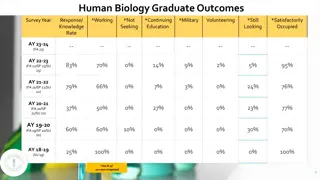
Comprehensive Primary Care Guidelines for NICU Graduates
 undefined
undefined







KAREN HUSSEIN, PGY-3
Primary Care of the
Preterm Infant








Goals and Objectives
Identify, understand and manage the ongoing
medical needs of the NICU graduate
Recognize the key role of the PCP in providing
optimal continuity of treatment by coordinating
transition of care from the neonatologist, providing
direct medical care and facilitating ongoing care of
the infant by subspecialists and other health
professionals
Review of common screening topics and medical
problems of the NICU graduate
Screening
Question #1
A premature infant presents to your office for an
initial visit after hospitalization.
What questions should be asked and topics should
be covered in the initial hospital follow up visit then
subsequent visits?
Initial Visit
NICU course
Current medications
Medical equipment
Home oxygen
Pulse oximetry
Apnea and bradycardia monitor
Ventilator
Feeding pump
Growth parameters
Current weight, length and head circumference as compared to at birth parameters
Vital signs
Nutrition
Formula and kcal/oz
Type of feeding (oral versus G-tube)
Volume and frequency of feeds
Immunization record
Neonatal screening
Metabolic and newborn screening
Cranial imaging
Hearing
Ophthalmologic
Specific problems related to infant
Review of NICU discharge summary
Initial Visit
Evaluation of progress since discharge including
growth
Time to listen and address the family’s concerns
Education for family about
Medical diagnoses
Cardiopulmonary resuscitation
Any medications and/or equipment required in care
Review future appointments with subspecialty
services , primary care visits and hearing and vision
screening
Subsequent Visits
Timing depends on infant’s medical condition
More frequent in the beginning to monitor and establish
adequate growth
Focus on:
Routine primary care (ie, immunizations)
General care directed towards NICU graduate (ie, hearing,
vision and development screening)
Specific medical problems of the infant
Consistent care that provides continuity of
information and psychosocial support to family
PREP Question #1
A 24-week-premature infant who is now 46 weeks of corrected gestational
age is being seen in your office for concerns of decreasing oral intake and
poor weight gain. The infant was discharged to home from the neonatal
intensive care unit 2 weeks ago weighing 2,400 grams. His medical
problems include bronchopulmonary dysplasia that requires diuretics and
gastroesophageal reflux that has been treated with omeprazole. The infant
was sent home feeding a minimum of 45 mL of premature formula
concentrated to 27 calories per ounce orally every 3 hours using a slow flow
nipple. At the first office visit 1 week ago, the infant weighed 2,505 grams
and was described as feeding slowly but taking the minimum volume of
formula daily. Currently, the infant weighs 2,610 g. The mother reports that
the infant is feeding 35 to 45 mL of formula every 3 hours. The mother
describes her son as waking and hungry every 3 hours, although he often
“shuts down” after 10 minutes of feeding and refuses to take more. The
infant does not spit, arch, or turn red with feedings. He passes 2 soft,
brown stools daily. The physical examination is otherwise unremarkable.
When you observe a feeding, the infant has unlabored respiratory effort
and maintains an oxygen saturation of 95%.
PREP Question #1
Of the following, the MOST appropriate approach to
help with the poor oral intake is to
A. advance the caloric content of the formula
B. change to a regular-flow nipple
C. consult occupational therapy
D. increase the diuretic dosage
E. initiate oxygen via nasal cannula
Answer
C. consult occupational therapy
Consultation with an occupational therapist
experienced with premature infants is recommended
when feeding problems are identified in discharged
premature infants.
Feeding problems are 7 times more common in
infants born prematurely, with 33% of infants born
at less than 26 weeks’ gestation having continued
feeding issues at 30 months’ corrected gestational
age.
Growth
At risk for inadequate growth due to increased caloric and
nutrient requirements and feeding skills
Swallowing problems
Oral motor dysfunction
Hypersensitivity
Delayed feeding skill development
Oral aversion problems
Plot growth curves and developmental milestones according
to corrected age for the first two years of life
Initiate corrective measures
Changes in the composition, volume, caloric density and mode of feeding
Evaluate for contributing conditions (ie, gastroesophageal
reflux or feeding disorders)
Prompt referral to a feeding specialist and/or nutritionist
Immunization
At increased risk for vaccine-preventable infections
AAP recommends that medically stable preterm
infants should receive full immunization based upon
their
chronological age
consistent with the
schedule and dose recommended for full-term
infants
May have been started in the NICU but delays are
common, especially in unstable infants, so it is
important to obtain an immunization record
Consider RSV prophylaxis with Palivizumab
Please see dedicated CCC presentation for more details
PREP Question #2
A 2-year-old boy who has a history of premature
birth has been diagnosed with hearing loss. He was
born at 28 weeks’ gestation and required 2 weeks of
mechanical ventilation. After discharge, he required
home oxygen therapy for 3 months. His mother asks
if any medications could have contributed to his
hearing loss.
