choose whether or not they will change.
6.
Readiness for change involves a balancing of “pros”
and “cons.”
7.
Creating motivation for change usually requires
confrontation.
8.
Denial is not a client problem, it is a therapist skill
problem.
Client Motivation is Greatly Influenced
by the Counselor
Clients’ motivation, retention and outcome vary with
the particular counselor to whom they are
assigned
Counselor style strongly drives client resistance
(confrontation drives it up, empathic listening
brings it down)
That is, the
counselor
is one of the biggest
determinants of client motivation and change
Readiness for What?
Rather than asking: “Why isn’t this
person motivated?”
Ask: “What is this person motivated
for?”
Potential Pitfall: Assuming you know.
The Righting Reflex:
NOT Motivational Interviewing
If following the righting instinct, you will
ineffectively ask:
Why don’t you want to change?
Why don’t you try… ?
Okay then, how about…
What makes you think you are not at risk?
How can you tell me you don’t have a problem?
NOT
Motivational Interviewing
Argues that person has a problem and needs to
change – emphasis on acceptance of
problem/diagnosis.
Offers direct advice or prescribes solutions (e.g.,
coping strategies) without actively encouraging
person to make his/her choices.
NOT
Motivational Interviewing
(Cont’d)
Uses authoritative/expert stance and leaves
client in passive role.
Does most of talking or if acts as unidirectional
information system – focus on imparting
information.
NOT
Motivational Interviewing
(Cont’d – 2)
Identifies and modifies maladaptive cognitions.
Allows the client to determine the content and
direction of the counseling.
Behaves in a punitive or coercive manner.
You take one side; I another
When you strong argue one side, the ambivalent
naturally argue the other
The stronger the argument the less likely
change occurs
Common Human Reactions to the Righting Reflex
Angry, agitated
Oppositional
Discounting
Defensive
Justifying
Not understood
Not heard
Procrastinate
Afraid
Helpless, overwhelmed
Ashamed
Trapped
Disengaged
Don’t come back – avoid
Uncomfortable
Resistant
Common Human Reactions to Being Listened to
Understood
Want to talk more
Liking the counselor
Open
Accepted
Respected
Engaged
Able to change
Safe
Empowered
Hopeful
Comfortable
Interested
Want to come back
Cooperative
A Change of Role
You don’t have to
make
change happen
You can’t
You don’t have to come up with all the
answers
You probably don’t have the best ones
You’re not wrestling
You’re dancing
Ambivalence
“
I
w
a
n
t
t
o
c
h
a
n
g
e
,
b
u
t
I
d
o
n
’
t
w
a
n
t
t
o
c
h
a
n
g
e
.
”
Very few decisions in life are made with
100% certainty
Ambivalence is normal
and part of the
change process for everyone
Ambivalence Exercise
1.
Find a partner.
2.
Each of you write down something you are interested in
doing but have mixed feelings about (e.g., studying,
buying a new car, quitting smoking, exercising, etc.).
3.
Select who will speak first.
4.
The speaker presents what it is that s/he would like to
do (but haven’t done yet).
5.
The listener then argues strongly in favor of one of the
options or sides.
6.
Speaker, your job is to listen and note what you are
thinking and feeling.
7.
Switch roles.
Ambivalence Exercise (Cont’d)
What were your thoughts/feelings as the
speaker?
What happens when ambivalence collides
with persuasion, prescription,
convincing?
Motivational Interviewing
M
o
t
i
v
a
t
i
o
n
a
l
i
n
t
e
r
v
i
e
w
i
n
g
i
s
a
s
e
m
i
-
d
i
r
e
c
t
i
v
e
,
c
l
i
e
n
t
-
c
e
n
t
e
r
e
d
c
o
u
n
s
e
l
i
n
g
s
t
y
l
e
t
h
a
t
e
n
h
a
n
c
e
s
m
o
t
i
v
a
t
i
o
n
f
o
r
c
h
a
n
g
e
b
y
h
e
l
p
i
n
g
t
h
e
c
l
i
e
n
t
c
l
a
r
i
f
y
a
n
d
r
e
s
o
l
v
e
a
m
b
i
v
a
l
e
n
c
e
a
b
o
u
t
b
e
h
a
v
i
o
r
c
h
a
n
g
e
.
