Pharmacogenomics Report for Patient BBS-001
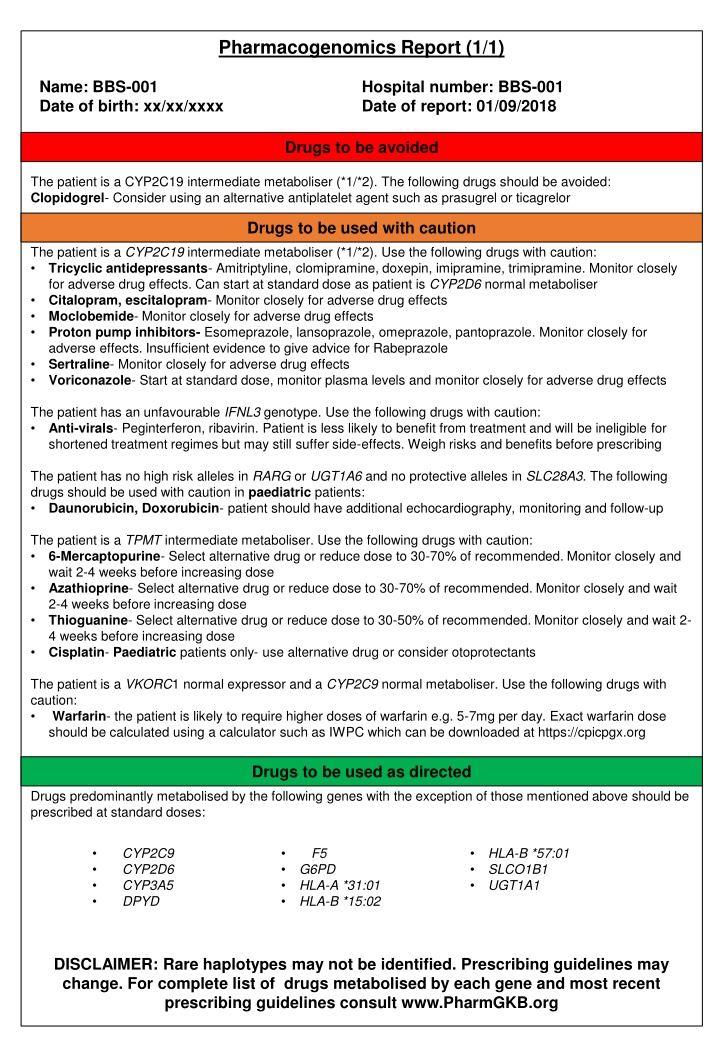
This pharmacogenomics report for patient BBS-001 reveals the patient's genotype information and provides guidance on drug usage. Drugs to be avoided, used with caution, and used as directed are clearly outlined based on the patient's metabolic profile. Recommendations for specific medications and monitoring strategies are provided to optimize treatment efficacy and safety.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Pharmacogenomics Report (1/1) Name: BBS-001 Date of birth: xx/xx/xxxx Hospital number: BBS-001 Date of report: 01/09/2018 Drugs to be avoided The patient is a CYP2C19 intermediate metaboliser (*1/*2). The following drugs should be avoided: Clopidogrel- Consider using an alternative antiplatelet agent such as prasugrel or ticagrelor Drugs to be used with caution The patient is a CYP2C19 intermediate metaboliser (*1/*2). Use the following drugs with caution: Tricyclic antidepressants- Amitriptyline, clomipramine, doxepin, imipramine, trimipramine. Monitor closely for adverse drug effects. Can start at standard dose as patient is CYP2D6 normal metaboliser Citalopram, escitalopram- Monitor closely for adverse drug effects Moclobemide- Monitor closely for adverse drug effects Proton pump inhibitors- Esomeprazole, lansoprazole, omeprazole, pantoprazole. Monitor closely for adverse effects. Insufficient evidence to give advice for Rabeprazole Sertraline- Monitor closely for adverse drug effects Voriconazole- Start at standard dose, monitor plasma levels and monitor closely for adverse drug effects The patient has an unfavourable IFNL3 genotype. Use the following drugs with caution: Anti-virals- Peginterferon, ribavirin. Patient is less likely to benefit from treatment and will be ineligible for shortened treatment regimes but may still suffer side-effects. Weigh risks and benefits before prescribing The patient has no high risk alleles in RARG or UGT1A6 and no protective alleles in SLC28A3. The following drugs should be used with caution in paediatric patients: Daunorubicin, Doxorubicin- patient should have additional echocardiography, monitoring and follow-up The patient is a TPMT intermediate metaboliser. Use the following drugs with caution: 6-Mercaptopurine- Select alternative drug or reduce dose to 30-70% of recommended. Monitor closely and wait 2-4 weeks before increasing dose Azathioprine- Select alternative drug or reduce dose to 30-70% of recommended. Monitor closely and wait 2-4 weeks before increasing dose Thioguanine- Select alternative drug or reduce dose to 30-50% of recommended. Monitor closely and wait 2- 4 weeks before increasing dose Cisplatin- Paediatric patients only- use alternative drug or consider otoprotectants The patient is a VKORC1 normal expressor and a CYP2C9 normal metaboliser. Use the following drugs with caution: Warfarin- the patient is likely to require higher doses of warfarin e.g. 5-7mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP2C9 CYP2D6 CYP3A5 DPYD F5 HLA-B *57:01 SLCO1B1 UGT1A1 G6PD HLA-A *31:01 HLA-B *15:02 DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (1/1) Name: BBS-002 Date of birth: xx/xx/xxxx Hospital number: BBS-002 Date of report: 01/09/2018 Drugs to be avoided The patient is a CYP2C19 intermediate metaboliser (*1/*2). The following drugs should be avoided: Clopidogrel- Consider using an alternative antiplatelet agent such as prasugrel or ticagrelor Drugs to be used with caution The patient is a CYP2C19 intermediate metaboliser (*1/*2). Use the following drugs with caution: Tricyclic antidepressants- Amitriptyline, clomipramine, doxepin, imipramine, trimipramine. Monitor closely for adverse drug effects. Can start at standard dose as patient is CYP2D6 normal metaboliser Citalopram, escitalopram- Monitor closely for adverse drug effects Moclobemide- Monitor closely for adverse drug effects Proton pump inhibitors- Esomeprazole, lansoprazole, omeprazole, pantoprazole. Monitor closely for adverse effects. Insufficient evidence to give advice for Rabeprazole Sertraline- Monitor closely for adverse drug effects Voriconazole- Start at standard dose, monitor plasma levels and monitor closely for adverse drug effects The patient is a CYP2C9 intermediate metaboliser (*1/*2). Use the following drugs with caution: Acenocoumarol- increase frequency of INR checks after initiation or discontinuation of NSAIDs Phenprocoumon- Monitor for adverse drug effects Phenytoin- consider 25% dose reduction and monitor closely Sulfonylureas- glibenclamide, gliclazide, glimepiride, tolbutamide. Monitor blood glucose levels The patient has an unfavourable IFNL3 genotype. Use the following drugs with caution: Anti-virals- Peginterferon, ribavirin. Patient is less likely to benefit from treatment and will be ineligible for shortened treatment regimes but may still suffer side-effects. Weigh risks and benefits before prescribing The patient has no high risk alleles in RARG or UGT1A6 and no protective alleles in SLC28A3. The following drugs should be used with caution in paediatric patients: Daunorubicin, Doxorubicin- patient should have additional echocardiography, monitoring and follow-up Patient is a UGT1A1 intermediate metaboliser. Use the following drugs with caution: Atazanavir- prescribe at standard dose but warn of possible side effects and monitor closely for adverse drug effects Irinotecan- For standard dosing (180-230mg/m2) and intensification regimes (>230mg/m2) there should be rigorous biological and clinical surveillance. Dose may need to be reduced The patient is a VKORC1 normal expressor and a CYP2C9 intermediate metaboliser. Use the following drugs with caution: Warfarin- the patient is likely to require higher doses of warfarin e.g. 5-7mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP2C19 CYP2D6 CYP3A5 DPYD F5 G6PD HLA-A *31:01 HLA-B *15:02 HLA-B *57:01 SLCO1B1 DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (1/1) Name: BBS-003 Date of birth: xx/xx/xxxx Hospital number: BBS-003 Date of report: 01/09/2018 Drugs to be avoided The patient is