PREP Question #2
Of the following, the medication exposure MOST
likely to contribute to hearing loss is
A. amphotericin B
B. caffeine
C. cefotaxime
D. chlorothiazide
E. furosemide
Answer
E. furosemide
The AAP Joint Committee on Infant Hearing Year 2007 position
statement has identified risk factors for children with congenital or
acquired hearing loss that include
Neonatal Intensive Care Unit (NICU) hospitalization greater than 5 days,
Extracorporeal membrane oxygenation (ECMO)
Mechanical ventilation
Hyperbilirubinemia requiring exchange transfusion
Exposure to ototoxic medications, such as aminoglycosides (gentamicin and
tobramycin) or loop diuretics (eg, furosemide)
Furosemide-induced ototoxicity can be either transient or
permanent.
Aminoglycosides appear to potentiate the ototoxic effects of
furosemide and, as such, it is recommended that efforts be made to
avoid simultaneous use of aminoglycoside and loop diuretics.
Hearing
Estimated prevalence of bilateral sensorineural
hearing loss is 1-2 per 1000 newborns in the US, but
is 10-20 times higher among premature infants
Recommended to have automated auditory
brainstem response as screening test for hearing
Follow up audiological evaluation during the first
year of life or sooner if needed is critical to ensure
the timely diagnosis on late-onset hearing loss
Infants with other risk factors, such as meningitis or
cytomegalovirus, should have follow up testing
performed soon after discharge
Vision
At increased risk for long-term ophthalmologic
abnormalities including
Retinopathy of prematurity (ROP)
Strabismus
Reduced visual acuity
Myopia
Amblyopia
Anisometropia
Retinal detachment
Neurodevelopment
At increased risk for developmental delays and disabilities
Motor impairment and/or tone abnormalities
Cerebral palsy
Learning delay or disability
Borderline low-average intelligence quotients (IQs)
Autism or autism spectrum disorders
Attention-deficit hyperactivity disorder (ADHD)
Specific neuropsychological deficits (ie, visual motor integration,
executive dysfunction)
Behavior problems (ie, internalizing problems, social difficulties)
Risk is increased with decreasing gestational age
Need to identify and refer at-risk infants for further
evaluation and early intervention services
Follow up with family to ensure infant is receiving appropriate
services specific to developmental needs (PT, OT, ST for
feeding, Early Steps)
Psychosocial Issues
Bringing home a NICU graduate can be very
challenging to parents because of social, financial
and psychological stresses
Siblings and spouses may feel neglected by the
infant’s needs
Need to screen for these stressors
Provide support services
Home health nursing visits
Early child intervention services
Support groups
Social work services
Child protective services
Car Seats and Beds
To prevent morbidity and mortality caused by motor
vehicle accidents
Premature infants can be at increase risk for
cardiopulmonary compromise while in car seats
Greater decreases in oxygen saturation
More frequent episodes of desaturation, bradycardia and
apnea
Greatest risk with infants with pre-discharge weights < 2000g
Need car seat challenge prior to discharge if at risk
Please see dedicated CCC presentation for more
details
Dental
Increased risk of dental problems
Enamel hypoplasia
Increased risk for dental carries
Delayed tooth eruption
Based upon adjusted postmenstrual age between 3-10 months
Tooth discoloration
Palatal groove
Tooth malalignment
If prolonged intubation, may develop V-shaped palate, posterior
cross bites, deformed incisal edges and missing teeth
Recommend first visit by 12 months of age
Fluoride exposure via water recommended after 6
months of age
Common Problems of the
NICU Graduate
PREP Question #3
A mother brings her 7-week-old infant in for his first
health supervision visit after being discharged from
the neonatal intensive care unit. The infant was
delivered at 31 weeks’ gestation because of placental
abruption. He was intubated for 4 days after delivery
and received 3 doses of surfactant for respiratory
distress syndrome. He subsequently required oxygen
by high flow nasal cannulae for 1 week. He has been
in room air since that time and results of his chest
radiograph are normal. His mother is worried that
her infant has moderate to severe chronic lung
disease.
PREP Question #3
Of the following, the MOST appropriate information
to provide to the mother is that infants who have
chronic lung disease
A. are born at less than or equal to 26 weeks’ gestation
B. have chest radiographs with severe fibrosis and
hyperventilation
C. have received a minimum of 5 days of assisted ventilation
D. maintain normal postnatal lung development
E. require supplemental oxygen at 36 weeks’ corrected
gestation
Answer
E. require supplemental oxygen at 36 weeks’
corrected gestation
The most commonly used definition of the “new BPD,”
currently referred to as chronic lung disease (CLD), is the
requirement of oxygen at 36 weeks’ corrected gestation.