T
h
e
g
o
a
l
o
f
m
o
t
i
v
a
t
i
o
n
a
l
i
n
t
e
r
v
i
e
w
i
n
g
i
s
t
o
c
r
e
a
t
e
a
n
d
a
m
p
l
i
f
y
d
i
s
c
r
e
p
a
n
c
y
b
e
t
w
e
e
n
p
r
e
s
e
n
t
b
e
h
a
v
i
o
r
a
n
d
b
r
o
a
d
e
r
g
o
a
l
s
.
C
r
e
a
t
e
c
o
g
n
i
t
i
v
e
d
i
s
s
o
n
a
n
c
e
b
e
t
w
e
e
n
W
h
e
r
e
o
n
e
W
h
e
r
e
o
n
e
I
s
n
o
w
w
a
n
t
s
t
o
b
e
MI is Semi-Directive
Two Phases of MI
Phase I:
Building Motivation to Change
Phase II: Strengthening commitment to
change
A
p
p
r
o
p
r
i
a
t
e
M
o
t
i
v
a
t
i
o
n
a
l
S
t
r
a
t
e
g
i
e
s
f
o
r
E
a
c
h
S
t
a
g
e
o
f
C
h
a
n
g
e
P
r
e
p
a
r
a
t
i
o
n
Action
M
a
i
n
t
e
n
a
n
c
e
R
e
c
u
r
r
e
n
c
e
3 Critical Components
of Motivation: Readiness Ruler - WAR
Able
Ready
Willing
W
i
l
l
i
n
g
:
The importance of change:
desires, wants or wills
change
A
b
l
e
:
C
o
n
f
i
d
e
n
c
e
f
o
r
c
h
a
n
g
e
;
f
e
e
l
s
w
i
l
l
i
n
g
b
u
t
u
n
a
b
l
e
-
“
I
w
i
s
h
I
c
o
u
l
d
”
m
a
y
u
s
e
d
e
f
e
n
s
e
m
e
c
h
.
R
e
a
d
y
:
A matter of priorities; “I want
to but not now.”
F
i
v
e
P
r
i
n
c
i
p
l
e
s
o
f
M
I
-
-
D
E
A
R
S
D
e
v
e
l
o
p
D
i
s
c
r
e
p
a
n
c
y
Person rather than the counselor should present the arguments
for change
Change is motivated by a perceived discrepancy between
present behavior and important personal goals or values
E
x
p
r
e
s
s
E
m
p
a
t
h
y
Research indicating importance of empathy
Skillful reflective listening is fundamental
Ambivalence is normal
F
i
v
e
P
r
i
n
c
i
p
l
e
s
o
f
M
I
A
v
o
i
d
A
r
g
u
m
e
n
t
a
t
i
o
n
Confrontation increases client resistance
to change
Labeling is unnecessary
F
i
v
e
P
r
i
n
c
i
p
l
e
s
o
f
M
I
(
C
o
n
t
’
d
)
R
o
l
l
w
i
t
h
R
e
s
i
s
t
a
n
c
e
▫
Provider’s role is to reduce resistance,
since this is correlated with poorer
outcomes
▫
If resistance increases, providers shift to
different strategies
▫
The person’s objections or minimization do
not demand a response
▫
The person is a primary resource in finding
answers and solutions
F
i
v
e
P
r
i
n
c
i
p
l
e
s
o
f
M
I
(
C
o
n
t
’
d
–
2
)
S
u
p
p
o
r
t
S
e
l
f
-
E
f
f
i
c
a
c
y
▫
A person’s belief in the possibility of change
is an important motivator
▫
The person, not the counselor, is
responsible for choosing and carrying out
change
▫
The counselor’s own belief in the person’s
ability to change becomes a self-fulfilling
prophecy
W
h
a
t
I
s
R
e
s
i
s
t
a
n
c
e
?
Verbal and non-verbal behaviors
Expected and normal
Function of interpersonal communication
Continued resistance predictive of reduced
change
Resistance is highly responsive to counselor
style
Getting resistance? Change strategies.
T
y
p
e
s
o
f
R
e
s
i
s
t
a
n
c
e
A
r
g
u
m
e
n
t
Challenging
Discounting
Hostility
I
n
t
e
r
r
u
p
t
i
o
n
Talking over
Cutting off
I
g
n
o
r
i
n
g
Inattention
Non-response
Non-answer
Side-tracking
D
e
n
i
a
l
Blaming
Disagreeing
Excusing
Reluctance
Minimizing
Pessimism
Unwillingness to change
Claiming immunity
WHAT ELSE?????
