Exploring Personalised Care in London

1

PERSONALISED CARE
FOR
LONDON
E
m
b
e
d
d
i
n
g
t
h
e
3
p
e
r
s
o
n
a
l
i
s
e
d
c
a
r
e
A
R
R
S
r
o
l
e
s

@SP_LDN
hlp.socialprescribing@nhs.net


2
Plan for today...
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
It is an informal session – talk
to each other & share
resources in the chat
The presentations will be
recorded & circulated with slides
3
PCN Advisors – working 2 days a week until Apr 22
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
Purpose of the role:
•
Supporting PCNS to successfully embed the three, personalised care roles (Social Prescribing Link
Workers, Health & Wellbeing Coaches and Care Coordinators) to effectively tackle health inequalities
and support primary care
•
Build a network of those that employ or are working to embed the three personalised care roles in their
work, facilitating a community of practice across London
Dr Hina Shahid
Hina is a Portfolio GP in North West London and has a
background in Public Health. She has worked in the VCSE
sector for 15 years in community engagement, outreach and
health inclusion, and health systems strengthening in the UK
and internationally. She is an undergraduate tutor, GP
Appraiser and also works in social research and health policy
and has supported SPLWs in thinking through culturally
appropriate practice
Lianna Martin
With over 20 years experience in the VCSE and
social enterprise sector, developing projects and
partnership work, and previously at the Bromley by Bow
Centre, Lianna is also a Regional Learning Coordinator for
Social Prescribing and a Programme Manager at HLP in the
Health Inequalities, Personalised Care team. Her time is
dedicated to pan London initiatives supporting the
development of social prescribing, enabling it to thrive
4
Personalised care for London
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
What it is:
“
Personalised care
means people have choice and control over the way their care is
planned and delivered. It is based on ‘what matters’ to them and their individual strengths
and needs.”
Person
centred
care strives to see an individual as bio-psycho-social whole, as a person
and not a disease or a collection of conditions.
C
o
m
m
i
t
m
e
n
t
i
n
N
H
S
L
o
n
g
T
e
r
m
P
l
a
n
:
Put in place more than 1,000
Social Prescribing link workers
by the end of 2020/21, rising
further by 2023/24, with the aim that more than 900,000 people are connected to wider
community services that can help improve health and well-being.
For London this means working towards
800 SPLWs operating by 23-24
= approx. 4 per PCN of average population of 50,000
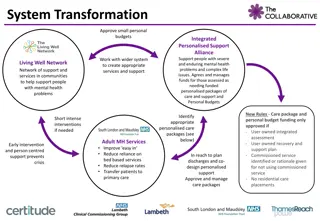
Vision for London:
Commitment to expanding Social
Prescribing in all 5 ICS operating
across the region
Core element of the
London Vision
and GLA’s
COVID recovery plan
–
to be joined up working at a
neighbourhood level, taking an
asset-based approach
and co-
creating
solutions
5
Why is it important?
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
•
5 London boroughs in top 10% most deprived boroughs in UK – PC role intrinsic tool for PCNs in community recovery
•
Uses appropriate team according local population needs & ensure roles working together, embedded in PCNs and
being used in the right way
•
Impact these roles can have on patients, community & surgeries can be significant
•
Significant ARRS underspend in London – funding & support available to grow these teams
Personalised care
is one of the five major,
practical changes to the NHS that will take place
over the next five years, as set out the recently
published
Long Term Plan
(Jan 2019).
Universal Personalised Care was written into an
implementation or
action plan for the rolling out
personalised care across England, to
reach 2.5
million people by 2023/24 and then aim to
double that again within a decade.