With the improvement in ventilator management and the
incorporation of therapeutic modalities such as prenatal
corticosteroids and surfactants into daily practice, the
underlying mechanism for CLD is believed to be an arrest
of normal lung development due to premature birth.
The radiographs of CLD often do not reveal the fibrosis
and hyperinflation that was characteristic of infants
diagnosed with BPD in the past.
Respiratory
Most common problem is bronchopulmonary dysplasia (BPD) or
chronic lung disease (CLD) of prematurity
Respiratory disease with requirement of supplemental oxygen at 36 weeks
postmenstrual age and persistent abnormalities on chest radiographs
At discharge, baseline studies include respiratory and heart rate, blood pressure,
oxygen requirement, chest radiograph and echocardiogram to assess for presence
of pulmonary hypertension
May continue to require supplemental oxygen, medications (ie, diuretics,
electrolyte supplements and bronchodilators) and increased caloric needs
Most often allowed to outgrow diuretic dose and slow wean of home oxygen
Morbidities include acute respiratory exacerbations, pulmonary edema, upper
and lower respiratory tract infections, cardiac problems (ie, cor pulmonale and
pulmonary hypertension) and growth failure
Typically improves by two years of age
At risk for reactive airway disease and respiratory infections (ie,
RSV and other virus or bacterial infections)
Be alert for late-onset sequelae of prolonged intubation (subglottic
stenosis)
Apnea of Prematurity
Approximately in 25% of premature infants
Most outgrow by postmenstrual age of 40 weeks
Some will continue to have apnea and may be
discharge home on methylxanthine therapy (ie,
caffeine) or apnea monitors
Timing to discontinue these interventions is
multifactorial, usually determined by the
subspecialist or NICU follow up clinic
Question #2
What is the second most common cause of childhood
blindness?
Retinopathy of Prematurity
Second most common cause of childhood blindness
Treatment can reduce morbidity
Indicated in all infants with birth weight < 1500 g or
gestational age less than 31 weeks
Also indicated in infants whose clinical course places them at
increased risk as determined by the neonatologist
Typically presents at approximately 32 weeks gestation
Peaks at 38 to 40 weeks
Beings to regress by 46 weeks
Initial retinal screening 4-6 weeks after birth
Additional examinations at intervals of 1-3 weeks until retinal
vessels have fully matured
PREP Question #4
You are the primary care physician for newborn
twins born at 33 weeks’ gestation and discharged
from the neonatal intensive care unit after a 4-week
stay. They required oxygen for 3 days after birth, but
little other respiratory support. They were diagnosed
with gastroesophageal reflux disease. They have
occasional episodes of coughing and gagging without
color change. They are otherwise well.
PREP Question #4
Of the following, the BEST advice to give the parents
is to place the twins in
A. prone sleep position
B. side sleep position
C. sitting devices, such as car seats, during sleep
D. sleep positioners to keep their heads elevated
E. supine sleep position
Answer
E. supine sleep position
Except in a very few instances, supine is the safest sleep
position for an infant including those with
gastroesophageal reflux.
The safest place for an infant to sleep is on a firm, well-
fitted mattress in an approved crib, bassinet, or play yard
free of other objects and located in the parents’ room.
Current American Academy of Pediatrics
recommendations extend beyond “Back to Sleep” to
address other sleep environment factors.
Bed sharing, while controversial, is not recommended,
and even twins should sleep on separate sleep surfaces.
Sudden Infant Death Syndrome (SIDS)
Death of an infant less than one year of age that
remains unexplained despite a thorough
investigation
At greater risk than term infants with a peak risk at
50-52 weeks postmenstrual age
No evidence that home apnea monitors decrease the
risk
Screen at each visit to ensure families are following
AAP recommendations of supine (back) sleeping
position and ask about location of sleeping
Gastroesophageal Reflux
Common in premature infants and in those with CLD,
neurological impairment or congenital defects (ie,
tracheoesophageal fistulas or diaphragmatic hernias)
Monitor for complications including
Poor weight gain due to decreased caloric intake
Apnea and bradycardia
Aspiration
Choking
Esophagitis
Laryngospasms
Discomfort
Nectrotizing Enterocolitis
Complications
Need for ostomy care
Malabsorption
Intestinal dysmotility
Need for parenteral nutrition despite enteral feedings
Cholestasis
Infections of the ascending biliary tract
Biliary calculi
Late partial or complete bowel obstruction
Short bowel syndrome
Dumping syndrome
Growth failure
Fluid imbalance and electrolyte abnormalities
Need for follow up with pediatric surgery and/or
gastroenterologist
PREP Question #5
A 6-week-old male infant is brought to your office for a routine visit. He
was born at 29 weeks’ gestational age with a birth weight of 1,250 grams to
an 18-year-old mother who did not receive prenatal care until the third
trimester. The baby’s blood type is O positive and his mother’s is B positive.
