Transition Planning for Community Treatment Programs

Oregon Center of Excellence for
Assertive Community Treatment
Why focus on transition planning?
Topic has been identified during reviews and technical
assistance as an area where Oregon programs could
benefit from additional support
Determining which criteria to use
Fully implementing policy
Mitigating external pressure to transition participants
early
August 2015 Transition
Presentation Conclusions
Research shows that individuals who receive ACT
services can successfully transfer to less intensive
services
It is important to identify individuals are ready to
make the transition by meeting recovery
benchmarks/criteria
Teams can expect that only a small percentage of ACT
individuals that have been served over a long period of
time will be ready to transition from ACT (research
indicated 9-14% met transition readiness criteria) even
after being served by ACT 4+ years
Topics to Cover
Fidelity scale criteria
Selecting criteria to determine readiness for transition
Determining additional individual criteria, if any, for
each ACT participant
Determining when and how this will be reviewed
Identifying individuals who may be ready for
transition
Planning for transition
Maintaining contact post transition
Determining need for returning to services
OCEACT Fidelity Scale Criteria
The team conducts a regular assessment of the need
for ACT services for each participant.
The team uses explicit criteria or markers for need to
transfer to less intensive service options.
Transition is gradual and individualized, with assured
continuity of care.
Status is monitored following transition, per
individual need.
There is an option to return to the ACT team as
needed.
Selecting Transition Criteria
Readily Available Criteria:
OCEACT Transition to Less Intensive Services Policy
Transition Readiness Scale, Donahue et al., 2012
(New York)
ACT Transition Readiness Scale (ATR), Cuddeback, 2011
(North Carolina)
OCEACT Transition to Less Intensive
Services Policy
Covers:
Timeline for reviewing criteria (quarterly)
Criteria checklist for transition to less intensive services
Criteria for re-admission to ACT services
OCEACT’s Criteria Checklist
Used ATR, TRS, and documentation from ACT
programs around Oregon to compile a more complete
list of indicators of ongoing service need
Added focus on community integration domains
Building strong community supports outside of mental
health service delivery system is key to successful
transition (Herman, 2011)
Looking for improved quality of life
Quality of Life
Changes in individual needs for care and quality of life in
Assertive Community Treatment patients: an observational
study (
Kortrijk et al., BMC Psychiatry, 2014)
Decrease in number of unmet needs predictive of higher
Quality of Life score at follow up
The five unmet needs reported most:
Daytime activities (T0 74%; T1 57%)
Company (T0 72%; T1 62%)
Intimate relationships (T0 52%; T1 45%)
Psychological distress (T0 39%; T1 31%)
Psychotic symptoms (T0 34%; T1 27%)
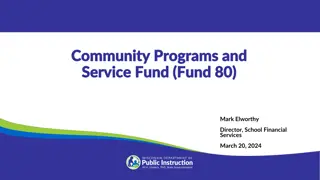
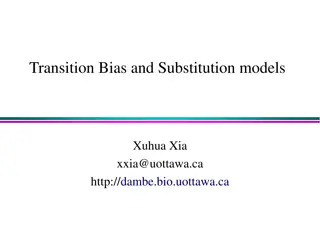
Figure 1 Outcome on quality of life, a combination of SEM and CS cut-off. Legend: The horizontal axis represents the baseline Quality of Life (QoL) total
score and the vertical axis represents the follow up QoL total score. Each data point represents the combination of the baseline and follow-up QoL total
score and illustrates if QoL improves, stabilizes, or worsens over time. The horizontal line represents the clinical significance cut-off between low level of
QoL and high level of QoL at follow-up. The diagonal lines represent meaningful change in QoL total score.
Kortrijk et al.
BMC Psychiatry 2014
http://www.biomedcentral.com/1471-244X/14/306
C
h
a
n
g
e
i
n
S
c
o
r
e
s
f
o
r
A
C
T
P
a
r
t
i
c
i
p
a
n
t
s
:
39.4%
improvement in
quality of life
45.8%
remained stable
14.7%
deteriorated
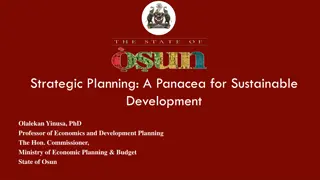
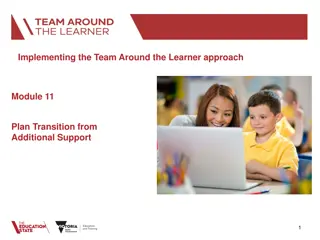
Matching Interventions to Outcomes
Checklist
Multiple criteria in each domain:
Treatment Engagement
Housing
Psychiatric Medication Use
Psychiatric Hospitalization and Emergency Room Use
High-risk Behaviors
Substance Abuse
Forensic Involvement
Education and Vocational Activity
Self-Care
Social Relationships
Health & Medical Status
Financial & Income Stability
Other Criteria Specific to Individual
Determining Individual Criteria
What additional needs does this individual have that
may impact their ability to successfully transition from
ACT services?