6
Health inequalities, inequities and primary care
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
•
Over 80% of health outcomes are socially determined
•
Inequities: systematic, avoidable and unfair differences in mental or physical health between
groups of people
•
Health disparities are widening in the UK- highest in London
•
COVID-19: vital community health function of general practice (RCGP)
•
The exceptional potential of PCNs- “anchor institutions”
•
Address and optimise individual and population health outcomes
•
Drive engagement between primary care and communities
•
Cross-sector working
7
Key areas of health disparities
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
8
Social determinants of health
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
•
Cross-sector
•
Multi agency
•
Joined up care
•
Partnership working
•
Co-production of services and resources
•
Outreach
•
Empowerment
•
Focus on individuals, communities and
their environment
Dahlgreen & Whitehead, 1991
9
Integrated care systems
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
•
Part of LTP
•
Fundamental shift in the way the health and care system is organised- move away from organisational
competition and the separation of commissioners and providers to focus on collaboration and on
places and local populations as the driving forces for improvement
•
Central aim of ICSs is to integrate care across different organisations and settings, joining up hospital
and community-based services, physical and mental health, and health and social care
•
greater integration of health and care services
•
improving population health and reducing inequalities
•
supporting productivity and sustainability of services
•
helping the NHS to support social and economic development
•
Case for collaborative, cross sector partnership working strengthened by experiences of Covid-19
pandemic
•
Statutory April 2022
•
Local contextualised arrangements- focus on local needs and resources and local leadership
10
What the roles do...
@SP_LDN
hlp.socialprescribing@nhs.net
11
Ensuring the personalised care roles work effectively together
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
12
Referrals into the system
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
•
First point of referral can be any of the three, this varies across services and depends on the presenting problem.
•
For example, some services might use the SPLW as an initial gatekeeper for referrals to all three workers, whereas some
PCNs might only have one of the roles in post so direct referral is necessary.
•
Can refer to each other and good communication between 3 roles is essential.
P
r
o
-
a
c
t
i
v
e
c
a
s
e
i
d
e
n
t
i
f
i
c
a
t
i
o
n
R
e
f
e
r
r
a
l
s
GPs
Pharmacist
Receptionist
Community
13
Optimising individual and population health and wellbeing
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
SPLWs
•
Range of positive health outcomes, reduced isolation, inc. independence
•
Rotherham: 80% improvement LTCs, 90% for mental health users
Care coordinators
•
LTCs and vulnerable/ excluded groups- deprivation, ethnic minority, disabilities, LGBTQ
•
Case finding – unmet needs
•
Coordinating care across sectors, MDTs, recalls, screening, care planning, annual reviews
Health and wellbeing coaches
•
Health creation: control, contact, confidence (The Health Creation Alliance)
•
Motivation and achieve health goals
•
Preventing illness
•
Empowering self supported management
14
Supporting the clinical workforce
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
•
~ 20% GP time spent on non—health matters
•
higher
in deprived areas
•
80% GPs report that dealing with non-health issues -> reduced time to treat
patient’s health issues
•
Release non-medical GP appointments
•
Ensure patients get appropriate support– right place, right person, right time
•
Addressing root causes reduces demand for services
15
The positive impact...
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
2017 University of Westminster review
•
average 28% reduction in demand for GP services
•
24% fall in A&E attendance for patients referred to a social
prescribing scheme.
•
fewer hospital admissions and A&E attendances
•
fewer outpatient appointments
•
fewer GP consultations
•
reduced reliance on medical prescriptions
•
effective in reducing demand on primary and secondary care.
2016 study in Rotherham
•
non-elective inpatient episodes reduced by 75%,
•
non-elective inpatient spells reduced by 11%
•
A&E attendances reduced by 17%.
2014 study from the University of East London and City and Hackney CCG
•
25% reduction in A&E attendance in their social prescribing group vs 66%
increase in A&E attendance by the control group
•
Hospital admissions
•
A&E attendance
•
Non-elective inpatient episodes
•
GP consultations
•
Reliance on prescriptions
•
Self-reported measures of health
and wellbeing
16
Evaluating cost effectiveness...
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
Social Return on Investment (SROI)
•
Conservative estimate £1: £3.52
•
Long term period £1: £5.77
•
For mental wellbeing £1: £8.56
QALY
•
Meets NICE thresholds for cost- effectiveness in studies
17
What is working...
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
•
G
i
v
e
t
h
e
s
e
r
o
l
e
s
T
I
M
E
•
to spend with patients – e.g. caseloads of 200 – 250 per year depending on
complexity for SPLWs for example
•
to build a meaningful bridge between primary care and the community,
scope appropriate activities, influencing development etc.