He had neonatal hyperbilirubinemia and received phototherapy for 1 week.
He is tolerating his feeds of 22-kcal/oz formula and his weight is now 2,265
grams. His temperature is 37.0°C, his pulse rate is 130/min, respiratory
rate is 30 breaths/min, and blood pressure is 80/55 mm Hg. He is alert and
in no apparent distress. His sclerae are anicteric, his oral mucosa is pink
and moist, his lungs are clear to auscultation, and there is no cardiac
murmur or hepatosplenomegaly. The mother is concerned that he looks
pale. The following are the results of his complete blood cell count:
White blood cell count, 12,500/μL (12.5 × 10
9
/L)
Hemoglobin, 8.5 g/dL (85 g/dL)
Mean corpuscular volume, 99 μm
3
(99 fL)
Platelet count, 389 × 10
3
/μL (389 × 10
9
/L)
Indirect (unconjugated) bilirubin, 1.0 mg/dL (17.1 μmol/L)
PREP Question #5
Of the following, the MOST appropriate assessment
of this patient would be that he has a
A. macrocytic anemia due to folate deficiency
B. microcytic anemia due to iron deficiency
C. normal hemoglobin for a preterm infant
D. normocytic anemia due to ABO incompatibility
E. normocytic anemia due to chronic inflammation
Answer
C. normal hemoglobin for a preterm infant
Normal hemoglobin concentration (Hb) and mean corpuscular
volume (MCV) vary with age, highest in the neonate and decline
significantly by 1 year of age.
During the first week after birth, hemoglobin production decreases
by a factor of 10 because of a sudden increase in tissue oxygenation,
causing a marked decrease of plasma erythropoietin.
This leads to a decrease in Hb known as the physiological anemia of
infancy, which occurs at around 6 to 8 weeks of age in full-term
infants.
In healthy preterm infants, this nadir can be exaggerated and is
known as the physiologic anemia of prematurity.
Although the term
anemia
is used, the decrease in hemoglobin is
normal and expected; therefore, physiological anemia of infancy is
not a true disease state.
Anemia of Prematurity
At risk for anemia that occurs earlier and is more
severe than physiologic anemia in term infants
Nadir for hemoglobin is 7-10 g/dL at 4-8 weeks
compared with 11 g/dL at 8-12 weeks in term infants
Treatment with iron supplementation (2 mg/kg/day
or in multivitamin) results in lower rate of iron
deficiency and iron deficiency anemia
Less additional supplementation needed if receiving
iron-fortified formula versus exclusively
breastfeeding
Symptomatic infants need red blood cell transfusion
Neurologic
Intraventricular hemorrhage (IVH), grades I-IV
Posthemorrhagic hydrocephalus occurs in 35% of infants with
IVH and risk increases with severity (ie, grades III and IV)
Early or late-onset
Obstructive, communicating or both
Transient or sustained
Slow or rapid progression
Shunt placement may be required with need for monitoring for
malfunction or infection
Postmeningitic hydrocephalus
Periventricular leukomalacia
Ischemic infarction of the white matter, most commonly adjacent to
lateral ventricle
Seizures
Common etiologies: hypoxic-ischemic injury, direct cerebral trauma,
intracranial hemorrhage, metabolic abnormalities, malformations and
infections
PREP Question #6
An infant develops abdominal distention and bilious
vomiting at 36 hours after birth. The 3.9-kg infant was
born at 37 weeks of gestation to a mother with type 1
diabetes mellitus. The prenatal course was
unremarkable, with negative carrier testing for cystic
fibrosis. According to the mother, the infant has been
breastfeeding and has had 4 wet diapers and 1 small
smear of meconium. Examination reveals an
uncomfortable infant with a distended, firm abdomen
that is slightly tender to deep palpation. The rectum
appears to be externally patent with an anal wink. A
radiograph is obtained.
PREP Question #6
PREP Question #6
Of the following, the MOST likely cause of the
infant’s findings is
A. anorectal malformation
B. Hirschsprung disease
C. meconium ileus
D. neonatal small left colon syndrome
E. pneumatosis coli
Answer
D. neonatal small left colon syndrome
An infant of a diabetic mother is at risk for
hypoglycemia, hypocalcemia, polycythemia and
neonatal small left colon syndrome.
Question #3
What are some of the common surgical procedures
performed on infants in the NICU?
Common Surgical Procedures
Surgical bowel resection secondary to necrotizing
enterocolitis (NEC) and/or intestinal perforation
Gastrostomy tube placement
Fundoplication
Ventriculo-peritoneal shunts
Tracheostomy
Cardiac surgeries
Umbilical hernia repair due to incarceration
Inguinal hernia repair
Discuss care for surgical areas and follow up with
surgical specialties
References
Committee on Fetus and Newborn (2008). Policy statement:
Hospital discharge of the high-risk neonate.
Pediatrics,
122(5)
, 1119-1126.
Stewart, J. (2014).
