Comprehensive Overview of Asthma and COPD: Insights in 30 Minutes
Explore the multifaceted aspects of Asthma and COPD, including definitions, statistics, patient demographics, diagnostic methods, and treatment guidelines from NAEPP. Gain valuable insights into the prevalence, severity, and management strategies for these respiratory conditions.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Asthma/COPD in 30 minutes Eric L. Olson MD, MSc, FCCP
Definition of Asthma A disease characterized by the following: 1) Airway obstruction that is reversible 2) Airway Inflammation 3) Increased airway responsiveness to a variety of stimuli
* NIH NAEPP 2007 Asthma Guidelines EPR-3
Overview of Asthma Statistics 23 million asthmatics in the United States and rising Every year, asthmatics have 2 million emergency room visits 450,000 hospitalizations (average LOS 3.6 days) > 100,000 lost work/school days Approximately 4000 deaths per year (1.1 per 100,000) > $20 billion in health care costs annually Mortality of asthma more than doubled from 1979 to the mid-1990s has recently plateaued and began to decline slightly
Asthma Patient Demographics US Population = 272.4 Million (US Census, 5/1/99); Asthma Patients = 5.5% Prevalence (ALA, 10/97) Severe persistent 16% 2.2 million African American 6.6% prevalence 3.5 million Hispanic 11.2% prevalence Men 42% Age 18+ y 10 million 67% Moderate persistent 31% 17 million asthma patients Mild 8.9 million Caucasian 4.6% prevalence persistent 25% Women 57% Age 0-17 y 5 million 33% Mild intermittent 28% Asthma Patients Age Severity Race Gender Scott Levin: PDDA, MAT 7/99 Asthma Physician Market Dynamics Study 3/99-10/99 National Center for Health Statistics 1982-1994 Scott Levin: PDDA, MAT 7/99 Morbidity & Mortality Weekly Report 1998
PFT Diagnosis Evidence of airway obstruction FEV1/FVC is reduced below normal (less than 0.70) Acute reversibility of airflow obstruction Is tested by administering a quick-acting bronchodilator (eg, albuterol) with a chamber device or nebulizer, and repeating spirometry 10 to 15 minutes later. An increase in FEV1of 12 percent or more, accompanied by an absolute increase in FEV1of at least 200 mL, can be attributed to bronchodilator responsiveness with 95 percent certainty.
National Asthma Education and Prevention Program (NAEPP 2002) Sx/day Sx/night PF variability PF or FEV1 Severity Daily Meds Preferred Alternatives none < 2 days/week > 80% < 2 nights/month < 20% Step I Mild Intermittent ICS (low dose) Cromolyn, leukotriene (-), nedocromil, theophylline ICS + long-acting agonist Increase ICS (medium dose), add leukotriene (-) or theophylline >2/week but < 1x/day > 80% > 2 nights/month 20-30% Step II Mild Persistent Step III Moderate Persistent Daily > 1 night/week > 30% >60% - <80% High dose ICS + long-acting agonist OS, add leukotriene (-) or theophylline Continual Frequent > 30% < 60% Step IV Severe Persistent Revised 2/2003
Risk Factors for Death Near-fatal and fatal asthma exacerbations may occur in patients with mild, moderate, or severe asthma and the course may be either slow or rapid in onset UpToDate 2015
Acute Respiratory Failure 2 to 4 percent of all patients hospitalized require invasive mechanical ventilation The decision to initiate mechanical ventilation should be based on serial clinical evaluations Factors to consider include: Degree of obstruction, degree of distress, clinical findings, gas exchange and response to treatment Hypercapnea alone is not an indication for intubation Role of noninvasive positive pressure ventilation (NIPPV) in acute asthma exacerbations remains undetermined NIPPV may be reasonable in selected patients prior to intubation
Acute Respiratory Failure Pre-oxygenation can be difficult. Dual therapy with HFNC and NRBM or BMV is optimal. BMV must be done cautiously to avoid hyperinflation Studies suggest that ketamine and propofol have bronchodilatory properties and thus are suitable induction agents for status asthmaticus. Ketamine may be preferable because it aids bronchodilation through both direct and indirect mechanisms and helps to maintain blood pressure. Neuromuscular blocking agents (eg, succinylcholine or rocuronium) are often used unless there is a contraindication Large endotracheal tubes are desirable in order to minimize airway resistance and facilitate aggressive pulmonary toilet Opiate medications should be avoided due to the risk of histamine release exacerbating bronchoconstriction
Acute Respiratory Failure Initial ventilator settings are generally volume controlled. RR from 10 to 12 breaths/min, low tidal volumes 5-8 mL/kg, inspiratory flow up to 80 L/min. Positive end-expiratory pressure (PEEP) is usually initiated at 2-5 cm H2O. Dynamic hyperinflation is a common problem creates intrinsic PEEP (auto-PEEP) and elevates the plateau pressure (Pplat), which place the patient at risk for cardiovascular collapse, barotrauma, and increased work of breathing. Measurement of Pplat is performed during a brief breath-hold at end- inspiration. Intrinsic PEEP is calculated by subtracting any extrinsic (ventilator) PEEP from Pplat.