R
e
s
i
s
t
a
n
c
e
a
n
d
P
e
r
s
u
a
s
i
o
n
Many older approaches to behavior change
relied on the counselor to persuade or
even intimidate client into changing
These approaches often elicit reactance
and reduce the chances that a resistant
client will consider changing a problem
behavior
D
a
n
c
i
n
g
v
s
.
W
r
e
s
t
l
i
n
g
Many MI proponents use the
metaphor of dancing with
clients to illustrate this
method of gently moving
with them around the
ambivalence of change
The Importance of Values “The
Hook”
If Values are not identified, there is no
discrepancy—a main component of MI
What makes their life worth living?
What do they value in their life that is
affected by the problem?
What is most important to them?
What gives their life meaning?
Areas of Values
1.
Family/Parenting
2.
Love/Intimate
relationships
3.
Friends/Social
connectedness
4.
Work/Career
5.
Education/Training
6.
Recreation/Fun
7.
Spirituality
8.
Citizenship/
Community Life
9.
Health/Physical Self
Care
C
a
s
e
#
1
Juan is a 40 year old unemployed plumber who would like
to get back to work, but has difficulty working due to
obesity and uncontrolled diabetes. Juan has tried to alter
his diet and take his medication consistently a few times
in the past, but has slipped back each time has made any
changes. He is in the clinic due to his diabetes and you
received a referral to meet with him.
C
a
s
e
#
2
Gina is a 42 year-old part time college student. She is a
single mother with 4 kids and is working part time. She
has hypertension, anxiety, and depression, and receives
her medication from the clinic for all three. She comes to
the clinic frequently stressed about her health problems
and her life situation.
C
a
s
e
#
3
Rafael is a 29 year old man who is HIV+.
He reports to you that he is having regular unprotected
sex. He tells you that he usually goes to church right
afterwards and prays for forgiveness but “can’t seem to
stop” himself from continuing this behavior. He also
remarks that although he has been feeling “fine” he visits
his primary care doctor frequently.
T
h
e
“
S
p
i
r
i
t
o
f
M
I
”
1
Too much focus on the techniques of MI results in a
loss of its essential style, “sprit” or way of being
•
Motivation elicited from the client, not imposed
from without
•
Client's task, not the counselor's, to articulate +
resolve ambivalence
•
Persuasion is not an effective method for
resolving ambivalence
“
S
p
i
r
i
t
o
f
M
I
”
2
•
Readiness to change not a client trait, but a
fluctuating product of interpersonal interaction
•
The therapeutic relationship is a partnership
rather than expert/recipient roles
“
S
p
i
r
i
t
o
f
M
I
”
3
Central therapist behaviors
•
Understand the person's frame of reference via
reflective listening
•
Express acceptance and affirmation
•
Eliciting + reinforcing the client's self motivational
statements expressions of problem recognition
•
Monitoring the client's degree of readiness to change +
ensuring that resistance is not generated
•
Affirming the client's freedom of choice and self-
direction
M
o
t
i
v
a
t
i
o
n
a
l
I
n
t
e
r
v
i
e
w
i
n
g
Being
Behaving
Techniques
Open-ended
Questions
Reflective
Listening
Affirm
Summarize
Elicit
Change Talk
Core Components
Express
Empathy
Avoid
Argumentation
Roll with
Resistance
Develop
Discrepancy
Support
Self-efficacy
Spirit
Collaboration
Evocation
Autonomy
MI Research Support in Health Settings
4, 5, 6
Substance use decrease
Treatment adherence increase
Treatment engagement increase
HIV risk reduction
Diet and exercise
Gambling decrease
Healthy behavioral change
Motivational interviewing consistently outperforms traditional
advice giving in the treatment of a broad range of behavioral
problems and diseases.
Hettema, J. et al., 2005; Lundahl & Burke 2009; Ruback, S. et al., 2005
References
1.
Miller, W.R. & Rollnick, S. (2002). Motivational interviewing (2nd ed.): Preparing people
for change. New York: Guilford Press.
2.
Miller, W.R. & Rollnick, S. (2002). Motivational interviewing (2nd ed.): Preparing people
for change. New York: Guilford Press.
3.