Examples:
Ability to cope effectively with significant date (e.g.
holiday, anniversary of loss, etc.)
Has successfully reconnected with important life role
(e.g. artist, athlete, etc.)
Document and review quarterly – informs service
planning process
Reviewing Criteria
Establish a timeline (OCEACT recommends quarterly)
Determine how criteria will be reviewed
Group supervision
Individual treatment teams
Daily team meetings
Service planning reviews
Review
all
ACT participants
Document review
See change over time
Monitor effectiveness of interventions over the past quarter
Plan for current service need
Service Planning
Reviewing progress toward transition informs service
planning
Identifies unmet needs
Assessment over time may help to assess effectiveness of
interventions
Provides more clear direction for service planning
Example
Jane has been receiving ACT services for 5 years. She now has stable
housing, part time employment, and improved physical health.
During a quarterly assessment of readiness for transition, it is
determined that Jane has not yet met the criteria under the “substance
use”, “social relationships”, and “financial & income stability” domains.
She is meeting all other transition criteria.
When explored with Jane, the team learns:
Jane is avoiding past friends that she used with because she wants to
become sober – she has not yet made any sober friends.
Jane experiences periodic substance use relapses which impact her
finances – she doesn’t have money for social activities. (1-2 times per
month meth use which she reports helps her focus at work.)
Jane’s most recent E-IMR goal is “to make a new friend.”
If the transition checklist looks for a 12 month period of stability in all
domains, what would be the next steps for Jane in her work with the
ACT team?
Identifying Individuals Ready for
Transition
Transition planning can begin with the individual is has
met or is close to meeting:
Criteria on checklist
Individually important criteria
Personally important goals
Individual and the ACT team mutually agree to plan for
transition out of ACT services
Note: circumstances may change during transition
planning process, which could indicate need for continued
ACT services
Avoid graduating individuals from ACT prematurely
(revolving door)
Planning for Transition
Gradual transition from ACT services with assured
continuity of care
Ideally occurs over 3-6 months
Documented transition plan which participant and team have
agreed to, which includes:
Any remaining goals to be met prior to transition
Plan for reducing ACT services
As community integration increases it is not uncommon for
services to naturally decrease over a period of time
Which services may still need to reduced
Over what period of time services will be reduced
Where individual will access services post transition
Overlapping service period (ACT and new provider)
Plan for ACT team to monitor transition (60 days)
Maintaining Contact
OCEACT recommends maintaining contact with the
ACT participant to ensure a successful transition for at
least 60 days post transition
Plan for contact
Contact person(s)
Frequency of contact
Type of contact
Documentation
Not just for reviews:
Future treatment providers (continuity of care)
Participant / family
Legal
Assessing Need for ACT Services
Post Transition
Individual may return to ACT services if the individual
was discharged from ACT within the past twelve (12)
months and any of the following has occurred, or the
individual is at risk of the following:
A psychiatric hospitalization, admission to an acute / sub-
acute psychiatric facility, or use of psychiatric emergency
services
A hospitalization or an emergency room visit as a result of
substance abuse
An arrest or other law enforcement contact
Homelessness or housing instability
Keep program capacity in mind
Documentation
Individual criteria being assessed for each participant
Participant has an active role in defining how they want their life to look
Assessments for transition readiness conducted over time
Clearly documented transition plan
Participant actively defines what transition will look like
Specific timeframes
Plan includes:
Any remaining goals to be met prior to transition
Plan for reducing ACT services
Where individual will access services post transition
Overlapping service period (ACT and new provider)
Plan for ACT team to monitor transition (60 days)
Progress notes
Document participant’s role in transition planning
Show that transition is planned and gradual based on reduced service need
Needs and progress documented in notes is consistent with transition
assessments
Questions?
References
Cuddeback, G.S. (2011). The Assertive Community Treatment Transition
Readiness Scale User Manual.
http://www.eastpointe.net/providers/providerforms/networkoperations/A
TR%20User's%20Manual%202011.pdf
Donahue, SA; Manuel JI, Herman DB, Fraser LH, Chen H, Essock SM.
(2012). Development and use of a transition readiness scale to help manage
ACT team capacity.
Psychiatric Services
: 63(3) 223-9.
http://ps.psychiatryonline.org/doi/full/10.1176/appi.ps.201100041
Herman DS, Conover S, Gorroochurn P, et al. (2011). Randomized trial of
critical time intervention to prevent homelessness after hospital discharge.