a CYP2C19 intermediate metaboliser (*1/*2). The following drugs should be avoided: Clopidogrel- Consider using an alternative antiplatelet agent such as prasugrel or ticagrelor Drugs to be used with caution The patient is a CYP2C19 intermediate metaboliser (*1/*2). Use the following drugs with caution: Tricyclic antidepressants- Amitriptyline, clomipramine, doxepin, imipramine, trimipramine. Monitor closely for adverse drug effects. Can start at standard dose as patient is CYP2D6 normal metaboliser Citalopram, escitalopram- Monitor closely for adverse drug effects Moclobemide- Monitor closely for adverse drug effects Proton pump inhibitors- Esomeprazole, lansoprazole, omeprazole, pantoprazole. Monitor closely for adverse effects. Insufficient evidence to give advice for Rabeprazole Sertraline- Monitor closely for adverse drug effects Voriconazole- Start at standard dose, monitor plasma levels and monitor closely for adverse drug effects The patient has no high risk alleles in RARG or UGT1A6 and no protective alleles in SLC28A3. The following drugs should be used with caution in paediatric patients: Daunorubicin, Doxorubicin- patient should have additional echocardiography, monitoring and follow-up The patient is a VKORC1 intermediate expressor and a CYP2C9 normal metaboliser. Use the following drugs with caution: Warfarin- the patient is likely to require higher doses of warfarin e.g. 5-7mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP2C9 CYP2D6 CYP3A5 DPYD F5 G6PD HLA-A *31:01 HLA-B *15:02 HLA-B *57:01 IFNL3 SLCO1B1 TPMT UGT1A1 DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (1/1) Name: BBS-004 Date of birth: xx/xx/xxxx Hospital number: BBS-004 Date of report: 01/09/2018 Drugs to be avoided The patient is a CYP2C19 intermediate metaboliser (*1/*2). The following drugs should be avoided: Clopidogrel- Consider using an alternative antiplatelet agent such as prasugrel or ticagrelor Drugs to be used with caution The patient is a CYP2C19 intermediate metaboliser (*1/*2). Use the following drugs with caution: Tricyclic antidepressants- Amitriptyline, clomipramine, doxepin, imipramine, trimipramine. Monitor closely for adverse drug effects. Can start at standard dose as patient is CYP2D6 normal metaboliser Citalopram, escitalopram- Monitor closely for adverse drug effects Moclobemide- Monitor closely for adverse drug effects Proton pump inhibitors- Esomeprazole, lansoprazole, omeprazole, pantoprazole. Monitor closely for adverse effects. Insufficient evidence to give advice for Rabeprazole Sertraline- Monitor closely for adverse drug effects Voriconazole- Start at standard dose, monitor plasma levels and monitor closely for adverse drug effects The patient is a CYP2C9 intermediate metaboliser (*1/*2). Use the following drugs with caution: Acenocoumarol- increase frequency of INR checks after initiation or discontinuation of NSAIDs Phenprocoumon- Monitor for adverse drug effects Phenytoin- consider 25% dose reduction and monitor closely Sulfonylureas- glibenclamide, gliclazide, glimepiride, tolbutamide. Monitor blood glucose levels The patient is a SLCO1B1 intermediate metaboliser. Use the following drugs with caution: Simvastatin- Prescribe lower dose and consider alternative e.g. pravastatin if lower dose not efficacious Patient is a UGT1A1 intermediate metaboliser. Use the following drugs with caution: Atazanavir- prescribe at standard dose but warn of possible side effects and monitor closely for adverse drug effects Irinotecan- For standard dosing (180-230mg/m2) and intensification regimes (>230mg/m2) there should be rigorous biological and clinical surveillance. Dose may need to be reduced The patient has no high risk alleles in RARG or UGT1A6 and no protective alleles in SLC28A3. The following drugs should be used with caution in paediatric patients: Daunorubicin, Doxorubicin- patient should have additional echocardiography, monitoring and follow-up The patient is a VKORC1 normal expressor and a CYP2C9 intermediate metaboliser. Use the following drugs with caution: Warfarin- the patient is likely to require higher doses of warfarin e.g. 5-7mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP2D6 CYP3A5 DPYD F5 G6PD HLA-A *31:01 HLA-B *15:02 HLA-B *57:01 IFNL3 TPMT DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (1/1) Name: BBS-005 Date of birth: xx/xx/xxxx Hospital number: BBS-005 Date of report: 01/09/2018 Drugs to be avoided The patient is a UGT1A1 poor metaboliser (*28/*28). Avoid the following drugs: Atazanavir- use alternative antiviral Drugs to be used with caution The patient has no high risk alleles in RARG or UGT1A6 and no protective alleles in SLC28A3. The following drugs should be used with caution in paediatric patients: Daunorubicin, Doxorubicin- patient should have additional echocardiography, monitoring and follow-up The patient is a UGT1A1 poor metaboliser (*28/*28). Use the following drugs with caution: Irinotecan- if dose is greater than 250mg/kg, reduce dose by 30%. Avoid dose intensification. Monitor closely for adverse drug effects The patient is a VKORC1 low expressor. Use the following drugs with caution: Acenocoumarol, phenprocoumon- the standard dose may be prescribed but monitor closely for high INR and bleeding The patient is a VKORC1 low expressor and a CYP2C9 normal metaboliser. Use the following drugs with caution: Warfarin- the patient is likely to require intermediate doses of warfarin e.g. 3-4mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP2C219 CYP2C9 CYP2D6 CYP3A5 DPYD F5 G6PD HLA-A *31:01 HLA-B *15:02 HLA-B *57:01 INFL3 SLCO1B1 TPMT DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (1/1) Name: BBS-006 Date of birth: xx/xx/xxxx Hospital number: BBS-006 Date of report: 01/09/2018 Drugs to be avoided None Drugs to be used with caution The patient is a CYP2C9 intermediate metaboliser (*1/*2). Use the following drugs with caution: Acenocoumarol- increase frequency of INR checks after initiation or discontinuation of NSAIDs Phenprocoumon- Monitor for adverse drug effects Phenytoin- consider 25% dose reduction and monitor closely