Miller, W.R. & Rollnick, S. (2002). Motivational interviewing (2nd ed.): Preparing people
for change. New York: Guilford Press.
4.
4. Hettema, J., Steele, J., & Miller, W. (2005). Motivational Interviewing. Annual Review of
Clinical Psychology, 91–111.
5.
5. Lundahl, B. W., & Burke, B. L. (2009). The effectiveness and applicability of
motivational interviewing: A practice-friendly review of four meta-analyses.
Journal of
Clinical Psychology: In session, 65
, 1232-1245.
6.
6. Ruback, S., Sandbaek, A., Lauritzen, T., & Christensen, B. (2005). Motivational
interviewing: A systematic review and meta-analyses. British Journal of General Practice,
April, 305-312.
7.
Center for Substance Abuse Treatment. Enhancing Motivation for Change in Substance
Abuse Treatment. Rockville (MD): Substance Abuse and Mental Health Services
Administration (US); 1999. (Treatment Improvement Protocol (TIP) Series, No. 35.)
Available from: http://www.ncbi.nlm.nih.gov/books/NBK64967/
Motivational Interviewing involves exploring and enhancing client motivation for change. Despite experiencing significant negative consequences, individuals may struggle to make behavioral changes. Motivation is a key factor in successful treatment outcomes, as more motivated clients tend to fare better. Beliefs about motivation are explored, including the notions that change requires personal motivation, crises can drive change, and readiness involves weighing pros and cons. Building motivation in clients does not necessarily entail confrontation, and denial can be a part of the therapeutic process.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Motivational Interviewing Overview Module 12 Blake Beecher, PhD Eastern Washington University
Learning Objectives: 1. Spirit of MI, DEARS 2. OARS practice 3. Stages of Change informed Intervention 4. Eliciting, recognizing, and sustaining change talk
You would think . . . that having had a heart attack would be enough to persuade a man to quit smoking, change his diet, exercise more, and take his medication that hangovers, damaged relationships, an auto crash, and memory blackouts would be enough to convince a woman to stop drinking losing one s life savings and children s inheritance in slot machines would be enough to help a man to quit gambling
You would think . . . (Contd) that the very real threats of blindness, amputations and other complications from diabetes would be enough to motivate weight loss and glycemic control that time spent in the dehumanizing privations of prison would dissuade people from re-offending
And yet so often it is not enough for people to change: What is the Key to change?
Client Motivation is a Key to Change Successful treatment outcomes are predicted by: Pretreatment motivation measures Treatment attendance Treatment adherence/compliance Counselor ratings of motivation and prognosis That is, more motivated clients do better
Beliefs About Motivation (True or False?) 1. Until a person is motivated to change, there is not much we can do. 2. It usually takes a significant crisis ( hitting bottom ) to motivate a person to change. 3. Motivation is influenced by human connections. 4. Resistance to change arises from deep-seated defense mechanisms.
Beliefs About Motivation (Contd) (True or False?) 5. People choose whether or not they will change. 6. Readiness for change involves a balancing of pros and cons. 7. Creating motivation for change usually requires confrontation. 8. Denial is not a client problem, it is a therapist skill problem.
Client Motivation is Greatly Influenced by the Counselor Clients motivation, retention and outcome vary with the particular counselor to whom they are assigned Counselor style strongly drives client resistance (confrontation drives it up, empathic listening brings it down) That is, the counselor is one of the biggest determinants of client motivation and change
Readiness for What? Rather than asking: Why isn t this person motivated? Ask: What is this person motivated for? Potential Pitfall: Assuming you know.
The Righting Reflex: NOT Motivational Interviewing If following the righting instinct, you will ineffectively ask: Why don t you want to change? Why don t you try ? Okay then, how about What makes you think you are not at risk? How can you tell me you don t have a problem?
NOT Motivational Interviewing Argues that person has a problem and needs to change emphasis on acceptance of problem/diagnosis. Offers direct advice or prescribes solutions (e.g., coping strategies) without actively encouraging person to make his/her choices.
NOT Motivational Interviewing (Cont d) Uses authoritative/expert stance and leaves client in passive role. Does most of talking or if acts as unidirectional information system focus on imparting information.
NOT Motivational Interviewing (Cont d 2) Identifies and modifies maladaptive cognitions. Allows the client to determine the content and direction of the counseling. Behaves in a punitive or coercive manner.