Psychiatric Services
62: 713–719
Kortrijk1, Hans, Kamperman, Astrid, Mulder, Cornelis. (2014). Changes in
individual needs for care and quality of life in Assertive Community
Treatment patients: an observational study.
BMC Psychiatry
: 14:306
http://bmcpsychiatry.biomedcentral.com/articles/10.1186/s12888-014-
0306-8
Oregon Center of Excellence for Assertive Community Treatment focuses on transition planning to help individuals move from intensive services to less intensive ones. Research shows that only a small percentage of individuals are ready to transition after being served by ACT for years. Topics covered include fidelity scale criteria, selecting transition criteria, and maintaining contact post transition to ensure continuity of care.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Oregon Center of Excellence for Assertive Community Treatment
Why focus on transition planning? Topic has been identified during reviews and technical assistance as an area where Oregon programs could benefit from additional support Determining which criteria to use Fully implementing policy Mitigating external pressure to transition participants early
August 2015 Transition Presentation Conclusions Research shows that individuals who receive ACT services can successfully transfer to less intensive services It is important to identify individuals are ready to make the transition by meeting recovery benchmarks/criteria Teams can expect that only a small percentage of ACT individuals that have been served over a long period of time will be ready to transition from ACT (research indicated 9-14% met transition readiness criteria) even after being served by ACT 4+ years
Topics to Cover Fidelity scale criteria Selecting criteria to determine readiness for transition Determining additional individual criteria, if any, for each ACT participant Determining when and how this will be reviewed Identifying individuals who may be ready for transition Planning for transition Maintaining contact post transition Determining need for returning to services
OCEACT Fidelity Scale Criteria The team conducts a regular assessment of the need for ACT services for each participant. The team uses explicit criteria or markers for need to transfer to less intensive service options. Transition is gradual and individualized, with assured continuity of care. Status is monitored following transition, per individual need. There is an option to return to the ACT team as needed.
Selecting Transition Criteria Readily Available Criteria: OCEACT Transition to Less Intensive Services Policy Transition Readiness Scale, Donahue et al., 2012 (New York) ACT Transition Readiness Scale (ATR), Cuddeback, 2011 (North Carolina)
OCEACT Transition to Less Intensive Services Policy Covers: Timeline for reviewing criteria (quarterly) Criteria checklist for transition to less intensive services Criteria for re-admission to ACT services
OCEACTs Criteria Checklist Used ATR, TRS, and documentation from ACT programs around Oregon to compile a more complete list of indicators of ongoing service need Added focus on community integration domains Building strong community supports outside of mental health service delivery system is key to successful transition (Herman, 2011) Looking for improved quality of life
Quality of Life Changes in individual needs for care and quality of life in Assertive Community Treatment patients: an observational study (Kortrijk et al., BMC Psychiatry, 2014) Decrease in number of unmet needs predictive of higher Quality of Life score at follow up The five unmet needs reported most: Daytimeactivities (T0 74%; T1 57%) Company (T0 72%; T1 62%) Intimaterelationships (T0 52%; T1 45%) Psychological distress (T0 39%; T1 31%) Psychoticsymptoms (T0 34%; T1 27%)
Change in Scores for ACT Participants: 39.4% improvement in quality of life 45.8% remained stable 14.7% deteriorated Figure 1 Outcome on quality of life, a combination of SEM and CS cut-off. Legend: The horizontal axis represents the baseline Quality of Life (QoL) total score and the vertical axis represents the follow up QoL total score. Each data point represents the combination of the baseline and follow-up QoL total score and illustrates if QoL improves, stabilizes, or worsens over time. The horizontal line represents the clinical significance cut-off between low level of QoL and high level of QoL at follow-up. The diagonal lines represent meaningful change in QoL total score. Kortrijk et al. BMC Psychiatry 2014 http://www.biomedcentral.com/1471-244X/14/306
Matching Interventions to Outcomes Service category Description of the content in the process Alleviating symptoms and distress (medications, therapy, IDDT, evidenced based practices) Controlling and resolving critical or dangerous problems Obtaining the services and coordinating care wanted and needed Consumer outcomes Mental health treatment/co- occurring TX Crisis Intervention Symptom Relief/Improved mental well-being Personal safety assured Case management Service access REHABILITATION Developing skills and supports related to individual s goals Engaging individuals in fulfilling and satisfying activities Advocating to uphold one s rights Providing the people places and things needed to survive (shelter, food, medical care) Exercising a voice and choice in one s life Promoting healthy lifestyles ROLE FUNCTIONING ENRICHMENT SELF- DEVELOPMENT/EFFICACY Equal opportunity Personal survival assured Rights protection Basic support Self-help Empowerment Wellness/Prevention Health status improved
Checklist Multiple criteria in each domain: Treatment Engagement Housing Psychiatric Medication Use Psychiatric Hospitalization and Emergency Room Use High-risk Behaviors Substance Abuse Forensic Involvement Education and Vocational Activity Self-Care Social Relationships Health & Medical Status Financial & Income Stability Other Criteria Specific to Individual