Care of the neonatal intensive care unit
graduate
. Retrieved from http://www.uptodate.com.
Woods, S. & Riley, P. (2006). A role for community health
care providers in neonatal follow-up.
Paediatr Child Health;
11(5)
, 301-302.
Andrews, B., Pellertie, M., Myers, P. & Hagerman, J. (2014).
NICU follow-up: Medical and developmental management
age 0 to 3 years.
Neoreviews, 15(4)
, e123-e132.
Sherman, M.P. (2013).
Follow-up of the NICU patient
.
Retrieved from http://emedicine.medscape.com/.
AAP PREP Questions
This guide outlines the essential aspects of primary care for preterm infants discharged from the NICU. It covers key topics such as initial visit assessments, follow-up visits, screening protocols, and ongoing management strategies. Emphasis is placed on continuity of care, monitoring growth, addressing family concerns, and collaborating with subspecialists for optimal outcomes.

Uploaded on Oct 01, 2024 | 0 Views
Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Primary Care of the Preterm Infant KAREN HUSSEIN, PGY-3
Goals and Objectives Identify, understand and manage the ongoing medical needs of the NICU graduate Recognize the key role of the PCP in providing optimal continuity of treatment by coordinating transition of care from the neonatologist, providing direct medical care and facilitating ongoing care of the infant by subspecialists and other health professionals Review of common screening topics and medical problems of the NICU graduate
Question #1 A premature infant presents to your office for an initial visit after hospitalization. What questions should be asked and topics should be covered in the initial hospital follow up visit then subsequent visits?
Initial Visit NICU course Current medications Medical equipment Home oxygen Pulse oximetry Apnea and bradycardia monitor Ventilator Feeding pump Growth parameters Current weight, length and head circumference as compared to at birth parameters Vital signs Nutrition Formula and kcal/oz Type of feeding (oral versus G-tube) Volume and frequency of feeds Immunization record Neonatal screening Metabolic and newborn screening Cranial imaging Hearing Ophthalmologic Specific problems related to infant Review of NICU discharge summary
Initial Visit Evaluation of progress since discharge including growth Time to listen and address the family s concerns Education for family about Medical diagnoses Cardiopulmonary resuscitation Any medications and/or equipment required in care Review future appointments with subspecialty services , primary care visits and hearing and vision screening
Subsequent Visits Timing depends on infant s medical condition More frequent in the beginning to monitor and establish adequate growth Focus on: Routine primary care (ie, immunizations) General care directed towards NICU graduate (ie, hearing, vision and development screening) Specific medical problems of the infant Consistent care that provides continuity of information and psychosocial support to family
PREP Question #1 A 24-week-premature infant who is now 46 weeks of corrected gestational age is being seen in your office for concerns of decreasing oral intake and poor weight gain. The infant was discharged to home from the neonatal intensive care unit 2 weeks ago weighing 2,400 grams. His medical problems include bronchopulmonary dysplasia that requires diuretics and gastroesophageal reflux that has been treated with omeprazole. The infant was sent home feeding a minimum of 45 mL of premature formula concentrated to 27 calories per ounce orally every 3 hours using a slow flow nipple. At the first office visit 1 week ago, the infant weighed 2,505 grams and was described as feeding slowly but taking the minimum volume of formula daily. Currently, the infant weighs 2,610 g. The mother reports that the infant is feeding 35 to 45 mL of formula every 3 hours. The mother describes her son as waking and hungry every 3 hours, although he often shuts down after 10 minutes of feeding and refuses to take more. The infant does not spit, arch, or turn red with feedings. He passes 2 soft, brown stools daily. The physical examination is otherwise unremarkable. When you observe a feeding, the infant has unlabored respiratory effort and maintains an oxygen saturation of 95%.
PREP Question #1 Of the following, the MOST appropriate approach to help with the poor oral intake is to A. advance the caloric content of the formula B. change to a regular-flow nipple C. consult occupational therapy D. increase the diuretic dosage E. initiate oxygen via nasal cannula
Answer C. consult occupational therapy Consultation with an occupational therapist experienced with premature infants is recommended when feeding problems are identified in discharged premature infants. Feeding problems are 7 times more common in infants born prematurely, with 33% of infants born at less than 26 weeks gestation having continued feeding issues at 30 months corrected gestational age.
Growth At risk for inadequate growth due to increased caloric and nutrient requirements and feeding skills Swallowing problems Oral motor dysfunction Hypersensitivity Delayed feeding skill development Oral aversion problems Plot growth curves and developmental milestones according to corrected age for the first two years of life Initiate corrective measures Changes in the composition, volume, caloric density and mode of feeding Evaluate for contributing conditions (ie, gastroesophageal reflux or feeding disorders) Prompt referral to a feeding specialist and/or nutritionist
Immunization At increased risk for vaccine-preventable infections AAP recommends that medically stable preterm infants should receive full immunization based upon their chronological age consistent with the schedule and dose recommended for full-term infants May have been started in the NICU but delays are common, especially in unstable infants, so it is important to obtain an immunization record Consider RSV prophylaxis with Palivizumab Please see dedicated CCC presentation for more details
PREP Question #2 A 2-year-old boy who has a history of premature birth has been diagnosed with hearing loss. He was born at 28 weeks gestation and required 2 weeks of mechanical ventilation. After discharge, he required home oxygen therapy for 3 months. His mother asks if any medications could have contributed to his hearing loss.