You take one side; I another When you strong argue one side, the ambivalent naturally argue the other The stronger the argument the less likely change occurs
Common Human Reactions to the Righting Reflex Angry, agitated Oppositional Discounting Defensive Justifying Not understood Not heard Procrastinate Resistant Afraid Helpless, overwhelmed Ashamed Trapped Disengaged Don t come back avoid Uncomfortable
Common Human Reactions to Being Listened to Safe Empowered Hopeful Comfortable Interested Want to come back Cooperative Understood Want to talk more Liking the counselor Open Accepted Respected Engaged Able to change
A Change of Role You don t have to make change happen You can t You don t have to come up with all the answers You probably don t have the best ones You re not wrestling You re dancing
Ambivalence I want to change, but I don t want to change. Very few decisions in life are made with 100% certainty Ambivalence is normal and part of the change process for everyone
Ambivalence Exercise 1. Find a partner. 2. Each of you write down something you are interested in doing but have mixed feelings about (e.g., studying, buying a new car, quitting smoking, exercising, etc.). 3. Select who will speak first. 4. The speaker presents what it is that s/he would like to do (but haven t done yet). 5. The listener then argues strongly in favor of one of the options or sides. 6. Speaker, your job is to listen and note what you are thinking and feeling. 7. Switch roles.
Ambivalence Exercise (Contd) What were your thoughts/feelings as the speaker? What happens when ambivalence collides with persuasion, prescription, convincing?
Motivational Interviewing Motivational interviewing is a semi-directive, client-centered counseling style that enhances motivation for change by helping the client clarify and resolve ambivalence about behavior change. The goal of motivational interviewing is to create and amplify discrepancy between present behavior and broader goals. Create cognitive dissonance between Where one Is now Where one wants to be
MI is Semi-Directive Nondirective/ Rogerian Motivational Interviewing Allows client to determine content and direction of counseling Systematically directs client toward motivation for change Explores client s conflicts and emotions without specific goals for change Uses empathic reflection noncontingently Seeks to evoke and amplify discrepancy to enhance motivation for change Uses reflection selectively to reinforce motivation for change Avoids interjecting counselor s advice/feedback Offers feedback where appropriate
Two Phases of MI Phase I: Building Motivation to Change Phase II: Strengthening commitment to change
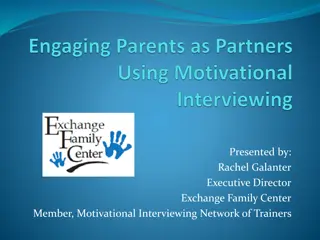
Appropriate Motivational Strategies for Each Stage of Appropriate Motivational Strategies for Each Stage of Change Change Client's Stage of Change Client's Stage of Change Appropriate Motivational Appropriate Motivational Strategies for the Clinician Strategies for the Clinician Precontemplation Precontemplation Establish rapport, ask Establish rapport, ask permission, and build trust. permission, and build trust. Raise doubts or concerns Raise doubts or concerns in the client about in the client about problematic patterns problematic patterns Express concern and Express concern and keep the door open. keep the door open. The client is not yet The client is not yet considering change or is considering change or is unwilling or unable to unwilling or unable to change. change.
Client's Stage of Change Client's Stage of Change Appropriate Motivational Strategies Appropriate Motivational Strategies for the Clinician for the Clinician Normalize ambivalence. Normalize ambivalence. Help the client "tip the Help the client "tip the decisional balance scales" decisional balance scales" toward change. toward change. Elicit and summarize self Elicit and summarize self- - motivational statements of motivational statements of intent and commitment from intent and commitment from the client. the client. Elicit ideas regarding the Elicit ideas regarding the client's perceived self client's perceived self- -efficacy and expectations regarding and expectations regarding treatment. treatment. Contemplation Contemplation The client acknowledges The client acknowledges concerns and is concerns and is considering the possibility considering the possibility of change but is of change but is ambivalent and uncertain. ambivalent and uncertain. efficacy
Preparation Client's Stage of Change Client's Stage of Change Appropriate Motivational Strategies for Appropriate Motivational Strategies for the Clinician the Clinician Explore treatment Explore treatment expectancies and the client's expectancies and the client's role. role. Clarify the client's own Clarify the client's own goals. goals. Negotiate a change Negotiate a change-- --or treatment treatment-- --plan and behavior plan and behavior contract. contract. Consider and lower barriers Consider and lower barriers to change. to change. Help the client enlist social Help the client enlist social support. support. Preparation Preparation The client is committed to and planning to make a change in the near future but is still considering what to do. or
Action Client's Stage of Change Client's Stage of Change Appropriate Motivational Strategies for the Appropriate Motivational Strategies for the Clinician Clinician Engage the client in treatment Engage the client in treatment and reinforce the importance of and reinforce the importance of retaining behavior change. retaining behavior change. Acknowledge difficulties for Acknowledge difficulties for the client in early stages of the client in early stages of change. change. Help the client identify high Help the client identify high- - risk situations through a risk situations through a functional analysis and develop functional analysis and develop appropriate coping strategies to appropriate coping strategies to overcome these. overcome these. Action Action The client is actively taking steps to change but has not yet reached a stable state.