Determining Individual Criteria What additional needs does this individual have that may impact their ability to successfully transition from ACT services? Examples: Ability to cope effectively with significant date (e.g. holiday, anniversary of loss, etc.) Has successfully reconnected with important life role (e.g. artist, athlete, etc.) Document and review quarterly informs service planning process
Reviewing Criteria Establish a timeline (OCEACT recommends quarterly) Determine how criteria will be reviewed Group supervision Individual treatment teams Daily team meetings Service planning reviews Review all ACT participants Document review See change over time Monitor effectiveness of interventions over the past quarter Plan for current service need
Service Planning Reviewing progress toward transition informs service planning Identifies unmet needs Assessment over time may help to assess effectiveness of interventions Provides more clear direction for service planning
Example Jane has been receiving ACT services for 5 years. She now has stable housing, part time employment, and improved physical health. During a quarterly assessment of readiness for transition, it is determined that Jane has not yet met the criteria under the substance use , social relationships , and financial & income stability domains. She is meeting all other transition criteria. When explored with Jane, the team learns: Jane is avoiding past friends that she used with because she wants to become sober she has not yet made any sober friends. Jane experiences periodic substance use relapses which impact her finances she doesn t have money for social activities. (1-2 times per month meth use which she reports helps her focus at work.) Jane s most recent E-IMR goal is to make a new friend. If the transition checklist looks for a 12 month period of stability in all domains, what would be the next steps for Jane in her work with the ACT team?
Identifying Individuals Ready for Transition Transition planning can begin with the individual is has met or is close to meeting: Criteria on checklist Individually important criteria Personally important goals Individual and the ACT team mutually agree to plan for transition out of ACT services Note: circumstances may change during transition planning process, which could indicate need for continued ACT services Avoid graduating individuals from ACT prematurely (revolving door)
Planning for Transition Gradual transition from ACT services with assured continuity of care Ideally occurs over 3-6 months Documented transition plan which participant and team have agreed to, which includes: Any remaining goals to be met prior to transition Plan for reducing ACT services As community integration increases it is not uncommon for services to naturally decrease over a period of time Which services may still need to reduced Over what period of time services will be reduced Where individual will access services post transition Overlapping service period (ACT and new provider) Plan for ACT team to monitor transition (60 days)
Maintaining Contact OCEACT recommends maintaining contact with the ACT participant to ensure a successful transition for at least 60 days post transition Plan for contact Contact person(s) Frequency of contact Type of contact Documentation Not just for reviews: Future treatment providers (continuity of care) Participant / family Legal
Assessing Need for ACT Services Post Transition Individual may return to ACT services if the individual was discharged from ACT within the past twelve (12) months and any of the following has occurred, or the individual is at risk of the following: A psychiatric hospitalization, admission to an acute / sub- acute psychiatric facility, or use of psychiatric emergency services A hospitalization or an emergency room visit as a result of substance abuse An arrest or other law enforcement contact Homelessness or housing instability Keep program capacity in mind
Documentation Individual criteria being assessed for each participant Participant has an active role in defining how they want their life to look Assessments for transition readiness conducted over time Clearly documented transition plan Participant actively defines what transition will look like Specific timeframes Plan includes: Any remaining goals to be met prior to transition Plan for reducing ACT services Where individual will access services post transition Overlapping service period (ACT and new provider) Plan for ACT team to monitor transition (60 days) Progress notes Document participant s role in transition planning Show that transition is planned and gradual based on reduced service need Needs and progress documented in notes is consistent with transition assessments
References Cuddeback, G.S. (2011). The Assertive Community Treatment Transition Readiness Scale User Manual. http://www.eastpointe.net/providers/providerforms/networkoperations/A TR%20User's%20Manual%202011.pdf Donahue, SA; Manuel JI, Herman DB, Fraser LH, Chen H, Essock SM. (2012). Development and use of a transition readiness scale to help manage ACT team capacity. Psychiatric Services: 63(3) 223-9. http://ps.psychiatryonline.org/doi/full/10.1176/appi.ps.201100041 Herman DS, Conover S, Gorroochurn P, et al. (2011). Randomized trial of critical time intervention to prevent homelessness after hospital discharge. Psychiatric Services 62: 713 719 Kortrijk1, Hans, Kamperman, Astrid, Mulder, Cornelis. (2014). Changes in individual needs for care and quality of life in Assertive Community Treatment patients: an observational study. BMC Psychiatry: 14:306 http://bmcpsychiatry.biomedcentral.com/articles/10.1186/s12888-014- 0306-8