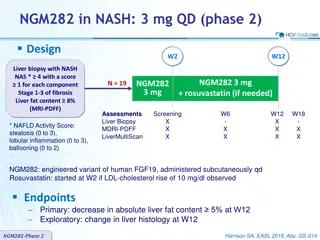
Safety and Feasibility of TIPS in Elderly Patients with Liver Cirrhosis
J
o
u
r
n
a
l
c
l
u
b
H
e
p
a
t
o
l
o
g
y
3
0
.
0
7
.
2
0
2
0
“
S
a
f
e
t
y
a
n
d
f
e
a
s
i
b
i
l
i
t
y
o
f
t
r
a
n
s
j
u
g
u
l
a
r
i
n
t
r
a
h
e
p
a
t
i
c
p
o
r
t
o
s
y
s
t
e
m
i
c
s
h
u
n
t
i
n
e
l
d
e
r
l
y
p
a
t
i
e
n
t
s
w
i
t
h
l
i
v
e
r
c
i
r
r
h
o
s
i
s
a
n
d
r
e
f
r
a
c
t
o
r
y
a
s
c
i
t
e
s
”
Stockhoff et al. Publishes 06/2020 in Plos one
Luisa Mathieu-Levin
B
a
c
k
g
r
o
u
n
d
I
•
Challenging management of liver cirrhosis with refractory ascites, specially at
higher age
•
Mortality can reach up to 50% in one year
•
Only curative treatment option is transplantation. Not always realistically available
•
TIPS is an established (non curative) treatment option
•
What is TIPS: artificial channel within the liver that establishes communication
between the inflow portal vein and the outflow hepatic vein.
•
Endovascular procedure, insertion via jugular vein. First successful TIPS 1988.
Steps in a TIPS procedure:
A)
initial situation with portal hypertension
B) a needle has been introduced (via the
jugular vein) and is passing from the hepatic
vein into the portal vein
C) the tract is dilated with a balloon
D) after placement of a stent, portal pressure
is normalized
Goal of TIPS: reduce immediately the portal
hypertension and the complications from
portal hypertension.
R. Torrance Andrews, 2011
B
a
c
k
g
r
o
u
n
d
I
I
•
Indications for TIPS:
•
Refractory ascites, variceal bleeding (2
nd
prevention/2
nd
line for acute bleeding), portal vein thrombosis ,
Budd-Chiari , (hepatic-veno-occlusive disease, hepatic hydrothorax, portal hypertensive gastropathy,
hepatopulmonary syndrome, HRS)
•
Absolute Contraindications:
•
Severe congestive heart failure, tricuspid regurgitation, severe pulmonary hypertension, sepsis, multiple
hepatic cysts, unrelieved biliary obstruction
•
Relative CI:
•
HE, significant PVT, > INR 5, Tc < 20, moderate pulmonary hypertension, HCC,
obstruction of all hepatic
veins
•
Possible periinterventional complications:
•
Operative mortality <1%, Acute bleeding and direct liver injury (rare), transient HE, hepatic ischemia (acute
liver failure secondary to hepatic ischemia), acute kidney failure, heart failure, Infection (Endotipsitis),
Closure (Clotting)
B
a
c
k
g
r
o
u
n
d
I
I
I
•
Risks of TIPS long term:
•
hepatic encephalopathy, aggravation of hyperdynamic circulatory state (up to short term cardiac failure)
•
Careful selection of patients is crucial
•
EASL Guidelines: Age is not mentioned as a parameter. In many centers, higher age is
considered a contraindication, specially because of increased risk of hepatic
encephalopathy in patients of higher age
.
Not in Bern.
•
Only few safety and feasibility data for elderly patients. In most studies either older
patients were excluded / small retrospective studies with controversial outcome / no
paracentesis control group.
T
o
s
u
m
u
p
:
The management of patients with liver cirrhosis and refractory ascites is challenging,
particularly at higher age. TIPS is an established treatment for refractory ascites, but safety
data in elderly patients are rare.
Q
u
e
s
t
i
o
n
a
n
d
a
i
m
o
f
t
h
e
s
t
u
d
y
E
v
a
l
u
a
t
e
s
a
f
e
t
y
a
n
d
f
e
a
s
i
b
i
l
i
t
y
o
f
T
I
P
S
i
n
e
l
d
e
r
l
y
p
a
t
i
e
n
t
s
w
i
t
h
c
i
r
r
h
o
s
i
s
a
n
d
r
e
f
r
a
c
t
o
r
y
a
s
c
i
t
e
s
.