•
to proactively reach out to cohorts of patients experiencing health
inequalities and most in need of this support
•
to connect with each other, access peer support and ongoing training and
development
•
E
m
b
e
d
t
h
e
s
e
r
o
l
e
s
w
i
t
h
i
n
P
C
N
t
e
a
m
s
–
a
t
t
e
n
d
i
n
g
M
D
T
m
e
e
t
s
w
i
l
l
e
n
a
b
l
e
a
h
o
l
i
s
t
i
c
a
p
p
r
o
a
c
h
t
o
s
u
p
p
o
r
t
i
n
g
p
a
t
i
e
n
t
s
w
i
t
h
c
o
m
p
l
e
x
n
e
e
d
s
•
E
n
s
u
r
e
t
h
e
t
h
r
e
e
r
o
l
e
s
a
r
e
w
o
r
k
i
n
g
e
f
f
e
c
t
i
v
e
l
y
t
o
g
e
t
h
e
r
s
o
t
h
e
y
a
r
e
b
e
i
n
g
u
s
e
d
t
o
t
h
e
i
r
g
r
e
a
t
e
s
t
v
a
l
u
e
•
E
n
s
u
r
e
t
h
e
r
e
i
s
a
r
o
b
u
s
t
p
l
a
n
i
n
p
l
a
c
e
,
w
i
t
h
i
n
d
u
c
t
i
o
n
&
c
l
e
a
r
j
o
b
r
o
l
e
s
•
C
o
m
m
u
n
i
c
a
t
e
t
o
t
h
e
w
i
d
e
r
r
e
f
e
r
r
i
n
g
w
o
r
k
f
o
r
c
e
,
t
h
e
p
u
r
p
o
s
e
o
f
t
h
e
r
o
l
e
s
a
n
d
h
o
w
t
h
e
y
c
a
n
b
e
n
e
f
i
t
t
h
e
w
o
r
k
o
f
t
h
e
w
i
d
e
r
p
r
a
c
t
i
c
e
A one team approach for
personalised care roles
•
to support and develop each role
•
to work together on shared goals
and outcomes
•
manage and benefit from role
interdependencies
•
combine traditional and place-
based MDT models
18
Examples of good practice in PCNs
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
•
Open and transparent
•
Clear values and purpose in a coherent system
•
Diverse governance and leadership – not just GPs
•
Executive committee/clinical cabinet, buddying with
other local PCNs
•
Focus on partnership working, shared decision making
•
Understand DES and use it to align with local needs and
priorities incl. health disparities
•
Intelligence driven population health management
•
Health inequalities lead and/or personalised care
champions
•
Understands 3 PC roles with clear and consistent referral
criteria
•
Forward thinking and developing a one team approach
•
Focused not just on outcomes but also experience
•
Multi agency, place based MDTs
•
Understand and work to overcome barriers to access
for vulnerable and excluded groups by working with
community- based partners and embedding an
asset—based approach
•
Shift to community-led community development
and a strategy/ community development specialist
to link PCNs and community partners
•
Empowering communities to address wellbeing
themselves through supported self management
•
Supporting professional development and
supervision of ARRS roles and considering team
leader / complex case manager
•
Service pathways co-produced with local partners to
meet diverse needs- social, economic, material,
cultural as well as medical
•
Evaluate, reflect, learn, share and embed
19
Support available in London
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
H
L
P
P
e
r
s
o
n
a
l
i
s
e
d
C
a
r
e
T
e
a
m
Supporting the London system to spread and scale personalised care
Convening multisector partnership work to support, develop and innovate social prescribing
N
H
S
E
A
s
s
o
c
i
a
t
e
r
o
l
e
s
s
u
p
p
o
r
t
i
n
g
f
r
o
n
t
l
i
n
e
s
t
a
f
f
Regional Learning Coordinator for Social Prescribing – Lianna Martin: lianna.martin@nhs.net
Health and Wellbeing Coach Mentor – Caroline Haines: caroline.haines1@nhs.net
Care Coordinator Mentor – Ali Hassas: alihassas@nhs.net
N
H
S
E
A
s
s
o
c
i
a
t
e
r
o
l
e
s
s
u
p
p
o
r
t
i
n
g
t
h
e
s
y
s
t
e
m
PCN Advisor –
Dr Hina
Shahid:
hina.shahid1@nhs.net
PCN Advisor – Lianna Martin: lianna.martin@nhs.net
L
o
c
a
l
T
r
a
i
n
i
n
g
H
u
b
s
I
C
S
P
e
r
s
o
n
a
l
i
s
e
d
C
a
r
e
C
l
i
n
i
c
a
l
L
e
a
d
s
(
s
e
e
n
e
x
t
s
l
i
d
e
)
One for each of the ICS & Dr Jagan John as Pan London Lead
20
Support for PCNs...