Sulfonylureas- glibenclamide, gliclazide, glimepiride, tolbutamide. Monitor blood glucose levels Patient is a UGT1A1 intermediate metaboliser. Use the following drugs with caution: Atazanavir- prescribe at standard dose but warn of possible side effects and monitor closely for adverse drug effects Irinotecan- For standard dosing (180-230mg/m2) and intensification regimes (>230mg/m2) there should be rigorous biological and clinical surveillance. Dose may need to be reduced The patient is a VKORC1 normal expressor and a CYP2C9 intermediate metaboliser. Use the following drugs with caution: Warfarin- the patient is likely to require higher doses of warfarin e.g. 5-7mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP2C19 CYP2D6 CYP3A5 DPYD F5 G6PD HLA-A *31:01 HLA-B *15:02 HLA-B *57:01 IFNL3 RARG SLC28A3 SLCO1B1 TPMT UGT1A6 DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (1/2) Name: BBS-007 Date of birth: xx/xx/xxxx Hospital number: BBS-007 Date of report: 01/09/2018 Drugs to be avoided The patient is a CYP2D6 poor metaboliser (*4/*4). The following drugs should be avoided: Opioids- avoid codeine, hydrocodone, oxycodone and tramadol Metoprolol- select alternate drug e.g. carvedilol or bisoprolol, especially if treating heart failure. If prescribing metoprolol reduce dose by 75% and be aware of risk of adverse drug effects Paroxetine- Consider alternative drug not predominantly metabolised by CYP2D6 or reduce dose by 50% and titrate to response Tricyclic antidepressants- these include amitriptyline, clomipramine, desipramine, doxepin, fluvoxamine, imipramine, nortriptyline. If prescribing tricyclic antidepressants reduce dose by at least 50% and plasma levels monitored (see www.pharmgkb.org for drug-specific guidance) Venlafaxine- Consider alternative e.g. sertraline, citalopram or if using venlafaxine monitor plasma O- desmethylvenlafaxine levels and adverse drug effects and adjust dose accordingly Drugs to be used with caution The patient is a CYP2D6 poor metaboliser (*4/*4). The following drugs should be used with caution: Aripiprazole- reduce dose to 67% of recommended daily dose Atomoxetine- monitor for adverse drug effects Carvedilol- monitor for adverse drug effects Clozapine- monitor for adverse drug effects Duloxetine- monitor for adverse drug effects Flecainide- Reduce dose by 50% monitor plasma drug levels and ECG Flupenthixol- monitor for adverse drug effects Haloperidol- Reduce dose by 50% or consider selecting alternative drug e.g. pimozide, quetiapine, olanzapine, clozapine, fluphenazine Mirtazapine- monitor for adverse drug effects Olanzapine- monitor for adverse drug effects Ondansetron/tropisetron- monitor for adverse drug effects Propafenone- Reduce dose by 70% and monitor plasma drug levels and ECG Risperidone- Monitor plasma levels. Monitor for adverse drug effects and titrate to clinical response. Consider selecting alternative drug e.g. clozapine, quetiapine, olanzapine Tamoxifen- consider aromatase inhibitor in post-menopausal women Zuclopenthixol- Reduce dose by 50% and monitor for adverse drug effects. Alternatively consider another antiopsychotic such as flupenthixol, clozapine, olanzapine or quetiapine The patient has no high risk alleles in RARG or UGT1A6 and no protective alleles in SLC28A3. The following drugs should be used with caution in paediatric patients: Daunorubicin, Doxorubicin- patient should have additional echocardiography, monitoring and follow-up Patient is a UGT1A1 intermediate metaboliser. Use the following drugs with caution: Atazanavir- prescribe at standard dose but warn of possible side effects and monitor closely for adverse drug effects Irinotecan- For standard dosing (180-230mg/m2) and intensification regimes (>230mg/m2) there should be rigorous biological and clinical surveillance. Dose may need to be reduced The patient is a VKORC1 intermediate expressor and a CYP2C9 normal metaboliser. Use the following drugs with caution: Warfarin- the patient is likely to require higher doses of warfarin e.g. 5-7mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (2/2) Name: BBS-007 Date of birth: xx/xx/xxxx Hospital number: BBS-007 Date of report: 01/09/2018 Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP2C19 CYP2C9 CYP3A5 DPYD F5 G6PD HLA-A *31:01 HLA-B *15:02 HLA-B *57:01 IFNL3 SLCO1B1 TPMT DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (1/2) Name: BBS-008 Date of birth: xx/xx/xxxx Hospital number: BBS-008 Date of report: 01/09/2018 Drugs to be avoided The patient is a CYP2C19 rapid metaboliser (*1/*17). The following drugs should be avoided: Citalopram, escitalopram- Prescribe alternative drug e.g. fluoxetine. If prescribing, may require up to 150% of standard dose Tricyclic antidepressants- those metabolised by CYP2C19 include amitriptyline, clomipramine, doxepin, imipramine, trimipraminechoose an alternative drug not predominantly metabolised by CYP2C19 such as nortriptyline or desipramine. However, in this case as patient is CYP2D6 poor metaboliser, tricyclic antidepressants should be avoided if possible (see CYP2D6 below). Voriconazole- choose an alternative anti-fungal agent not predominantly metabolised by CYP2C19 such as isavuconazole, amphotericin B or posaconozole. If using Voriconazole, monitor serum levels The patient is a CYP2D6 poor metaboliser (*4/*4). The following drugs should be avoided: Opioids- avoid codeine, hydrocodone, oxycodone and tramadol Metoprolol- select alternate drug e.g. carvedilol or bisoprolol, especially if treating heart failure. If prescribing metoprolol reduce dose by 75% and be aware of risk of adverse drug effects Paroxetine- Consider alternative drug not predominantly metabolised by CYP2D6 or reduce dose by 50% and titrate to response Tricyclic antidepressants- these include amitriptyline, clomipramine, desipramine, doxepin, fluvoxamine, imipramine, nortriptyline. If prescribing tricyclic antidepressants reduce dose by at least 50% and plasma levels monitored (see www.pharmgkb.org for drug-specific guidance) Venlafaxine- Consider alternative e.g. sertraline, citalopram or if using venlafaxine