Maintenance Maintenance Client's Stage of Change Client's Stage of Change Appropriate Motivational Strategies for Appropriate Motivational Strategies for the Clinician the Clinician Support lifestyle changes. Support lifestyle changes. Affirm the client's resolve Affirm the client's resolve and self and self- -efficacy. efficacy. Help the client practice and Help the client practice and use new coping strategies to use new coping strategies to avoid a relapse. avoid a relapse. Develop a "fire escape" plan Develop a "fire escape" plan if the client resumes if the client resumes problematic behaviors. problematic behaviors. Review long Review long- -term goals with term goals with the client. the client. Maintenance Maintenance The client has achieved initial goals such as abstinence and is now working to maintain gains.
Recurrence Recurrence Client's Stage of Change Client's Stage of Change Appropriate Motivational Strategies for Appropriate Motivational Strategies for the Clinician the Clinician Help the client reenter the Help the client reenter the change cycle and commend change cycle and commend any willingness to reconsider any willingness to reconsider positive change. positive change. Explore the meaning and Explore the meaning and reality of the recurrence as a reality of the recurrence as a learning opportunity. learning opportunity. Assist the client in finding Assist the client in finding alternative coping strategies. alternative coping strategies. Maintain supportive contact. Maintain supportive contact. Recurrence Recurrence The client has The client has experienced a recurrence experienced a recurrence of symptoms and must of symptoms and must now cope with now cope with consequences and decide consequences and decide what to do next. what to do next.
3 Critical Components of Motivation: Readiness Ruler - WAR Willing: The importance of change: desires, wants or wills change Able: Confidence for change; feels willing but unable- I wish I could may use defense mech. Ready: A matter of priorities; I want to but not now. Able
Five Principles of MI-- DEARS Develop Discrepancy Person rather than the counselor should present the arguments for change Change is motivated by a perceived discrepancy between present behavior and important personal goals or values Express Empathy Research indicating importance of empathy Skillful reflective listening is fundamental Ambivalence is normal
Five Principles of MI Avoid Argumentation Confrontation increases client resistance to change Labeling is unnecessary
Five Principles of MI (Contd) Roll with Resistance Provider s role is to reduce resistance, since this is correlated with poorer outcomes If resistance increases, providers shift to different strategies The person s objections or minimization do not demand a response The person is a primary resource in finding answers and solutions
Five Principles of MI (Contd 2) Support Self-Efficacy A person s belief in the possibility of change is an important motivator The person, not the counselor, is responsible for choosing and carrying out change The counselor s own belief in the person s ability to change becomes a self-fulfilling prophecy
What Is Resistance? Verbal and non-verbal behaviors Expected and normal Function of interpersonal communication Continued resistance predictive of reduced change Resistance is highly responsive to counselor style Getting resistance? Change strategies.
Types of Resistance Argument Challenging Discounting Hostility Interruption Talking over Cutting off Ignoring Inattention Non-response Non-answer Side-tracking Denial Blaming Disagreeing Excusing Reluctance Minimizing Pessimism Unwillingness to change Claiming immunity WHAT ELSE?????
Resistance and Persuasion Many older approaches to behavior change relied on the counselor to persuade or even intimidate client into changing These approaches often elicit reactance and reduce the chances that a resistant client will consider changing a problem behavior
Dancing vs. Wrestling Many MI proponents use the metaphor of dancing with clients to illustrate this method of gently moving with them around the ambivalence of change
The Importance of Values The Hook If Values are not identified, there is no discrepancy a main component of MI What makes their life worth living? What do they value in their life that is affected by the problem? What is most important to them? What gives their life meaning?