PREP Question #2 Of the following, the medication exposure MOST likely to contribute to hearing loss is A. amphotericin B B. caffeine C. cefotaxime D. chlorothiazide E. furosemide
Answer E. furosemide The AAP Joint Committee on Infant Hearing Year 2007 position statement has identified risk factors for children with congenital or acquired hearing loss that include Neonatal Intensive Care Unit (NICU) hospitalization greater than 5 days, Extracorporeal membrane oxygenation (ECMO) Mechanical ventilation Hyperbilirubinemia requiring exchange transfusion Exposure to ototoxic medications, such as aminoglycosides (gentamicin and tobramycin) or loop diuretics (eg, furosemide) Furosemide-induced ototoxicity can be either transient or permanent. Aminoglycosides appear to potentiate the ototoxic effects of furosemide and, as such, it is recommended that efforts be made to avoid simultaneous use of aminoglycoside and loop diuretics.
Hearing Estimated prevalence of bilateral sensorineural hearing loss is 1-2 per 1000 newborns in the US, but is 10-20 times higher among premature infants Recommended to have automated auditory brainstem response as screening test for hearing Follow up audiological evaluation during the first year of life or sooner if needed is critical to ensure the timely diagnosis on late-onset hearing loss Infants with other risk factors, such as meningitis or cytomegalovirus, should have follow up testing performed soon after discharge
Vision At increased risk for long-term ophthalmologic abnormalities including Retinopathy of prematurity (ROP) Strabismus Reduced visual acuity Myopia Amblyopia Anisometropia Retinal detachment
Neurodevelopment At increased risk for developmental delays and disabilities Motor impairment and/or tone abnormalities Cerebral palsy Learning delay or disability Borderline low-average intelligence quotients (IQs) Autism or autism spectrum disorders Attention-deficit hyperactivity disorder (ADHD) Specific neuropsychological deficits (ie, visual motor integration, executive dysfunction) Behavior problems (ie, internalizing problems, social difficulties) Risk is increased with decreasing gestational age Need to identify and refer at-risk infants for further evaluation and early intervention services Follow up with family to ensure infant is receiving appropriate services specific to developmental needs (PT, OT, ST for feeding, Early Steps)
Psychosocial Issues Bringing home a NICU graduate can be very challenging to parents because of social, financial and psychological stresses Siblings and spouses may feel neglected by the infant s needs Need to screen for these stressors Provide support services Home health nursing visits Early child intervention services Support groups Social work services Child protective services
Car Seats and Beds To prevent morbidity and mortality caused by motor vehicle accidents Premature infants can be at increase risk for cardiopulmonary compromise while in car seats Greater decreases in oxygen saturation More frequent episodes of desaturation, bradycardia and apnea Greatest risk with infants with pre-discharge weights < 2000g Need car seat challenge prior to discharge if at risk Please see dedicated CCC presentation for more details
Dental Increased risk of dental problems Enamel hypoplasia Increased risk for dental carries Delayed tooth eruption Based upon adjusted postmenstrual age between 3-10 months Tooth discoloration Palatal groove Tooth malalignment If prolonged intubation, may develop V-shaped palate, posterior cross bites, deformed incisal edges and missing teeth Recommend first visit by 12 months of age Fluoride exposure via water recommended after 6 months of age
Common Problems of the NICU Graduate
PREP Question #3 A mother brings her 7-week-old infant in for his first health supervision visit after being discharged from the neonatal intensive care unit. The infant was delivered at 31 weeks gestation because of placental abruption. He was intubated for 4 days after delivery and received 3 doses of surfactant for respiratory distress syndrome. He subsequently required oxygen by high flow nasal cannulae for 1 week. He has been in room air since that time and results of his chest radiograph are normal. His mother is worried that her infant has moderate to severe chronic lung disease.
PREP Question #3 Of the following, the MOST appropriate information to provide to the mother is that infants who have chronic lung disease A. are born at less than or equal to 26 weeks gestation B. have chest radiographs with severe fibrosis and hyperventilation C. have received a minimum of 5 days of assisted ventilation D. maintain normal postnatal lung development E. require supplemental oxygen at 36 weeks corrected gestation
Answer E. require supplemental oxygen at 36 weeks corrected gestation The most commonly used definition of the new BPD, currently referred to as chronic lung disease (CLD), is the requirement of oxygen at 36 weeks corrected gestation. With the improvement in ventilator management and the incorporation of therapeutic modalities such as prenatal corticosteroids and surfactants into daily practice, the underlying mechanism for CLD is believed to be an arrest of normal lung development due to premature birth. The radiographs of CLD often do not reveal the fibrosis and hyperinflation that was characteristic of infants diagnosed with BPD in the past.