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
•
A suite of co-produced support
•
Monthly share and learn ?any volunteers!
•
Case studies
•
Tailored 1:1 sessions – to answer any burning questions, explore challenges,
think through strategy to best use the roles, advice on peers to connect with
etc
•
Co-produced PCN toolkit & FAQ Guide
•
Your ideas?
21
Resources referenced...
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
KEY DOCUMENTS
•
NHS Long Term Plan available
here
.
•
PCN plans including IIF
•
IIF/ DES implementation guidance
•
DES Requirements and entitlements
•
The Health Creation Alliance:
How can PCNs suceed in reducing health inequalities
•
The Primary Care Network Handbook 21-22:
This handbook
has been created to give advice and options to practices looking to establish and develop a
primary care network (PCN). The “Workforce and employment” section provides in depth descriptions of all PCN roles.
FutureNHS
COLLABORATION PLATFORM
•
Please feel free to join the Personalised Care Collaborative Network
here
.
•
ARRS Primary Care Workspace
EXAMPLE PCN WORK PLAN
•
Health & Wellbeing Coaches and Care Coordinators Work Plan available
here
.
VIDEOS
•
Healthy London Partnership:
Library of Social Prescribing videos
•
Social prescribing: A GP’s perspective #NHSLongTermPlan –
Link Here
•
BMA:
Social prescribing & making it work for GPs and patients
•
UEL study:
Evaluation of social prescribing in City & Hackney
•
Value in Health Journal:
Combining Health and Outcomes Beyond
Health in Complex Evaluations of Complex Interventions: Suggestions
for Economic Evaluation
SPLWs, HWBCs & CCs MAILING LIST
•
In order to receive a monthly newsletter packed with events, guidance,
resources and interesting reads:
sign up here.
22
Social Prescribing: key resources
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
23
Supportive Self-Management: key resources
@
S
P
_
L
D
N
h
l
p
.
s
o
c
i
a
l
p
r
e
s
c
r
i
b
i
n
g
@
n
h
s
.
n
e
t
Vision for London includes expanding Social Prescribing to provide individualized care, tackling health inequalities, and promoting person-centered approaches to healthcare. Learn about the roles and benefits of implementing personalized care strategies in primary care networks in London.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
PERSONALISED CARE FOR LONDON Embedding the 3 personalised care ARRS roles @SP_LDN hlp.socialprescribing@nhs.net 1
Plan for today... TIME ITEM 12:35 Why is personalised care important? 12:40 Health inequalities & primary care 12:50 What are the 3 roles? 12:55 Benefits to PCN using 3 roles 1:05 Recruitment trends 1:20 Q&A 1:50 Shaping a way forward It is an informal session talk to each other & share resources in the chat The presentations will be recorded & circulated with slides @SP_LDN hlp.socialprescribing@nhs.net 2
PCN Advisors working 2 days a week until Apr 22 Purpose of the role: Supporting PCNS to successfully embed the three, personalised care roles (Social Prescribing Link Workers, Health & Wellbeing Coaches and Care Coordinators) to effectively tackle health inequalities and support primary care Build a network of those that employ or are working to embed the three personalised care roles in their work, facilitating a community of practice across London Dr Hina Shahid Lianna Martin Hina is a Portfolio GP in North West London and has a background in Public Health. She has worked in the VCSE sector for 15 years in community engagement, outreach and health inclusion, and health systems strengthening in the UK and internationally. She is an undergraduate tutor, GP Appraiser and also works in social research and health policy and has supported SPLWs in thinking through culturally appropriate practice With over 20 years experience in the VCSE and social enterprise sector, developing projects and partnership work, and previously at the Bromley by Bow Centre, Lianna is also a Regional Learning Coordinator for Social Prescribing and a Programme Manager at HLP in the Health Inequalities, Personalised Care team. Her time is dedicated to pan London initiatives supporting the development of social prescribing, enabling it to thrive @SP_LDN hlp.socialprescribing@nhs.net 3