monitor plasma O- desmethylvenlafaxine levels and adverse drug effects and adjust dose accordingly Drugs to be used with caution The patient is a CYP2C19 rapid metaboliser (*1/*17). The following drugs should be used with caution: Moclobemide- monitor for adverse drug effects Proton-pump inhibitors- For Helicobacter Pylori eradication therapy, increase dose by 50-100% (esomeprazole), by 200% (lansoprazole), by 100-200% (omeprazole) and by 400% (pantoprazole). Monitor closely for insufficient response. For indications other than H. Pylori eradication monitor for insufficient response and consider dose increase of 50-100% (esomeprazole), by 200% (lansoprazole), by 100-200% (omeprazole) and by 400% (pantoprazole) Sertraline- prescribe standard dose and if lack of therapeutic effect change to drug not predominantly metabolised by CYP2C19 The patient is a CYP2C9 intermediate metaboliser (*1/*3). The following drugs should be used with caution: Acenocoumarol- increase frequency of INR checks after initiation or discontinuation of NSAIDs Phenprocoumon- Monitor for adverse drug effects Phenytoin- consider 25% dose reduction and monitor closely Sulfonylureas- glibenclamide, gliclazide, glimepiride, tolbutamide. Monitor blood glucose levels The patient is a CYP2D6 poor metaboliser (*4/*4). The following drugs should be used with caution: Aripiprazole- reduce dose to 67% of recommended daily dose Atomoxetine- monitor for adverse drug effects Carvedilol- monitor for adverse drug effects Clozapine- monitor for adverse drug effects Duloxetine- monitor for adverse drug effects DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (2/2) Name: BBS-008 Date of birth: xx/xx/xxxx Hospital number: BBS-008 Date of report: 01/09/2018 Drugs to be used with caution (continued) The patient is a CYP2D6 poor metaboliser (*4/*4). The following drugs should be used with caution: Flecainide- Reduce dose by 50% monitor plasma drug levels and ECG Haloperidol- Reduce dose by 50% or consider selecting alternative drug e.g. pimozide, quetiapine, olanzapine, clozapine, fluphenazine Mirtazapine- monitor for adverse drug effects Olanzapine- monitor for adverse drug effects Ondansetron/tropisetron- monitor for adverse drug effects Propafenone- Reduce dose by 70% and monitor plasma drug levels and ECG Risperidone- Monitor plasma levels. Monitor for adverse drug effects and titrate to clinical response. Consider selecting alternative drug e.g. clozapine, quetiapine, olanzapine Tamoxifen- consider aromatase inhibitor in post-menopausal women Zuclopenthixol- Reduce dose by 50% and monitor for adverse drug effects. Alternatively consider another antiopsychotic such as flupenthixol, clozapine, olanzapine or quetiapine The patient is a CYP3A5 intermediate metaboliser (*1/*3). The following drugs should be used with caution: Tacrolimus: The patient is likely to require a 1.5-2-fold dose increase. Dose adjustments should be guided by therapeutic monitoring and the total daily dose should not exceed 0.3mg/kg/day The patient is a VKORC1 normal expressor and a CYP2C9 intermediate metaboliser (*1/*3). Use the following drugs with caution: Warfarin- the patient is likely to require intermediate doses of warfarin e.g. 3-4mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP3A5 DPYD F5 G6PD HLA-A *31:01 HLA-B *15:02 HLA-B *57:01 IFNL3 RARG SLC28A3 SLCO1B1 TPMT UGT1A1 UGT1A6 DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (1/1) Name: BBS-009 Date of birth: xx/xx/xxxx Hospital number: BBS-009 Date of report: 01/09/2018 Drugs to be avoided The patient is a CYP2C19 rapid metaboliser (*1/*17). The following drugs should be avoided: Tricyclic antidepressants- those metabolised by CYP2C19 include amitriptyline, clomipramine, doxepin, imipramine, trimipramine Voriconazole- choose an alternative anti-fungal agent not predominantly metabolised by CYP2C19 such as nortriptyline or desipramine Citalopram, escitalopram- Prescribe alternative drug e.g. fluoxetine. If prescribing, may require up to 150% of standard dose Voriconazole- choose an alternative anti-fungal agent not predominantly metabolised by CYP2C19 such as isavuconazole, amphotericin B or posaconozole. If using Voriconazole, monitor serum levels Drugs to be used with caution The patient is a CYP2C19 rapid metaboliser (*1/*17). The following drugs should be used with caution: Moclobemide- monitor for adverse drug effects Proton-pump inhibitors- For Helicobacter Pylori eradication therapy, increase dose by 50-100% (esomeprazole), by 200% (lansoprazole), by 100-200% (omeprazole) and by 400% (pantoprazole). Monitor closely for insufficient response. For indications other than H. Pylori eradication monitor for insufficient response and consider dose increase of 50-100% (esomeprazole), by 200% (lansoprazole), by 100-200% (omeprazole) and by 400% (pantoprazole) Sertraline- prescribe standard dose and if lack of therapeutic effect change to drug not predominantly metabolised by CYP2C19 The patient has a high risk allele in UGT1A6 and no protective alleles in SLC28A3. The following drugs should be used with caution in paediatric patients: Daunorubicin, Doxorubicin- Patient carries a high risk allele so management and follow up as follows: should be prescribed dexrasoxane (iron chelation), have serial echocardiography, aggressive management of cardiovascular risk factors, have liposomal anthracyclines prescribed and at lower rate of infusion. Use of other cardioprotective agents should be considered The patient is a VKORC1 low expressor. Use the following drugs with caution: Acenocoumarol, phenprocoumon- the standard dose may be prescribed but monitor closely for high INR and bleeding The patient is a VKORC1 low expressor and a CYP2C9 normal metaboliser. Use the following drugs with caution: Warfarin- the patient is likely to require intermediate doses of warfarin e.g. 3-4mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP2C9 CYP2D6 CYP3A5 DPYD F5 G6PD HLA-A *31:01 HLA-B *15:02 HLA-B *57:01 IFNL3 SLCO1B1 TPMT UGT1A1 DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (1/1) Name: BBS-010 Date of birth: xx/xx/xxxx Hospital number: BBS-010 Date of report: 01/09/2018 Drugs to be avoided The patient is a CYP2C19 rapid metaboliser (*1/*17). The following drugs should be avoided: Tricyclic antidepressants- those metabolised by CYP2C19 include amitriptyline, clomipramine, doxepin, imipramine, trimipramine Voriconazole- choose an alternative anti-fungal agent not predominantly metabolised by CYP2C19 such as nortriptyline or desipramine Citalopram, escitalopram- Prescribe alternative drug e.g. fluoxetine. If prescribing, may require up to 150% of standard dose Voriconazole- choose an alternative anti-fungal agent not predominantly metabolised by CYP2C19 such as isavuconazole, amphotericin B or posaconozole. If using Voriconazole, monitor serum levels The patient is a UGT1A1 poor metaboliser (*28/*28). Avoid the following drugs: Atazanavir- use alternative antiviral Drugs to be used with caution The patient is a CYP2C19 rapid metaboliser (*1/*17). The following drugs should be used with caution: Moclobemide- monitor for adverse drug effects Proton-pump inhibitors- For Helicobacter Pylori eradication therapy, increase dose by 50-100% (esomeprazole), by 200% (lansoprazole), by 100-200% (omeprazole) and by 400% (pantoprazole). Monitor closely for insufficient response. For indications other than H. Pylori eradication monitor for insufficient response and consider dose increase of 50-100% (esomeprazole), by 200% (lansoprazole), by 100-200% (omeprazole) and by 400% (pantoprazole) Sertraline- prescribe standard dose and if lack of therapeutic effect change to drug not predominantly metabolised by CYP2C19 The patient has an unfavourable IFNL3 genotype. Use the following drugs with caution: Anti-virals- Peginterferon, ribavirin. Patient is less likely to benefit from treatment and will be ineligible for shortened treatment regimes but may still suffer side-effects. Weigh risks and benefits before prescribing The patient is a UGT1A1 poor metaboliser (*28/*28). Use the following drugs with caution: Irinotecan- if dose is greater than 250mg/kg, reduce dose by 30%. Avoid dose intensification. Monitor closely for adverse drug effects The patient is a VKORC1 intermediate expressor and a CYP2C9 normal metaboliser. Use the following drugs with caution: Warfarin- the patient is likely to require higher doses of warfarin e.g. 5-7mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP2C9 CYP2D6 CYP3A5 DPYD F5 G6PD HLA-A *31:01 HLA-B *15:02 HLA-B *57:01 RARG SLC28A3 SLCO1B1 TPMT UGT1A6 DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (1/1) Name: BBS-011 Date of birth: xx/xx/xxxx Hospital number: BBS-011 Date of report: 01/09/2018 Drugs to be avoided The patient is a CYP2C19 rapid metaboliser (*1/*17). The following drugs should be avoided: Tricyclic antidepressants- those metabolised by CYP2C19 include amitriptyline, clomipramine, doxepin, imipramine, trimipramine. Choose an alternative drug not metabolised by CYP2C19 such as nortriptyline or desipramine Citalopram, escitalopram- Prescribe alternative drug e.g. fluoxetine. If prescribing, may require up to 150% of standard dose Voriconazole- choose an alternative anti-fungal agent not predominantly metabolised by CYP2C19 such as isavuconazole, amphotericin B or posaconozole. If using Voriconazole, monitor serum levels The patient is a UGT1A1 poor metaboliser (*28/*28). Avoid the following drugs: Atazanavir- use alternative antiviral Drugs to be used with caution The patient is a CYP2C19 rapid metaboliser (*1/*17). The following drugs should be used with caution: Moclobemide- monitor for adverse drug effects Proton-pump inhibitors- For Helicobacter Pylori eradication therapy, increase dose by 50-100% (esomeprazole), by 200% (lansoprazole), by 100-200% (omeprazole) and by 400% (pantoprazole). Monitor closely for insufficient response. For indications other than H. Pylori eradication monitor for insufficient response and consider dose increase of 50-100% (esomeprazole), by 200% (lansoprazole), by 100-200% (omeprazole) and by 400% (pantoprazole) Sertraline- prescribe standard dose and if lack of therapeutic effect change to drug not predominantly metabolised by CYP2C19 The patient has an unfavourable IFNL3 genotype. Use the following drugs with caution: Anti-virals- Peginterferon, ribavirin. Patient is less likely to benefit from treatment and will be ineligible for shortened treatment regimes but may still suffer side-effects. Weigh risks and benefits before prescribing The patient is a UGT1A1 poor metaboliser (*28/*28). Use the following drugs with caution: Irinotecan- if dose is greater than 250mg/kg, reduce dose by 30%. Avoid dose intensification. Monitor closely for adverse drug effects The patient is a VKORC1 intermediate expressor and a CYP2C9 normal metaboliser. Use the following drugs with caution: Warfarin- the patient is likely to require higher doses of warfarin e.g. 5-7mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP2C9 CYP2D6 CYP3A5 DPYD F5 G6PD HLA-A *31:01 HLA-B *15:02 HLA-B *57:01 RARG SLC28A3 SLCO1B1 TPMT UGT1A6 DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (1/1) Name: BBS-012 Date of birth: xx/xx/xxxx Hospital number: BBS-012 Date of report: 01/09/2018 Drugs to be avoided The patient is a CYP2C19 rapid metaboliser (*17/*17). The following drugs should be avoided: Tricyclic antidepressants- those metabolised by CYP2C19 include amitriptyline, clomipramine, doxepin, imipramine, trimipramine V choose an alternative drug not predominantly metabolised by CYP2C19 such as nortriptyline or desipramine Citalopram, escitalopram- Prescribe alternative drug e.g. fluoxetine. If prescribing, may require up to 150% of standard dose Voriconazole- choose an alternative anti-fungal agent not predominantly metabolised by CYP2C19 such as isavuconazole, amphotericin B or posaconozole. If using Voriconazole, monitor serum levels The patient is HLA-B *57:01 positive. The following drugs should be avoided Abacavir- choose alternative drug Drugs to be used with caution The patient is a CYP2C19 rapid metaboliser (*17/*17). The following drugs should be used with