ENT In-Service Review by Dr. Quinton Gopen, M.D. - UCLA Medical School
Detailed in-service review by Dr. Quinton Gopen from UCLA Medical School covering various ENT topics such as trauma management, hearing loss, and Meniere's disease. Includes sample questions, answers, and explanations. Helpful insights for medical students and professionals.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
In-Service Review Quinton Gopen, M.D. U.C.L.A. Medical School Division of Otolaryngology Feb 29th, 2012
General points Exam setup Little to no time pressure Only half of the questions are scored Different versions of same question are test questions Many questions ambiguous and difficult to interpret If everyone get them right, they are thrown out If everyone get them wrong , they are thrown out Don t fall for traps Question seems too straight forward, probably is! What is clinically done not always right answer
Question 1 24y.o. male is involved in a motor vehicle accident. Patient has left bloody otorrhea and complains of hearing loss. Patient has obvious facial fractures. What is the first imaging test you should order? A. MRI scan brain and internal auditory canals B. CT scan of the temporal bones C. AP and lateral neck films D. Chest X-ray E. CT scan facial bones
Question 1 Answer C. AP and lateral neck films Explanation: clearing the C-spine is an important first step in trauma management.
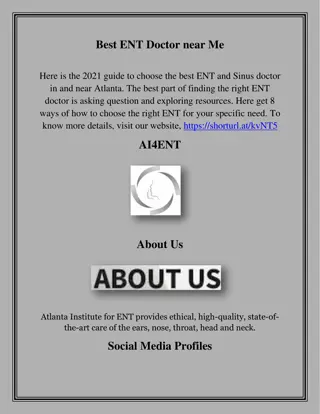
Question 2 46 year old woman complains of hearing loss in both ears. Weber test localizes to the right ear and bone conduction greater than air conduction on right side. Otoscopy normal, no history of ear infections. What is the best management? A. Observation B. Left stapedotomy C. Right stapedotomy D. CROS hearing aid E. Bi-CROS hearing aid FREQUENCY IN HERTZ (Hz) HEARING LEVEL (HL) IN DECIBELS (dB) X XX X X X X WRS RT76% WRS LT 26%
Question 2 Answer E Bi-Cros hearing aid YOU CAN NEVER OPERATE ON THE BETTER HEARING EAR!!!! * *UNLESS THERE IS A DESTRUCTIVE PROCESS WHICH WILL INJUR THE EAR FURTHER WITHOUT SURGERY Cholesteatoma Mastoiditis
Question 3 A 33 y.o. man has bilateral Meniere s disease. He has undergone a left labyrinthectomy. ENG shows no left sided vestibular function and 50% reduced right sided vestibular function. Persistent frequent disabling vertigo attacks. Management? A. left intratympanic gentamicin B. Right intratympanic gentamicin C. Left vestibular nerve section D. Right vestibular nerve section E. Right endolymphatic sac decompression
Question 3 Answer: Choice E Right endolymphatic sac decompression This is an example of the default choice. All other choices can be eliminated, and tough sac decompression is controversial, it is the only answer that is not contra-indicated
Question 4 An 8 y.o. girl has profound bilateral deafness. She presents with a syncopal episode while playing at school. Her parents are interested in pursuing a cochlear implant. What should your work up include? A. An EKG B. A CT scan of the temporal bones C. A MRI of the brain and internal auditory canals D. A promontory stimulation test E. An ABR test
Question 4 Answer: A An EKG This patient has Jervel-Lange-Nielson syndrome. Profound deafness and prolonged Q-T interval places them at significant risk for sudden death, particularly with exercise or surgical procedures. Critical to identify. This is an example of many appropriate choices, but one is more correct than the others.
Question 5 What is the most likely place of recurrent cholesteatoma? A. Eustachian tube B. Anterior epitympanic space C. Angle of Citelli D. Sinus tympani E. Retrofacial air cells
Question 5 Answer: D Sinus tympani A classic question. Sinus tympani cannot be seen directly as the facial nerve lies on top of this space. It cannot be opened from the mastoid side as the labyrinth blocks the approach Extra credit. The subiculum is the inferior boundary of the sinus tympani, and the ponticulus is the superior boundary of the sinus tympani
Question 6 A 17y.o. man has a large left acoustic neuroma. Postoperatively he has complete facial paralysis. He has waited 14 months and has no return of volitional movement of his face. What is his best rehabilitative option? A. Revision left retrosigmoid approach with cable graft B. XII-VII left nerve crossover graft C. Left brow lift D. Botox injection to the right face E. Botox injectin to the left face
Question 6 Answer B XII-VII crossover graft Although a cable graft sounds good, the facial nerve is almost always intact after acoustic neuroma resection. If the nerve was torn, a cable graft should be done at the time of surgery. Since no mention of this, assume the proximal part of the nerve is not viable. XII-VII better than static reanimation.
Question 7 A 14 y.o. boy falls down a hill into a tree branch that punctures his right eardrum. He is brought into the ER and is vertiginous with nausea and vomiting. He complains of right hearing loss. What is the best treatment. A. IV dexamethasone 10mg B. CT scan of the temporal bones C. Middle ear exploration D. Scopolamine patch E. IV rehydration
Question 7 Answer: C Middle ear exploration The vertigo is of concern. May be a subluxed stapes or worse, a foreign body of wood in the vestibule. Urgent surgery to seal the inner ear and remove and foreign material is crucial. The other choices are all reasonable, but exploring the ear is the best answer.