S
t
u
d
y
d
e
s
i
g
n
a
n
d
m
e
t
h
o
d
s
•
Single centre Study at Hannover Medical School in Germany
•
Retrospective Analysis 2012-2018
•
Comparison between groups :
•
Young vs older TIPS patients
•
Older TIPS patients vs older paracentesis patients
•
non-randomized
Inclusion criteria: TIPS at
Hannover Medical school 2012-
2018, liver cirrhosis and
refractory ascites
T
I
P
S
G
r
o
u
p
> 2.2 million patients with German
operation and procedure code for
TIPS surgical procedure.
P
a
r
a
c
e
n
t
e
s
i
s
g
r
o
u
p
:
•
Hannover Ascites cohort (> 600 patients with decompensated liver cirrhosis and ascites)
•
Inclusion criteria: >= 65 years old, refractory ascites
•
Exclusion: TIPS contraindications like pulmonary hypertension, Hepatic encephalopathy
(>= 2/chronic) , HCC, cardiac failure and also acute clinical deterioration, Budd Chiari,
ongoing infection
•
Goal: minimize bias between the two groups
•
n=85
•
P
r
i
m
a
r
y
e
n
d
p
o
i
n
t
s
:
m
o
r
t
a
l
i
t
y
/
s
u
r
i
v
a
l
2
8
d
a
y
s
,
9
0
d
a
y
s
a
n
d
1
y
e
a
r
a
f
t
e
r
T
I
P
S
i
n
s
e
r
t
i
o
n
•
S
e
c
o
n
d
a
r
y
e
n
d
p
o
i
n
t
s
:
•
periinterventional complications (Infections, HE, AKI , ACLF,) duration of hospital stay
•
ascites control, changes of creatinine levels after TIPS insertion
•
A
djustment for degree of portal hypertension (PSG), severity of liver disease (MELD), sex,
etiology of cirrhosis
•
1:1 Propensity score matching between elderly TIPS patients and elderly paracentesis patients
(Matching covariates: MELD, sex, age, bilirubin, Tc, Sodium)
•
Drop outs: liver transplantation, end of follow up
•
Baseline time of tips insertion or time of first paracentesis
B
a
s
e
l
i
n
e
c
h
a
r
a
c
t
e
r
i
s
t
i
c
s
o
f
T
I
P
S
p
a
t
i
e
n
t
s
•
61% alcohol related liver cirrhosis. In the younger patients the
amount of alcohol-related liver disease was higher (p= 0.035)
•
Median MELD of 12.6. MELD, Bili and Tc about the same
between younger and elderly. Elderly higher creatinine levels,
lower INR at baseline
•
No difference in CHILD
between age groups
•
Hemodynamic success ( finals PSG <= 12 mmHg) achieved in
99.4%. Median preinterventional PSG 16.2mmHg. Median
postinterventional PSG 5.9 mmHg
•
Final PSG significantly lower in patients >= 65 y (p=0.037)
P
r
i
m
a
r
y
e
n
d
p
o
i
n
t
s
:
m
o
r
t
a
l
i
t
y
2
8
d
a
y
s
,
9
0
d
a
y
s
a
n
d
1
y
e
a
r
a
f
t
e
r
T
I
P
S
i
n
s
e
r
t
i
o
n
.
•
Mortality after 28d of TIPS placement was similar between < 65
and >= 65 y (p= 0.35)
•
In contrast, survival of younger patients was significantly higher
at 90d (p= 0.029)
•
the 1 year survival was again very similar
•
no difference between medium old 65-74 and very old > 75
•
Overall 19% died in 1 year (18% < 65y, 23% >= 65y)
•
Proportion of death related to impaired liver function higher in younger cohort (Supplements;
liver, cardiac, infection, other/unknown)
Adjustments (Table 3b)
•
A
ge > = 65 y remained a predictor for 90d mortality
.
Age
>= 65 y no
t
a predictor
for 28d or 1
year mortality.
•
MELD score associated with survival at all three times (p= 0.001)
•
Sex, degree of portal hypertension and cirrhosis etiology insignificant predictors
•
Other article: „ Is 70 the new 50?
Complication and outcomes of transjugular intrahepatic
portosystemic shunt in older versus younger patients“ (Bisht et al. 2020) -> Age does not
matter (All TIPS indications
, complication rather than survival)
R
e
s
u
l
t
s
:
s
e
c
o
n
d
a
r
y
e
n
d
p
o
i
n
t
s
•
In older patients hospital stay was significantly longer (8 vs 6 days, p=0.03).
•
Elderly patients has significantly more ACLF episodes 21% vs 9% (p= 0.044).
•
No difference for HE, AKI or Infection
•
Sufficient ascites control after 2 to 6 month after TIPS insertion was achieved in 68%. Ascites
persisted in a significantly higher proportion of younger patients (37% vs 12% in elderly, p=
0.048)
C
o
m
p
a
r
i
s
o
n
T
I
P
S
v
s
p
a
r
a
c
e
n
t
e
s
i
s
•
53 matched pairs (all >= 65 y)
•
no large imbalances between
groups, no significant differences in
the covariates (e.g. similar MELD
Score)
•
No significant difference in 28 d
mortality (p= 0.196), 90d mortality
(p=0.808) or 1 year survival
(p=0.419 ) between elderly TIPS
and matched paracentesis group.