caution: Moclobemide- monitor for adverse drug effects Proton-pump inhibitors- For Helicobacter Pylori eradication therapy, increase dose by 50-100% (esomeprazole), by 200% (lansoprazole), by 100-200% (omeprazole) and by 400% (pantoprazole). Monitor closely for insufficient response. For indications other than H. Pylori eradication monitor for insufficient response and consider dose increase of 50-100% (esomeprazole), by 200% (lansoprazole), by 100-200% (omeprazole) and by 400% (pantoprazole) Sertraline- prescribe standard dose and if lack of therapeutic effect change to drug not predominantly metabolised by CYP2C19 The patient is a VKORC1 normal expressor and a CYP2C9 intermediate metaboliser. Use the following drugs with caution: Warfarin- the patient is likely to require higher doses of warfarin e.g. 5-7mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP2C9 CYP2D6 CYP3A5 DPYD F5 G6PD HLA-A *31:01 HLA-B *15:02 IFNL3 RARG SLC28A3 SLCO1B1 TPMT UGT1A1 UGT1A6 DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (1/2) Name: BBS-013 Date of birth: xx/xx/xxxx Hospital number: BBS-013 Date of report: 01/09/2018 Drugs to be avoided The patient is a CYP2C19 rapid metaboliser (*1/*17). The following drugs should be avoided: Citalopram, escitalopram- Prescribe alternative drug e.g. fluoxetine. If prescribing, may require up to 150% of standard dose Tricyclic antidepressants- those metabolised by CYP2C19 include amitriptyline, clomipramine, doxepin, imipramine, trimipraminechoose an alternative drug not predominantly metabolised by CYP2C19 such as nortriptyline or desipramine. However, in this case as patient is CYP2D6 poor metaboliser, tricyclic antidepressants should be avoided if possible (see CYP2D6 below). Voriconazole- choose an alternative anti-fungal agent not predominantly metabolised by CYP2C19 such as isavuconazole, amphotericin B or posaconozole. If using Voriconazole, monitor serum levels The patient is a CYP2D6 poor metaboliser (*4/*4). The following drugs should be avoided: Opioids- avoid codeine, hydrocodone, oxycodone and tramadol Metoprolol- select alternate drug e.g. carvedilol or bisoprolol, especially if treating heart failure. If prescribing metoprolol reduce dose by 75% and be aware of risk of adverse drug effects Paroxetine- Consider alternative drug not predominantly metabolised by CYP2D6 or reduce dose by 50% and titrate to response Tricyclic antidepressants- these include amitriptyline, clomipramine, desipramine, doxepin, fluvoxamine, imipramine, nortriptyline. Avoid if possible. If prescribing tricyclic antidepressants reduce dose by at least 50% and plasma levels monitored (see www.pharmgkb.org for drug-specific guidance) Venlafaxine- Consider alternative e.g. sertraline, citalopram or if using venlafaxine monitor plasma O- desmethylvenlafaxine levels and adverse drug effects and adjust dose accordingly The patient is HLA-B *57:01 positive. The following drugs should be avoided Abacavir- choose alternative drug Drugs to be used with caution The patient is a CYP2C19 rapid metaboliser (*1/*17). The following drugs should be used with caution: Moclobemide- monitor for adverse drug effects Proton-pump inhibitors- For Helicobacter Pylori eradication therapy, increase dose by 50-100% (esomeprazole), by 200% (lansoprazole), by 100-200% (omeprazole) and by 400% (pantoprazole). Monitor closely for insufficient response. For indications other than H. Pylori eradication monitor for insufficient response and consider dose increase of 50-100% (esomeprazole), by 200% (lansoprazole), by 100-200% (omeprazole) and by 400% (pantoprazole) Sertraline- prescribe standard dose and if lack of therapeutic effect change to drug not predominantly metabolised by CYP2C19 The patient is a CYP2C9 intermediate metaboliser (*1/*2). Use the following drugs with caution: Acenocoumarol- increase frequency of INR checks after initiation or discontinuation of NSAIDs Phenprocoumon- Monitor for adverse drug effects Phenytoin- consider 25% dose reduction and monitor closely Sulfonylureas- glibenclamide, gliclazide, glimepiride, tolbutamide. Monitor blood glucose levels DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (2/2) Name: BBS-013 Date of birth: xx/xx/xxxx Hospital number: BBS-013 Date of report: 01/09/2018 Drugs to be used with caution (continued) The patient is a CYP2D6 poor metaboliser (*4/*4). The following drugs should be used with caution: Aripiprazole- reduce dose to 67% of recommended daily dose Atomoxetine- monitor for adverse drug effects Carvedilol- monitor for adverse drug effects Clozapine- monitor for adverse drug effects Duloxetine- monitor for adverse drug effects Flecainide- Reduce dose by 50% monitor plasma drug levels and ECG Haloperidol- Reduce dose by 50% or consider selecting alternative drug e.g. pimozide, quetiapine, olanzapine, clozapine, fluphenazine Mirtazapine- monitor for adverse drug effects Olanzapine- monitor for adverse drug effects Ondansetron/tropisetron- monitor for adverse drug effects Propafenone- Reduce dose by 70% and monitor plasma drug levels and ECG Risperidone- Monitor plasma levels. Monitor for adverse drug effects and titrate to clinical response. Consider selecting alternative drug e.g. clozapine, quetiapine, olanzapine Tamoxifen- consider aromatase inhibitor in post-menopausal women Zuclopenthixol- Reduce dose by 50% and monitor for adverse drug effects. Alternatively consider another antiopsychotic such as flupenthixol, clozapine, olanzapine or quetiapine The patient has an unfavourable IFNL3 genotype. Use the following drugs with caution: Anti-virals- Peginterferon, ribavirin. Patient is less likely to benefit from treatment and will be ineligible for shortened treatment regimes but may still suffer side-effects. Weigh risks and benefits before prescribing The patient has no high risk alleles in RARG or UGT1A6 and no protective alleles in SLC28A3. The following drugs should be used with caution in paediatric patients: Daunorubicin, Doxorubicin- patient should have additional echocardiography, monitoring and follow-up The patient is a VKORC1 intermediate