Question 8 Which of the following is the best candidate for cochlear implantation? A. A child with Mondini malformation B. A child with a small IAC on CT scan C. An adult patient who was born profoundly deaf D. A child with Michel s malformation E. An adult with neurofibromatosis type II s/p bilateral acoustic neuroma resections.
Question 8 Answer: A Mondini malformation The key issue for cochlear implantation is a viable cochlear nerve. All the other choices, the nerve is either not present or not viable. Mondin malformations have an increased risk of spinal fluid leaks but otherwise do reasonably well with cochlear implantation
Question 9 A 47 y.o. woman undergoes a glomus jugular resection. After obtaining distal and proximal control of the sigmoid sinus and jugular vein, profuse bleeding occurs during resection of the tumor. What is the most likely source? A. Transverse sinus B. Straight sinus C. Superior petrosal sinus D. Inferior petrosal sinus E. Confluence of the sinuses
Question 9 Answer: D. Inferior petrosal sinus This sinus plugs into the jugular bulb from its medial aspect and is a common source of bleeding. Packing must be limited as over packing results in lower cranial dysfunction from compression injury.
Question 10 Which is the best hearing test for an 18 month old baby girl? A. Conventional audiometry B. VEMP testing C. Conditioned play audiometry D. Dichotic testing E. Visual reinforcement audiometry
Question 10 Answer: E - Visual reinforcement audiometry This is the most appropriate test for this age. Conditioned play audiometry is more for 2- 3years old. Dichotic testing is for central processing disorders, usually not testable unitl around 8y.o.
Question 11 What runs within the cochlear aqueduct? A. Endolymhatic duct B. Ductus Reuniens C. Perotic duct D. Endolymphatic sac E. Helicotrema
Question 11 Answer: C Perotic duct The perotic duct is analagous to the endolymphatic duct within the vestibular aqueduct. The perotic duct is comprised of loose connective tissue and contains CSF as it turns into perilmph within the inner ear. The cochlear aqueduct runs from the posterior cranial fossa to the basal turn of the cochlea inferior to the internal auditory canal
Question 12 Which of the following is a false statement about a patulous Eustachian tube? A. It causes autophony B. It improves with exercise C. It improves with lying supine D. It is associated with extreme weight loss E. It is associated with rheumatologic cases
Question 12 Answer B - It improves with exercise. This is false, the condition worsens with exercise as the exercise causes vasoconstriction of the mucus membranes in the nose to increase airflow through the nose during exercise. This causes the condition to get worse.
Question 13 This condition is: A. Autosomal recessive B. Is associated with retinitis pigmentosum C. X-linked D. Is associated with thyroid dysfunction E. Results from a defect in neural crest development
Question 13 E. Results from a defect in neural crest development Pendred s Usher s Jervel Lange Nielson Alport s thyroid dysfunction retinitis pigmentosum (blindness) cardiac (prolonged QT) kidney dysfunction
Question 14 A patients presents with right hearing loss. A 30dB pure tone at 1k Hz is presented to the right ear at the same time a 15dB pure tone at 1k Hz is presented to the left ear. The patient does not hear any sound. What is your diagnosis? A. Pseudohypoacusis B. Right mild sensorineural hearing loss C. Right conductive hearing loss D. Central hearing loss E. Right profound sensorineural hearing loss
Question 14 Answer: A Pseudohypoacusis (also known as malingering). This is an example of the Stenger s test. Same tone to both ears, the louder side is the only side a normal patient will hear. The malingerer only hears the sound on the ear that they are lying about the hearing, so they claim to hear nothing. Pt with true hearing loss hears the sound in the only hearing ear.
Question 15 A patient has a lesion within the petrous apex that is hypointense on T1 and hyperintense on T2 imaging. It does not enhance with Gadolinium. What is the most likely pathology? A. Asymmetric bone marrow B. Vestibular schwannoma C. Cholesterol granuloma D. Cholesteatoma E. meningioma
Question 15 Answer: D Cholesteatoma Although variable, cholesteatoma is usually bright on T2 and does not enhance with gadolinium. It is bright on diffusion weighted images. Cholesterol granuloma is bright on T1/T2 images, bone marrow on T1 and tumors enhance with gadolinium.
Question 16 What is the most common complication of cochlear implant surgery? A. Facial paralysis B. Malpositioned device C. Meningitis D. Spinal fluid leak E. Device exposure
Question 16 Answer E Device extrusion. These are all complications of cochlear implantation, but flap necrosis with device extrusion is the most common complication I believe.
Question 17 A 57 y.o. man has a 4mm enhancing mass in the fundus of the left internal auditory canal. There is a moderate left sensorineural hearing loss with a discrimination score of 62%. What is the best approach to this tumor? A. Middle fossa craniotomy B. Translabyrinthine craniotomy C. Transotic craniotomy D. Retrosigmoid craniotomy E. Infracochlear approach
Question 17 Answer: A Middle fossa craniotomy Although controversial, the correct answer is middle fossa for small tumors in the fundus of the IAC. The fundus is the lateral most part of the IAC, whereas the porus is the more medial part of the IAC. A translabyrinthine approach is good for any sized tumor, huge to tiny, but does not preserve hearing.