Personalised care for London What it is: Vision for London: Personalised care means people have choice and control over the way their care is planned and delivered. It is based on what matters to them and their individual strengths and needs. Commitment to expanding Social Prescribing in all 5 ICS operating across the region Person centred care strives to see an individual as bio-psycho-social whole, as a person and not a disease or a collection of conditions. Core element of the London Vision and GLA s COVID recovery plan to be joined up working at a neighbourhood level, taking an asset-based approach and co- creating solutions Commitment in NHS Long Term Plan: Put in place more than 1,000 Social Prescribing link workers by the end of 2020/21, rising further by 2023/24, with the aim that more than 900,000 people are connected to wider community services that can help improve health and well-being. For London this means working towards 800 SPLWs operating by 23-24 = approx. 4 per PCN of average population of 50,000 @SP_LDN hlp.socialprescribing@nhs.net 4
Why is it important? 5 London boroughs in top 10% most deprived boroughs in UK PC role intrinsic tool for PCNs in community recovery Uses appropriate team according local population needs & ensure roles working together, embedded in PCNs and being used in the right way Impact these roles can have on patients, community & surgeries can be significant Significant ARRS underspend in London funding & support available to grow these teams Personalised care is one of the five major, practical changes to the NHS that will take place over the next five years, as set out the recently published Long Term Plan (Jan 2019). Universal Personalised Care was written into an implementation or action plan for the rolling out personalised care across England, to reach 2.5 million people by 2023/24 and then aim to double that again within a decade. @SP_LDN hlp.socialprescribing@nhs.net 5
Health inequalities, inequities and primary care Over 80% of health outcomes are socially determined Inequities: systematic, avoidable and unfair differences in mental or physical health between groups of people Health disparities are widening in the UK- highest in London COVID-19: vital community health function of general practice (RCGP) The exceptional potential of PCNs- anchor institutions Address and optimise individual and population health outcomes Drive engagement between primary care and communities Cross-sector working @SP_LDN hlp.socialprescribing@nhs.net 6
Key areas of health disparities @SP_LDN hlp.socialprescribing@nhs.net 7
Social determinants of health Cross-sector Multi agency Joined up care Partnership working Co-production of services and resources Outreach Empowerment Focus on individuals, communities and their environment Dahlgreen & Whitehead, 1991 @SP_LDN hlp.socialprescribing@nhs.net 8
Integrated care systems Part of LTP Fundamental shift in the way the health and care system is organised- move away from organisational competition and the separation of commissioners and providers to focus on collaboration and on places and local populations as the driving forces for improvement Central aim of ICSs is to integrate care across different organisations and settings, joining up hospital and community-based services, physical and mental health, and health and social care greater integration of health and care services improving population health and reducing inequalities supporting productivity and sustainability of services helping the NHS to support social and economic development Case for collaborative, cross sector partnership working strengthened by experiences of Covid-19 pandemic Statutory April 2022 Local contextualised arrangements- focus on local needs and resources and local leadership @SP_LDN hlp.socialprescribing@nhs.net 9
What the roles do... Social Prescribing Link Workers Health & Wellbeing Coaches Care Coordinators Address wider issues (social determinants of health) that impact people s health & wellbeing. Work with patients who will benefit from and provide: Work with patients who will benefit from, and provide: Support in navigating the health system and connecting with the right people Continuity of care a point of contact alongside busy clinicians Goal setting - Guide and support people with LTCs to set self-identified health and wellbeing goals Take time with patient, using personalised care support planning, motivational interviewing & health coaching approaches, over several sessions to identify what matters to the person and connect them with; Behaviour change - Use specialist coaching and behaviour change techniques, usually over a number of sessions Allyship and advocacy - post appointment follow-up conversations, support in understanding health conditions, creating space to reflect on choices right for individual ensuring changing needs are addressed practical, social and emotional support within their community activities that promote wellbeing e.g. arts, sports, natural