M
a
i
n
r
e
s
u
l
t
s
•
Periinterventional course in those >= 65 years appears to be slightly more complicated than in < 65
years as reflected by a significant longer hospital stay ( p=0.03) and more ACLF -episodes (21% vs.
9%; p= 0.44).
•
28-day mortality was similar between both groups (p= 0.350), whereas survival of the younger
patients was significantly higher at 90 days (p= 0.029).
•
In the multivariate analysis age >= 65 years remained an independent predictor for 90-days
mortality (p= 0.028), while it was not a associated with 28-day mortality and 1-year survival.
•
After matching for potential confounders 1-year survival was similar in elderly patients if treated with
TIPS or paracentesis ( p= 0.419)
L
i
m
i
t
a
t
i
o
n
s
•
Retrospective, non randomized
•
inherent selection bias regarding TIPS vs Paracentesis allocation
•
small sample size
•
single institution
•
Dysfunction of TIPS for survival
?
•
Nutritional status of patients?
C
o
n
c
l
u
s
i
o
n
s
TIPS placement in elderly patients with refractory ascites appears to be
slightly more complicated compared to younger individuals, but overall
feasible and at least not inferior to paracentesis.
Challenging liver cirrhosis management in elderly patients with refractory ascites has high mortality rates, and transplantation is not always viable. Transjugular intrahepatic portosystemic shunt (TIPS) serves as a non-curative treatment option, aiming to reduce portal hypertension. The procedure involves creating a channel between the portal vein and hepatic vein, effectively lowering portal pressure. TIPS is indicated for multiple conditions but has both absolute and relative contraindications. Despite potential complications, careful patient selection is key due to risks such as hepatic encephalopathy and circulatory issues. Considerations like age, not universally agreed upon, impact the decision to perform TIPS.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Journal club Hepatology 30.07.2020 Safety and feasibility of transjugular intrahepatic portosystemic shunt in elderly patients with liver cirrhosis and refractory ascites Stockhoff et al. Publishes 06/2020 in Plos one Luisa Mathieu-Levin
Background I Challenging management of liver cirrhosis with refractory ascites, specially at higher age Mortality can reach up to 50% in one year Only curative treatment option is transplantation. Not always realistically available TIPS is an established (non curative) treatment option What is TIPS: artificial channel within the liver that establishes communication between the inflow portal vein and the outflow hepatic vein. Endovascular procedure, insertion via jugular vein. First successful TIPS 1988.
Steps in a TIPS procedure: A) initial situation with portal hypertension B) a needle has been introduced (via the jugular vein) and is passing from the hepatic vein into the portal vein C) the tract is dilated with a balloon D) after placement of a stent, portal pressure is normalized Goal of TIPS: reduce immediately the portal hypertension and the complications from portal hypertension. R. Torrance Andrews, 2011
Background II Indications for TIPS: Refractory ascites, variceal bleeding (2ndprevention/2ndline for acute bleeding), portal vein thrombosis , Budd-Chiari , (hepatic-veno-occlusive disease, hepatic hydrothorax, portal hypertensive gastropathy, hepatopulmonary syndrome, HRS) Absolute Contraindications: Severe congestive heart failure, tricuspid regurgitation, severe pulmonary hypertension, sepsis, multiple hepatic cysts, unrelieved biliary obstruction Relative CI: HE, significant PVT, > INR 5, Tc < 20, moderate pulmonary hypertension, HCC, obstruction of all hepatic veins Possible periinterventional complications: Operative mortality <1%, Acute bleeding and direct liver injury (rare), transient HE, hepatic ischemia (acute liver failure secondary to hepatic ischemia), acute kidney failure, heart failure, Infection (Endotipsitis), Closure (Clotting)
Background III Risks of TIPS long term: hepatic encephalopathy, aggravation of hyperdynamic circulatory state (up to short term cardiac failure) Careful selection of patients is crucial EASL Guidelines: Age is not mentioned as a parameter. In many centers, higher age is considered a contraindication, specially because of increased risk of hepatic encephalopathy in patients of higher age. Not in Bern. Only few safety and feasibility data for elderly patients. In most studies either older patients were excluded / small retrospective studies with controversial outcome / no paracentesis control group. To sum up: The management of patients with liver cirrhosis and refractory ascites is challenging, particularly at higher age. TIPS is an established treatment for refractory ascites, but safety data in elderly patients are rare.