expressor and a CYP2C9 intermediate metaboliser. Use the following drugs with caution: Warfarin- the patient is likely to require intermediate doses of warfarin e.g. 3-4mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP3A5 DPYD F5 G6PD HLA-A *31:01 HLA-B *15:02 SLCO1B1 TPMT UGT1A1 DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (1/1) Name: BBS-014 Date of birth: xx/xx/xxxx Hospital number: BBS-014 Date of report: 01/09/2018 Drugs to be avoided The patient is a CYP2C19 intermediate metaboliser (*1/*2). The following drugs should be avoided: Clopidogrel- Consider using an alternative antiplatelet agent such as prasugrel or ticagrelor Drugs to be used with caution The patient is a CYP2C19 intermediate metaboliser (*1/*2). Use the following drugs with caution: Tricyclic antidepressants- Amitriptyline, clomipramine, doxepin, imipramine, trimipramine. Monitor closely for adverse drug effects. Can start at standard dose as patient is CYP2D6 normal metaboliser Citalopram, escitalopram- Monitor closely for adverse drug effects Moclobemide- Monitor closely for adverse drug effects Proton pump inhibitors- Esomeprazole, lansoprazole, omeprazole, pantoprazole. Monitor closely for adverse effects. Insufficient evidence to give advice for Rabeprazole Sertraline- Monitor closely for adverse drug effects Voriconazole- Start at standard dose, monitor plasma levels and monitor closely for adverse drug effects The patient is a CYP2C9 intermediate metaboliser (*1/*2). Use the following drugs with caution: Acenocoumarol- increase frequency of INR checks after initiation or discontinuation of NSAIDs Phenprocoumon- Monitor for adverse drug effects Phenytoin- consider 25% dose reduction and monitor closely Sulfonylureas- glibenclamide, gliclazide, glimepiride, tolbutamide. Monitor blood glucose levels The patient is a CYP3A5 intermediate metaboliser (*1/*3). The following drugs should be used with caution: Tacrolimus: The patient is likely to require a 1.5-2-fold dose increase. Dose adjustments should be guided by therapeutic monitoring and the total daily dose should not exceed 0.3mg/kg/day The patient has a high risk allele UGT1A6 and no protective alleles in SLC28A3. The following drugs should be used with caution in paediatric patients: Daunorubicin, Doxorubicin- Patient carries a high risk allele so management and follow up as follows: should be prescribed dexrasoxane (iron chelation, have serial echocardiography, aggressive management of cardiovascular risk factors, have liposomal anthracyclines prescribed and at lower rate of infusion. Use of other cardioprotective agents should be considered The patient is a VKORC1 normal expressor and a CYP2C9 intermediate metaboliser. Use the following drugs with caution: Warfarin- the patient is likely to require higher doses of warfarin e.g. 5-7mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP2D6 DPYD F5 G6PD HLA-A *31:01 HLA-B *15:02 HLA-B *57:01 IFNL3 SLCO1B1 TPMT UGT1A1 DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (1/1) Name: BBS-015 Date of birth: xx/xx/xxxx Hospital number: BBS-015 Date of report: 01/09/2018 Drugs to be avoided The patient is a CYP2C19 intermediate metaboliser (*1/*2). The following drugs should be avoided: Clopidogrel- Consider using an alternative antiplatelet agent such as prasugrel or ticagrelor Drugs to be used with caution The patient is a CYP2C19 intermediate metaboliser (*1/*2). Use the following drugs with caution: Tricyclic antidepressants- Amitriptyline, clomipramine, doxepin, imipramine, trimipramine. Monitor closely for adverse drug effects. Can start at standard dose as patient is CYP2D6 normal metaboliser Citalopram, escitalopram- Monitor closely for adverse drug effects Moclobemide- Monitor closely for adverse drug effects Proton pump inhibitors- Esomeprazole, lansoprazole, omeprazole, pantoprazole. Monitor closely for adverse effects. Insufficient evidence to give advice for Rabeprazole Sertraline- Monitor closely for adverse drug effects Voriconazole- Start at standard dose, monitor plasma levels and monitor closely for adverse drug effects The patient has an unfavourable IFNL3 genotype. Use the following drugs with caution: Anti-virals- Peginterferon, ribavirin. Patient is less likely to benefit from treatment and will be ineligible for shortened treatment regimes but may still suffer side-effects. Weigh risks and benefits before prescribing The patient has no high risk alleles in RARG or UGT1A6 and no protective alleles in SLC28A3. The following drugs should be used with caution in paediatric patients: Daunorubicin, Doxorubicin- patient should have additional echocardiography, monitoring and follow-up The patient is a TPMT intermediate metaboliser. Use the following drugs with caution: 6-Mercaptopurine- Select alternative drug or reduce dose to 30-70% of recommended. Monitor closely and wait 2-4 weeks before increasing dose Azathioprine- Select alternative drug or reduce dose to 30-70% of recommended. Monitor closely and wait 2-4 weeks before increasing dose Thioguanine- Select alternative drug or reduce dose to 30-50% of recommended. Monitor closely and wait 2- 4 weeks before increasing dose Cisplatin- Paediatric patients only- use alternative drug or consider otoprotectants The patient is a VKORC1 normal expressor and a CYP2C9 normal metaboliser. Use the following drugs with caution: Warfarin- the patient is likely to require higher doses of warfarin e.g. 5-7mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP2C9 CYP2D6 CYP3A5 DPYD F5 G6PD HLA-A *31:01 HLA-B *15:02 HLA-B *57:01 SLCO1B1 UGT1A1 DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (1/1) Name: BBS-016 Date of birth: xx/xx/xxxx Hospital number: BBS-016 Date of report: 01/09/2018 Drugs to be avoided None Drugs to be used with caution The patient is a CYP2C9 intermediate metaboliser (*1/*3). The following drugs should be used with caution: Acenocoumarol- increase frequency of INR checks after initiation or discontinuation of NSAIDs Phenprocoumon- Monitor for adverse drug effects Phenytoin- consider 25% dose reduction and monitor closely