Respiratory Most common problem is bronchopulmonary dysplasia (BPD) or chronic lung disease (CLD) of prematurity Respiratory disease with requirement of supplemental oxygen at 36 weeks postmenstrual age and persistent abnormalities on chest radiographs At discharge, baseline studies include respiratory and heart rate, blood pressure, oxygen requirement, chest radiograph and echocardiogram to assess for presence of pulmonary hypertension May continue to require supplemental oxygen, medications (ie, diuretics, electrolyte supplements and bronchodilators) and increased caloric needs Most often allowed to outgrow diuretic dose and slow wean of home oxygen Morbidities include acute respiratory exacerbations, pulmonary edema, upper and lower respiratory tract infections, cardiac problems (ie, cor pulmonale and pulmonary hypertension) and growth failure Typically improves by two years of age At risk for reactive airway disease and respiratory infections (ie, RSV and other virus or bacterial infections) Be alert for late-onset sequelae of prolonged intubation (subglottic stenosis)
Apnea of Prematurity Approximately in 25% of premature infants Most outgrow by postmenstrual age of 40 weeks Some will continue to have apnea and may be discharge home on methylxanthine therapy (ie, caffeine) or apnea monitors Timing to discontinue these interventions is multifactorial, usually determined by the subspecialist or NICU follow up clinic
Question #2 What is the second most common cause of childhood blindness?
Retinopathy of Prematurity Second most common cause of childhood blindness Treatment can reduce morbidity Indicated in all infants with birth weight < 1500 g or gestational age less than 31 weeks Also indicated in infants whose clinical course places them at increased risk as determined by the neonatologist Typically presents at approximately 32 weeks gestation Peaks at 38 to 40 weeks Beings to regress by 46 weeks Initial retinal screening 4-6 weeks after birth Additional examinations at intervals of 1-3 weeks until retinal vessels have fully matured
PREP Question #4 You are the primary care physician for newborn twins born at 33 weeks gestation and discharged from the neonatal intensive care unit after a 4-week stay. They required oxygen for 3 days after birth, but little other respiratory support. They were diagnosed with gastroesophageal reflux disease. They have occasional episodes of coughing and gagging without color change. They are otherwise well.
PREP Question #4 Of the following, the BEST advice to give the parents is to place the twins in A. prone sleep position B. side sleep position C. sitting devices, such as car seats, during sleep D. sleep positioners to keep their heads elevated E. supine sleep position
Answer E. supine sleep position Except in a very few instances, supine is the safest sleep position for an infant including those with gastroesophageal reflux. The safest place for an infant to sleep is on a firm, well- fitted mattress in an approved crib, bassinet, or play yard free of other objects and located in the parents room. Current American Academy of Pediatrics recommendations extend beyond Back to Sleep to address other sleep environment factors. Bed sharing, while controversial, is not recommended, and even twins should sleep on separate sleep surfaces.
Sudden Infant Death Syndrome (SIDS) Death of an infant less than one year of age that remains unexplained despite a thorough investigation At greater risk than term infants with a peak risk at 50-52 weeks postmenstrual age No evidence that home apnea monitors decrease the risk Screen at each visit to ensure families are following AAP recommendations of supine (back) sleeping position and ask about location of sleeping
Gastroesophageal Reflux Common in premature infants and in those with CLD, neurological impairment or congenital defects (ie, tracheoesophageal fistulas or diaphragmatic hernias) Monitor for complications including Poor weight gain due to decreased caloric intake Apnea and bradycardia Aspiration Choking Esophagitis Laryngospasms Discomfort
Nectrotizing Enterocolitis Complications Need for ostomy care Malabsorption Intestinal dysmotility Need for parenteral nutrition despite enteral feedings Cholestasis Infections of the ascending biliary tract Biliary calculi Late partial or complete bowel obstruction Short bowel syndrome Dumping syndrome Growth failure Fluid imbalance and electrolyte abnormalities Need for follow up with pediatric surgery and/or gastroenterologist