environment. Tend to support with physical and mental health conditions, and with one or more LTCs such as type 2 diabetes, COPD, or those at risk of developing a LTC. Provide coordination and access to other appropriate services and support. Act as a bridge between primary care and the community - Identify and nurture community assets by working with partners such as VCSE, LA and NHS. Can be main point of contact for care homes Tend to support people experiencing loneliness, complex social needs, mental health needs or multiple LTCs. Tend to support those with multiple appointments, chronic conditions, frail/elderly and particularly vulnerable people often with LTCs. @SP_LDN 10 hlp.socialprescribing@nhs.net
Ensuring the personalised care roles work effectively together @SP_LDN hlp.socialprescribing@nhs.net 11
Referrals into the system First point of referral can be any of the three, this varies across services and depends on the presenting problem. For example, some services might use the SPLW as an initial gatekeeper for referrals to all three workers, whereas some PCNs might only have one of the roles in post so direct referral is necessary. Can refer to each other and good communication between 3 roles is essential. Social Prescribing Link Worker Service GPs Referrals Community Pro-active case identification Receptionist Care Health & Wellbeing Coach Pharmacist Coordinator @SP_LDN hlp.socialprescribing@nhs.net 12
Optimising individual and population health and wellbeing SPLWs Range of positive health outcomes, reduced isolation, inc. independence Rotherham: 80% improvement LTCs, 90% for mental health users Care coordinators LTCs and vulnerable/ excluded groups- deprivation, ethnic minority, disabilities, LGBTQ Case finding unmet needs Coordinating care across sectors, MDTs, recalls, screening, care planning, annual reviews Health and wellbeing coaches Health creation: control, contact, confidence (The Health Creation Alliance) Motivation and achieve health goals Preventing illness Empowering self supported management @SP_LDN hlp.socialprescribing@nhs.net 13
Supporting the clinical workforce ~ 20% GP time spent on non health matters higher in deprived areas 80% GPs report that dealing with non-health issues -> reduced time to treat patient s health issues Release non-medical GP appointments Ensure patients get appropriate support right place, right person, right time Addressing root causes reduces demand for services @SP_LDN hlp.socialprescribing@nhs.net 14
The positive impact... 2017 University of Westminster review average 28% reduction in demand for GP services 24% fall in A&E attendance for patients referred to a social prescribing scheme. fewer hospital admissions and A&E attendances fewer outpatient appointments fewer GP consultations reduced reliance on medical prescriptions effective in reducing demand on primary and secondary care. Hospital admissions A&E attendance Non-elective inpatient episodes GP consultations Reliance on prescriptions 2016 study in Rotherham non-elective inpatient episodes reduced by 75%, non-elective inpatient spells reduced by 11% A&E attendances reduced by 17%. Self-reported measures of health and wellbeing 2014 study from the University of East London and City and Hackney CCG 25% reduction in A&E attendance in their social prescribing group vs 66% increase in A&E attendance by the control group @SP_LDN hlp.socialprescribing@nhs.net 15
Evaluating cost effectiveness... Social Return on Investment (SROI) Conservative estimate 1: 3.52 Long term period 1: 5.77 For mental wellbeing 1: 8.56 QALY Meets NICE thresholds for cost- effectiveness in studies @SP_LDN hlp.socialprescribing@nhs.net 16
What is working... Give these roles TIME to spend with patients e.g. caseloads of 200 250 per year depending on complexity for SPLWs for example to build a meaningful bridge between primary care and the community, scope appropriate activities, influencing development etc. A one team approach for personalised care roles to proactively reach out to cohorts of patients experiencing health inequalities and most in need of this support to support and develop each role to connect with each other, access peer support and ongoing training and development to work together on shared goals and outcomes Embed these roles within PCN teams attending MDT meets will enable a holistic approach to supporting patients with complex needs manage and benefit from role interdependencies Ensure the three roles are working effectively together so they are being used to their greatest value combine traditional and place- based MDT models Ensure there is a robust plan in place, with induction & clear job roles Communicate to the wider referring workforce, the purpose of the roles and how they can benefit the work of the wider practice @SP_LDN hlp.socialprescribing@nhs.net 17