Areas of Values 1. Family/Parenting 2. Love/Intimate relationships 3. Friends/Social connectedness 4. Work/Career 5. Education/Training 6. Recreation/Fun 7. Spirituality 8. Citizenship/ Community Life 9. Health/Physical Self Care
Case # 1 Juan is a 40 year old unemployed plumber who would like to get back to work, but has difficulty working due to obesity and uncontrolled diabetes. Juan has tried to alter his diet and take his medication consistently a few times in the past, but has slipped back each time has made any changes. He is in the clinic due to his diabetes and you received a referral to meet with him.
Case # 2 Gina is a 42 year-old part time college student. She is a single mother with 4 kids and is working part time. She has hypertension, anxiety, and depression, and receives her medication from the clinic for all three. She comes to the clinic frequently stressed about her health problems and her life situation.
Case # 3 Rafael is a 29 year old man who is HIV+. He reports to you that he is having regular unprotected sex. He tells you that he usually goes to church right afterwards and prays for forgiveness but can t seem to stop himself from continuing this behavior. He also remarks that although he has been feeling fine he visits his primary care doctor frequently.
The Spirit of MI1 Too much focus on the techniques of MI results in a loss of its essential style, sprit or way of being Motivation elicited from the client, not imposed from without Client's task, not the counselor's, to articulate + resolve ambivalence Persuasion is not an effective method for resolving ambivalence
Spirit of MI2 Readiness to change not a client trait, but a fluctuating product of interpersonal interaction The therapeutic relationship is a partnership rather than expert/recipient roles
Spirit of MI3 Central therapist behaviors Understand the person's frame of reference via reflective listening Express acceptance and affirmation Eliciting + reinforcing the client's self motivational statements expressions of problem recognition Monitoring the client's degree of readiness to change + ensuring that resistance is not generated Affirming the client's freedom of choice and self- direction
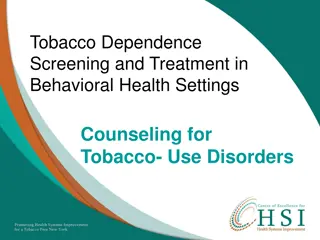
Motivational Interviewing Techniques Open-ended Questions Reflective Listening Elicit Affirm Summarize Change Talk Core Components Express Empathy Roll with Resistance Avoid Develop Discrepancy Support Self-efficacy Argumentation Spirit Collaboration Evocation Autonomy
MI Research Support in Health Settings4, 5, 6 Substance use decrease Treatment adherence increase Treatment engagement increase HIV risk reduction Diet and exercise Gambling decrease Healthy behavioral change Motivational interviewing consistently outperforms traditional advice giving in the treatment of a broad range of behavioral problems and diseases. Hettema, J. et al., 2005; Lundahl & Burke 2009; Ruback, S. et al., 2005
References 1. Miller, W.R. & Rollnick, S. (2002). Motivational interviewing (2nd ed.): Preparing people for change. New York: Guilford Press. 2. Miller, W.R. & Rollnick, S. (2002). Motivational interviewing (2nd ed.): Preparing people for change. New York: Guilford Press. 3. Miller, W.R. & Rollnick, S. (2002). Motivational interviewing (2nd ed.): Preparing people for change. New York: Guilford Press. 4. 4. Hettema, J., Steele, J., & Miller, W. (2005). Motivational Interviewing. Annual Review of Clinical Psychology, 91 111. 5. 5. Lundahl, B. W., & Burke, B. L. (2009). The effectiveness and applicability of motivational interviewing: A practice-friendly review of four meta-analyses. Journal of Clinical Psychology: In session, 65, 1232-1245. 6. 6. Ruback, S., Sandbaek, A., Lauritzen, T., & Christensen, B. (2005). Motivational interviewing: A systematic review and meta-analyses. British Journal of General Practice, April, 305-312. 7. Center for Substance Abuse Treatment. Enhancing Motivation for Change in Substance Abuse Treatment. Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 1999. (Treatment Improvement Protocol (TIP) Series, No. 35.) Available from: http://www.ncbi.nlm.nih.gov/books/NBK64967/



")



")












")












")
")