Learning from Collaborative Evaluation in India
 undefined
undefined

1
CONTEXT(S) MATTER:
Learning from Collaborative Evaluation in India

WHY CONTEXT?
Human Component-
Developmental Programs are
not mechanical
Micro vs Macro lens to program
development and evaluation
Realistic expectation of
program success
2
3
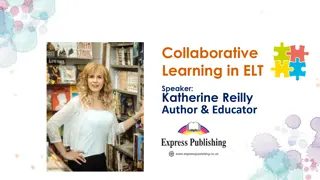
OUTCOME TRAJECTORY–
Taking the Context Lens
Fascination with Average-
Missing out on significant small
wins
Timelines of impact- a
dominant context
Making Course correction-
based on contextual outcomes
WHAT CAN BE COUNTED AS CONTEXT
?
4
Socio-
Demographic
Previous
Experience with
the
intervention(s)
Political/Policy
Priority
Crisis
/Ecological
challenges
Time to
adapt/Change
Organizational
Culture/Personal
Motivation
Community
Practices, belief,
& attitude
Leadership
Implementation
climate(Micro
level)
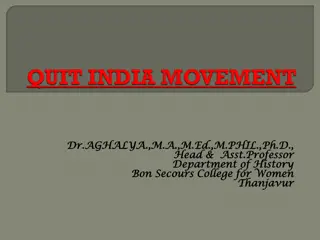
A CURIOUS CASE OF INFANT MORTALITY REDUCTION
5
Source: SRS, India
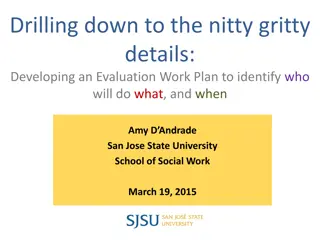
ZOOMING IN
6
Source: AHS 2012-13, India
Source: xMLE study 2019, UP
MEASUREMENT CHALLENGES–
FOR PROGRAM AND EVALUATIONS
Measurement and utilization of contexts are often
challenging for incorporation into Program design
and Evaluation
Unavailability of standard framework and standard
indicators
Realist Evaluation as an approach to incorporate
contexts in Evaluations
7
IMPLICATION
Incorporating contexts
in the program’s Theory
of Change
8
Looking from Below-
Collaborative learning with
Implementation teams
Exit strategy and
sustainability- Based on
contextual Success
CAN WE DECIDE SUCCESS?
Which one is more successful then other?
THANK YOU
10
APPENDIX
11
CONTEXT-MECHANISM-OUTCOMES: AN EXAMPLE
12
Population Demographic
•
Home to 235 million people, accounting for ~16% of the country’s
population
•
Approximately 30% of the population migrate within the state (Census
2012)
UP : SOCIAL AND HEALTH CONTEXT
What adds to the risk?
Nutrition and Food Security
•
46% U5 children are stunted, 40% underweight and 18% wasted (NFHS-4)
•
Per capita monthly expenditure on food – Rs 612 (rural) households, protein
intake is below RDA level even with PDS supplementation (MOPSI &WFP
2019)
Health Indicators (SRS-2018)
•
IMR-46 (rural) 35 (urban): death before the age of one-year per1,000 live
births
•
MMR: 197 deaths per 100,000 live births, maternal mortality rate of 17.1%
•
NMR- 31.7 (Global Burden of Disease Study, 2017)
13
Collaborative evaluation in India presents unique challenges and opportunities for program development and success. By understanding the context, such as previous experiences, socio-demographic factors, and organizational culture, stakeholders can map outcomes effectively, make course corrections, and ensure sustainable impact. Measurement challenges exist when incorporating contexts into program design, necessitating realist evaluation approaches. Exit strategies and sustainability hinge on contextual success, emphasizing the importance of incorporating context into program strategies.

Uploaded on Mar 04, 2025 | 0 Views
Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
CONTEXT(S) MATTER: Learning from Collaborative Evaluation in India 1
WHY CONTEXT? Human Component- Developmental Programs are not mechanical Micro vs Macro lens to program development and evaluation Realistic expectation of program success 2
OUTCOME TRAJECTORYTaking the Context Lens Mapping Outcome of a Maternal Health intervention Fascination with Average- Missing out on significant small wins 70 60 50 Timelines of impact- a dominant context 40 30 20 Making Course correction- based on contextual outcomes 10 0 T-0 T-0 T-1 T-2 T-3 T-4 Average Cluster A Cluster B 3
WHAT CAN BE COUNTED AS CONTEXT? Time to Previous Experience with the intervention(s) adapt/Change Socio- Demographic Crisis /Ecological challenges Political/Policy Priority Organizational Culture/Personal Motivation Community Practices, belief, & attitude Implementation climate(Micro level) Leadership 4
A CURIOUS CASE OF INFANT MORTALITY REDUCTION Infant Mortality Rate 250 200 150 100 43 50 32 0 7 India UP Kerala Source: SRS, India 5
ZOOMING IN Home delivery- across geography 41.3 38.4 30.3 21.6 18 16.5 16.1 15.413.6 15.3 12.9 10.511.6 10.8 6.9 AGRA DIVISION Bareilly Pilibhit Allahabad Gonda Sonbhadra Mirzapur Budaun Rampur Shahjahanpur Balrampur Siddharthnagar Kaushambi Mahrajganj Sant_Kabir_Nagar Shrawasti JHANSI DIVISION Bareilly Allahabad Gonda Source: xMLE study 2019, UP Source: AHS 2012-13, India 6
MEASUREMENT CHALLENGES FOR PROGRAM AND EVALUATIONS Measurement and utilization of contexts are often challenging for incorporation into Program design and Evaluation Unavailability of standard framework and standard indicators Realist Evaluation as an approach to incorporate contexts in Evaluations 7
IMPLICATION Exit strategy and sustainability- Based on contextual Success Incorporating contexts in the program s Theory of Change Looking from Below- Collaborative learning with Implementation teams
CAN WE DECIDE SUCCESS? Which one is more successful then other? CLUSTER 1 CLUSTER 2 CLUSTER 3 40 40 40 35 35 35 30 30 30 25 25 25 20 20 20 15 15 15 10 10 10 5 5 5 0 0 0 T0 T1 T2 T3 T0 T1 T2 T3 T0 T1 T2 T3
THANK YOU 10
APPENDIX 11
CONTEXT-MECHANISM-OUTCOMES: AN EXAMPLE Did it work? How did it work? Who did it work for? In what context did it work? Did the intervention lead to the desired outcomes? e.g. improvements practices on complication managements referral Underlying mechanisms that worked for the intervention e.g- the NM and trained doctors at the CEmONC facilities mentoring and hand holding support focused complications SNs, MoICs Where excellent with SNs and the facility had a supportive MoIC towards NM intervention NMs relationship had - - - - in provided and on 12
UP : SOCIAL AND HEALTH CONTEXT Population Demographic Home to 235 million people, accounting for ~16% of the country s population Approximately 30% of the population migrate within the state (Census 2012) What adds to the risk? Nutrition and Food Security 46% U5 children are stunted, 40% underweight and 18% wasted (NFHS-4) Per capita monthly expenditure on food Rs 612 (rural) households, protein intake is below RDA level even with PDS supplementation (MOPSI &WFP 2019) Health Indicators (SRS-2018) IMR-46 (rural) 35 (urban): death before the age of one-year per1,000 live births MMR: 197 deaths per 100,000 live births, maternal mortality rate of 17.1% NMR- 31.7 (Global Burden of Disease Study, 2017) 13
 MATTER:")