PREP Question #5 A 6-week-old male infant is brought to your office for a routine visit. He was born at 29 weeks gestational age with a birth weight of 1,250 grams to an 18-year-old mother who did not receive prenatal care until the third trimester. The baby s blood type is O positive and his mother s is B positive. He had neonatal hyperbilirubinemia and received phototherapy for 1 week. He is tolerating his feeds of 22-kcal/oz formula and his weight is now 2,265 grams. His temperature is 37.0 C, his pulse rate is 130/min, respiratory rate is 30 breaths/min, and blood pressure is 80/55 mm Hg. He is alert and in no apparent distress. His sclerae are anicteric, his oral mucosa is pink and moist, his lungs are clear to auscultation, and there is no cardiac murmur or hepatosplenomegaly. The mother is concerned that he looks pale. The following are the results of his complete blood cell count: White blood cell count, 12,500/ L (12.5 109/L) Hemoglobin, 8.5 g/dL (85 g/dL) Mean corpuscular volume, 99 m3 (99 fL) Platelet count, 389 103/ L (389 109/L) Indirect (unconjugated) bilirubin, 1.0 mg/dL (17.1 mol/L)
PREP Question #5 Of the following, the MOST appropriate assessment of this patient would be that he has a A. macrocytic anemia due to folate deficiency B. microcytic anemia due to iron deficiency C. normal hemoglobin for a preterm infant D. normocytic anemia due to ABO incompatibility E. normocytic anemia due to chronic inflammation
Answer C. normal hemoglobin for a preterm infant Normal hemoglobin concentration (Hb) and mean corpuscular volume (MCV) vary with age, highest in the neonate and decline significantly by 1 year of age. During the first week after birth, hemoglobin production decreases by a factor of 10 because of a sudden increase in tissue oxygenation, causing a marked decrease of plasma erythropoietin. This leads to a decrease in Hb known as the physiological anemia of infancy, which occurs at around 6 to 8 weeks of age in full-term infants. In healthy preterm infants, this nadir can be exaggerated and is known as the physiologic anemia of prematurity. Although the term anemia is used, the decrease in hemoglobin is normal and expected; therefore, physiological anemia of infancy is not a true disease state.
Anemia of Prematurity At risk for anemia that occurs earlier and is more severe than physiologic anemia in term infants Nadir for hemoglobin is 7-10 g/dL at 4-8 weeks compared with 11 g/dL at 8-12 weeks in term infants Treatment with iron supplementation (2 mg/kg/day or in multivitamin) results in lower rate of iron deficiency and iron deficiency anemia Less additional supplementation needed if receiving iron-fortified formula versus exclusively breastfeeding Symptomatic infants need red blood cell transfusion
Neurologic Intraventricular hemorrhage (IVH), grades I-IV Posthemorrhagic hydrocephalus occurs in 35% of infants with IVH and risk increases with severity (ie, grades III and IV) Early or late-onset Obstructive, communicating or both Transient or sustained Slow or rapid progression Shunt placement may be required with need for monitoring for malfunction or infection Postmeningitic hydrocephalus Periventricular leukomalacia Ischemic infarction of the white matter, most commonly adjacent to lateral ventricle Seizures Common etiologies: hypoxic-ischemic injury, direct cerebral trauma, intracranial hemorrhage, metabolic abnormalities, malformations and infections
PREP Question #6 An infant develops abdominal distention and bilious vomiting at 36 hours after birth. The 3.9-kg infant was born at 37 weeks of gestation to a mother with type 1 diabetes mellitus. The prenatal course was unremarkable, with negative carrier testing for cystic fibrosis. According to the mother, the infant has been breastfeeding and has had 4 wet diapers and 1 small smear of meconium. Examination reveals an uncomfortable infant with a distended, firm abdomen that is slightly tender to deep palpation. The rectum appears to be externally patent with an anal wink. A radiograph is obtained.
PREP Question #6 Of the following, the MOST likely cause of the infant s findings is A. anorectal malformation B. Hirschsprung disease C. meconium ileus D. neonatal small left colon syndrome E. pneumatosis coli
Answer D. neonatal small left colon syndrome An infant of a diabetic mother is at risk for hypoglycemia, hypocalcemia, polycythemia and neonatal small left colon syndrome.
Question #3 What are some of the common surgical procedures performed on infants in the NICU?
Common Surgical Procedures Surgical bowel resection secondary to necrotizing enterocolitis (NEC) and/or intestinal perforation Gastrostomy tube placement Fundoplication Ventriculo-peritoneal shunts Tracheostomy Cardiac surgeries Umbilical hernia repair due to incarceration Inguinal hernia repair Discuss care for surgical areas and follow up with surgical specialties
References Committee on Fetus and Newborn (2008). Policy statement: Hospital discharge of the high-risk neonate. Pediatrics, 122(5), 1119-1126. Stewart, J. (2014). Care of the neonatal intensive care unit graduate. Retrieved from http://www.uptodate.com. Woods, S. & Riley, P. (2006). A role for community health care providers in neonatal follow-up. Paediatr Child Health; 11(5), 301-302. Andrews, B., Pellertie, M., Myers, P. & Hagerman, J. (2014). NICU follow-up: Medical and developmental management age 0 to 3 years. Neoreviews, 15(4), e123-e132. Sherman, M.P. (2013). Follow-up of the NICU patient. Retrieved from http://emedicine.medscape.com/. AAP PREP Questions
































")