Examples of good practice in PCNs Understand and work to overcome barriers to access for vulnerable and excluded groups by working with community- based partners and embedding an asset based approach Shift to community-led community development and a strategy/ community development specialist to link PCNs and community partners Empowering communities to address wellbeing themselves through supported self management Supporting professional development and supervision of ARRS roles and considering team leader / complex case manager Service pathways co-produced with local partners to meet diverse needs- social, economic, material, cultural as well as medical Evaluate, reflect, learn, share and embed Open and transparent Clear values and purpose in a coherent system Diverse governance and leadership not just GPs Executive committee/clinical cabinet, buddying with other local PCNs Focus on partnership working, shared decision making Understand DES and use it to align with local needs and priorities incl. health disparities Intelligence driven population health management Health inequalities lead and/or personalised care champions Understands 3 PC roles with clear and consistent referral criteria Forward thinking and developing a one team approach Focused not just on outcomes but also experience Multi agency, place based MDTs @SP_LDN hlp.socialprescribing@nhs.net 18
Support available in London HLP Personalised Care Team Supporting the London system to spread and scale personalised care Convening multisector partnership work to support, develop and innovate social prescribing NHSE Associate roles supporting frontline staff Regional Learning Coordinator for Social Prescribing Lianna Martin: lianna.martin@nhs.net Health and Wellbeing Coach Mentor Caroline Haines: caroline.haines1@nhs.net Care Coordinator Mentor Ali Hassas: alihassas@nhs.net NHSE Associate roles supporting the system PCN Advisor Dr Hina Shahid: hina.shahid1@nhs.net PCN Advisor Lianna Martin: lianna.martin@nhs.net Local Training Hubs ICS Personalised Care Clinical Leads (see next slide) One for each of the ICS & Dr Jagan John as Pan London Lead @SP_LDN hlp.socialprescribing@nhs.net 19
Support for PCNs... A suite of co-produced support Monthly share and learn ?any volunteers! Case studies Tailored 1:1 sessions to answer any burning questions, explore challenges, think through strategy to best use the roles, advice on peers to connect with etc Co-produced PCN toolkit & FAQ Guide Your ideas? @SP_LDN hlp.socialprescribing@nhs.net 20
Resources referenced... KEY DOCUMENTS NHS Long Term Plan available here. PCN plans including IIF IIF/ DES implementation guidance DES Requirements and entitlements The Health Creation Alliance: How can PCNs suceed in reducing health inequalities The Primary Care Network Handbook 21-22: This handbook has been created to give advice and options to practices looking to establish and develop a primary care network (PCN). The Workforce and employment section provides in depth descriptions of all PCN roles. BMA: Social prescribing & making it work for GPs and patients UEL study: Evaluation of social prescribing in City & Hackney Value in Health Journal: Combining Health and Outcomes Beyond Health in Complex Evaluations of Complex Interventions: Suggestions for Economic Evaluation FutureNHS COLLABORATION PLATFORM Please feel free to join the Personalised Care Collaborative Network here. ARRS Primary Care Workspace SPLWs, HWBCs & CCs MAILING LIST In order to receive a monthly newsletter packed with events, guidance, resources and interesting reads: sign up here. EXAMPLE PCN WORK PLAN Health & Wellbeing Coaches and Care Coordinators Work Plan available here. VIDEOS Healthy London Partnership: Library of Social Prescribing videos Social prescribing: A GP s perspective #NHSLongTermPlan Link Here @SP_LDN hlp.socialprescribing@nhs.net 21