Question and aim of the study Evaluate safety and feasibility of TIPS in elderly patients with cirrhosis and refractory ascites. Studydesign and methods Single centre Study at Hannover Medical School in Germany Retrospective Analysis 2012-2018 Comparison between groups : Young vs older TIPS patients Older TIPS patients vs older paracentesis patients non-randomized
> 2.2 million patients with German operation and procedure code for TIPS surgical procedure. TIPS Group Inclusion criteria: TIPS at Hannover Medical school 2012- 2018, liver cirrhosis and refractory ascites
Paracentesis group: Hannover Ascites cohort (> 600 patients with decompensated liver cirrhosis and ascites) Inclusion criteria: >= 65 years old, refractory ascites Exclusion: TIPS contraindications like pulmonary hypertension, Hepatic encephalopathy (>= 2/chronic) , HCC, cardiac failure and also acute clinical deterioration, Budd Chiari, ongoing infection Goal: minimize bias between the two groups n=85
Primary endpoints: mortality/surival 28 days, 90 days and 1 year after TIPS insertion Secondary endpoints: periinterventional complications (Infections, HE, AKI , ACLF,) duration of hospital stay ascites control, changes of creatinine levels after TIPS insertion Adjustment for degree of portal hypertension (PSG), severity of liver disease (MELD), sex, etiology of cirrhosis 1:1 Propensity score matching between elderly TIPS patients and elderly paracentesis patients (Matching covariates: MELD, sex, age, bilirubin, Tc, Sodium) Drop outs: liver transplantation, end of follow up Baseline time of tips insertion or time of first paracentesis
Baseline characteristics of TIPS patients 61% alcohol related liver cirrhosis. In the younger patients the amount of alcohol-related liver disease was higher (p= 0.035) Median MELD of 12.6. MELD, Bili and Tc about the same between younger and elderly. Elderly higher creatinine levels, lower INR at baseline No difference in CHILD between age groups Hemodynamic success ( finals PSG <= 12 mmHg) achieved in 99.4%. Median preinterventional PSG 16.2mmHg. Median postinterventional PSG 5.9 mmHg Final PSG significantly lower in patients >= 65 y (p=0.037)
Primary endpoints: mortality 28 days, 90 days and 1 year after TIPS insertion. Mortality after 28d of TIPS placement was similar between < 65 and >= 65 y (p= 0.35) In contrast, survival of younger patients was significantly higher at 90d (p= 0.029) the 1 year survival was again very similar no difference between medium old 65-74 and very old > 75
Overall 19% died in 1 year (18% < 65y, 23% >= 65y) Proportion of death related to impaired liver function higher in younger cohort (Supplements; liver, cardiac, infection, other/unknown) Adjustments (Table 3b) Age > = 65 y remained a predictor for 90d mortality. Age >= 65 y not a predictor for 28d or 1 year mortality. MELD score associated with survival at all three times (p= 0.001) Sex, degree of portal hypertension and cirrhosis etiology insignificant predictors Other article: Is 70 the new 50? Complication and outcomes of transjugular intrahepatic portosystemic shunt in older versus younger patients (Bisht et al. 2020) -> Age does not matter (All TIPS indications, complication rather than survival)
Results: secondary endpoints In older patients hospital stay was significantly longer (8 vs 6 days, p=0.03). Elderly patients has significantly more ACLF episodes 21% vs 9% (p= 0.044). No difference for HE, AKI or Infection Sufficient ascites control after 2 to 6 month after TIPS insertion was achieved in 68%. Ascites persisted in a significantly higher proportion of younger patients (37% vs 12% in elderly, p= 0.048)
Comparison TIPS vs paracentesis 53 matched pairs (all >= 65 y) no large imbalances between groups, no significant differences in the covariates (e.g. similar MELD Score) No significant difference in 28 d mortality (p= 0.196), 90d mortality (p=0.808) or 1 year survival (p=0.419 ) between elderly TIPS and matched paracentesis group.
Main results Periinterventional course in those >= 65 years appears to be slightly more complicated than in < 65 years as reflected by a significant longer hospital stay ( p=0.03) and more ACLF -episodes (21% vs. 9%; p= 0.44). 28-day mortality was similar between both groups (p= 0.350), whereas survival of the younger patients was significantly higher at 90 days (p= 0.029). In the multivariate analysis age >= 65 years remained an independent predictor for 90-days mortality (p= 0.028), while it was not a associated with 28-day mortality and 1-year survival. After matching for potential confounders 1-year survival was similar in elderly patients if treated with TIPS or paracentesis ( p= 0.419)
Limitations Retrospective, non randomized inherent selection bias regarding TIPS vs Paracentesis allocation small sample size single institution Dysfunction of TIPS for survival? Nutritional status of patients?
Conclusions TIPS placement in elderly patients with refractory ascites appears to be slightly more complicated compared to younger individuals, but overall feasible and at least not inferior to paracentesis.











")