Sulfonylureas- glibenclamide, gliclazide, glimepiride, tolbutamide. Monitor blood glucose levels The patient has an unfavourable IFNL3 genotype. Use the following drugs with caution: Anti-virals- Peginterferon, ribavirin. Patient is less likely to benefit from treatment and will be ineligible for shortened treatment regimes but may still suffer side-effects. Weigh risks and benefits before prescribing The patient has a high risk allele UGT1A6. The following drugs should be used with caution in paediatric patients: Daunorubicin, Doxorubicin- Patient carries a high risk allele so management and follow up as follows: should be prescribed dexrasoxane (iron chelation, have serial echocardiography, aggressive management of cardiovascular risk factors, have liposomal anthracyclines prescribed and at lower rate of infusion. Use of other cardioprotective agents should be considered Patient is a UGT1A1 intermediate metaboliser. Use the following drugs with caution: Atazanavir- prescribe at standard dose but warn of possible side effects and monitor closely for adverse drug effects Irinotecan- For standard dosing (180-230mg/m2) and intensification regimes (>230mg/m2) there should be rigorous biological and clinical surveillance. Dose may need to be reduced The patient is a VKORC1 intermediate expressor and a CYP2C9 intermediate metaboliser. Use the following drugs with caution: Warfarin- the patient is likely to require intermediate doses of warfarin e.g. 3-4mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP2C19 CYP2D6 CYP3A5 DPYD F5 G6PD HLA-A *31:01 HLA-B *15:02 HLA-B *57:01 SLCO1B1 TPMT DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (1/1) Name: BBS-017 Date of birth: xx/xx/xxxx Hospital number: BBS-0017 Date of report: 01/09/2018 Drugs to be avoided None Drugs to be used with caution The patient is a CYP2C9 intermediate metaboliser (*1/*3). The following drugs should be used with caution: Acenocoumarol- increase frequency of INR checks after initiation or discontinuation of NSAIDs Phenprocoumon- Monitor for adverse drug effects Phenytoin- consider 25% dose reduction and monitor closely Sulfonylureas- glibenclamide, gliclazide, glimepiride, tolbutamide. Monitor blood glucose levels The patient has an unfavourable IFNL3 genotype. Use the following drugs with caution: Anti-virals- Peginterferon, ribavirin. Patient is less likely to benefit from treatment and will be ineligible for shortened treatment regimes but may still suffer side-effects. Weigh risks and benefits before prescribing The patient has a high risk allele UGT1A6. The following drugs should be used with caution in paediatric patients: Daunorubicin, Doxorubicin- Patient carries a high risk allele so management and follow up as follows: should be prescribed dexrasoxane (iron chelation, have serial echocardiography, aggressive management of cardiovascular risk factors, have liposomal anthracyclines prescribed and at lower rate of infusion. Use of other cardioprotective agents should be considered Patient is a UGT1A1 intermediate metaboliser. Use the following drugs with caution: Atazanavir- prescribe at standard dose but warn of possible side effects and monitor closely for adverse drug effects Irinotecan- For standard dosing (180-230mg/m2) and intensification regimes (>230mg/m2) there should be rigorous biological and clinical surveillance. Dose may need to be reduced The patient is a VKORC1 intermediate expressor and a CYP2C9 intermediate metaboliser. Use the following drugs with caution: Warfarin- the patient is likely to require intermediate doses of warfarin e.g. 3-4mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP2C19 CYP2D6 CYP3A5 DPYD F5 G6PD HLA-A *31:01 HLA-B *15:02 HLA-B *57:01 SLCO1B1 TPMT DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
Pharmacogenomics Report (1/1) Name: BBS-018 Date of birth: xx/xx/xxxx Hospital number: BBS-018 Date of report: 01/09/2018 Drugs to be avoided The patient is a UGT1A1 poor metaboliser (*28/*28). Avoid the following drugs: Atazanavir- use alternative antiviral Drugs to be used with caution The patient has no high risk alleles in RARG or UGT1A6 and no protective alleles in SLC28A3. The following drugs should be used with caution in paediatric patients: Daunorubicin, Doxorubicin- patient should have additional echocardiography, monitoring and follow-up The patient is a SLCO1B1 intermediate metaboliser. Use the following drugs with caution: Simvastatin- Prescribe lower dose and consider alternative e.g. pravastatin if lower dose not efficacious The patient is a TPMT intermediate metaboliser. Use the following drugs with caution: 6-Mercaptopurine- Select alternative drug or reduce dose to 30-70% of recommended. Monitor closely and wait 2-4 weeks before increasing dose Azathioprine- Select alternative drug or reduce dose to 30-70% of recommended. Monitor closely and wait 2-4 weeks before increasing dose Thioguanine- Select alternative drug or reduce dose to 30-50% of recommended. Monitor closely and wait 2- 4 weeks before increasing dose The patient is a UGT1A1 poor metaboliser (*28/*28). Use the following drugs with caution: Irinotecan- if dose is greater than 250mg/kg, reduce dose by 30%. Avoid dose intensification. Monitor closely for adverse drug effects The patient is a VKORC1 intermediate expressor and a CYP2C9 normal metaboliser. Use the following drugs with caution: Warfarin- the patient is likely to require higher doses of warfarin e.g. 5-7mg per day. Exact warfarin dose should be calculated using a calculator such as IWPC which can be downloaded at https://cpicpgx.org Drugs to be used as directed Drugs predominantly metabolised by the following genes with the exception of those mentioned above should be prescribed at standard doses: CYP2C19 CYP2C9 CYP2D6CYP3A5 DPYD F5 G6PD HLA-A *31:01 HLA-B *15:02 HLA-B *57:01 IFNL3 DISCLAIMER: Rare haplotypes may not be identified. Prescribing guidelines may change. For complete list of drugs metabolised by each gene and most recent prescribing guidelines consult www.PharmGKB.org
")
")
")
")
")
")
")
")
")
")
")
")
")
")
")
")
")
")
")
")
")