Social Prescribing: key resources 1. Summary Guide, which gives a clear picture of what a good social prescribing scheme looks like for everyone - also includes a common outcomes framework to help measure the impact of social prescribing on people, the local system, and the voluntary and community sector. 2. Reference Guide for PCNs supports PCNs with information on setting up social prescribing services including support for recruitment, induction and supervision - also outlines quality assurance measures, and how info can be gathered to help develop a consistent evidence base for social prescribing. 3. Welcome and induction pack for link workers in primary care networks (PCNs). 4. Handout for practice staff to give to people who are referred to a social prescribing link worker. 5. Themed fortnightly webinars for link workers 6. Regional Learning coordinators (London = lianna.martin@nhs.net) provide learning and peer support for link workers (SPLWs) at both a regional and Primary Care Network (PCN) level 7. Regional Facilitators support local system leaders to bring partners together to create and deliver place-based plans across the ICS/STP footprint which support the development of social prescribing and community-based approaches and to embed link workers in every Primary Care Network . 8. Regional PCN Advisors - support PCNs to embed the three personalised care roles within primary care: Social Prescribing Link Workers (SPLWs), Health and Wellbeing Coaches (HWbCs) and Care Coordinators (CCs) (London = lianna.mrtin@nhs.net + hina.shahid1@nhs.net) 9. Accredited online training through Health Education England 10. Personalised Care Institute - Free courses available through the Personalised Care Institute. Core skills training shared decision making and personalised care and support planning training that is available free online from the PCI would be, on the whole, relevant and of benefit to the personalised care roles. 11. Social Prescribing Slide deck Generic slide deck for social prescribing presentations 12. Directed Enhanced Service sets out how commissioners must offer to primary medical services contractors the opportunity to participate in the Network Contract Directed Enhanced Service (DES). It outlines the eligibility requirements and process for primary medical services contractors to participate; and sets out the relevant rights and obligations for PCNs and commissioners. 13. Network Contract DES VAT Information This document is an information note from NHS England regarding the Network Contract DES and VAT 14. IIF Implementation Guidance 2021-22 This document sets out guidance for primary care networks (PCNs) implementing the Investment and Impact Fund, as per the requirements set out in the 2021/22 Network Contract Directed Enhanced Service (DES) Specification. 15. Key DES-IIF and operating changes 2021-22 16. FutureNHS Collaboration Platform Source of good practice guidance, webinars, updates and more. Something we should be encouraging link workers to join. To join please email: england.socialprescribing@nhs.net @SP_LDN hlp.socialprescribing@nhs.net 22
Supportive Self-Management: key resources 1. Measurement and evaluation within supported self-management This guide describes the steps for planning hot to use measurement within supported self-management, based on evidence and good practice. 2. Health & Wellbeing Coach Welcome pack - The welcome pack is designed for newly appointed health and wellbeing coaches in primary care networks. 3. Care Coordinator workers Welcome pack - The welcome pack is designed for newly appointed care coordinators in primary care networks. 4. Health Coaching guide and technical annex Designed to support the delivery of health coaching. This guide should be used when commission and when deciding what can or should be counted and reported as health coaching in a local area. 5. Care Coordinator recruitment pack An optional resource to provide support to PCN s in the recruitment or engagement of care coordinators. The resource includes: Sample job description Sample person specification Sample job advert Sample interview questions 6. Health & Wellbeing Coach recruitment pack An optional resource to provide support to PCN s in the recruitment or engagement of care coordinators. The resource includes: Sample job description Sample person specification Sample job advert Sample interview questions 7. Care Co-ordination practice leaflet - Primary Care practice leaflet to explain the role of Care Coordinators to patients 8. Health and Wellbeing FAQ s 9. Care Coordination- Primary Care leaflet - This document provides an in-depth summary of the roles and application of the Care Coordinator within primary care. 10. Health & Wellbeing Coach Mentor: Caroline Haines, caroline.haines1@nhs.net 11. Care Coordinator Mentor: Dr Ali Hassas, alihassas@nhs.net 12. FutureNHS Collaboration Platform - Source of good practice guidance, webinars, updates and more. Something we should be encouraging link workers to join. To join please email: england.supportedselfmangement@nhs.net @SP_LDN hlp.socialprescribing@nhs.net 23