Acute Respiratory Failure Alternative therapies anesthetic agents (eg, intravenous ketamine, inhaled halothane, isoflurane, enflurane, sevoflurane) have bronchodilating effects Helium-oxygen (heliox) mixtures have been administered in an attempt to decrease the work of breathing and improve ventilation. parenteral beta-agonists are generally avoided except when concern for anaphylaxis or standard therapy has failed. Leukotriene receptor antagonists are an established therapy for chronic asthma, but the role of these medications in acute setting is unclear except in patients whose exacerbation was triggered by ingestion of aspirin or a nonsteroidal anti-inflammatory drug (NSAID).
COPD Characterized by airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases. Exacerbations and comorbidities contribute to the overall severity in individual patients GOLD definition Symptoms include: Dyspnea, chronic cough, chronic sputum production Exacerbations are frequent Spirometry required for diagnosis. FEV1/FVC < 0.70 Third-ranked cause of death in the United States, killing more than 120,000 individuals annually
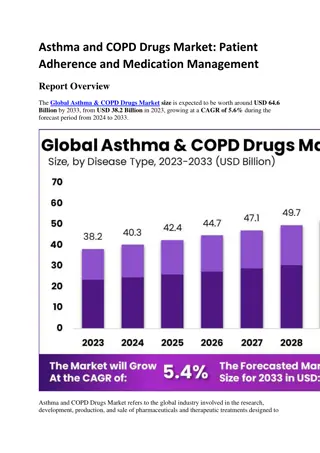
COPD Statistics In 2010, COPD resulted in $49.9 billion in direct and indirect costs . Total costs incurred by COPD patients are approximately $6000 higher than non-COPD patients. 13-14% of COPD patients had a hospital readmission; 41-49% had a readmission within 60 days. The average direct per patient costs for commercially insured increased 6% per year between 2006 and 2009. Treatments that reduce frequency of COPD-related exacerbations are associated with lower COPD-related medical costs. 40% of COPD costs could be avoided by preventing complications and hospitalizations. Individuals with COPD had more days of lost productivity than any other chronic condition.
COPD Global Initiative for Chronic Obstructive Lung Disease GOLD COPD staging uses four categories of severity for COPD, based on the value of FEV1 Stage I Mild COPD FEV1/FVC<0.70 FEV1 80% normal Stage II Moderate COPD FEV1/FVC<0.70 FEV150-79% normal Stage III Severe COPD FEV1/FVC<0.70 FEV130-49% normal Stage IV Very Severe COPD FEV1/FVC<0.70 FEV1<30% normal, or <50% normal with chronic respiratory failure present* * Usually, this means requiring long-term oxygen therapy.
COPD Global Initiative for Chronic Obstructive Lung Disease Stable COPD
COPD Global Initiative for Chronic Obstructive Lung Disease Exacerbations of COPD are defined as acute changes in symptoms (cough, dyspnea and sputum production) beyond what is considered normal variability in a patient and leads to a change in medications
COPD Global Initiative for Chronic Obstructive Lung Disease Treatment options Oxygen- titrated to SpO2 88%-92% Bronchodilators short acting Systemic corticosteroids shorten recovery time, improve lung function and PaO2, reduce risks of early relapse and treatment failure and LOS 40 mg prednisone daily (or equivalent) x 5 days is recommended Antibiotics With all 3 cardinal symptoms of: Dyspnea, sputum volume and sputum purulence Increased sputum purulence + one other cardinal symptom Mechanical ventilation Anti-pseudomonal agents should be used for pt s at risk for colonization or new infection
COPD Risk factors for pseudomonal infection include: recent hospitalization ( 2 days' duration during the past 90 days) frequent administration of antibiotics ( 4 courses within the past year), severe COPD (FEV1 <35 percent of predicted or < 1L) isolation of Pseudomonas aeruginosa during a previous exacerbation colonization during a stable period systemic glucocorticoid use
COPD Noninvasive positive pressure ventilation (NIPPV) improves numerous clinical outcomes and is the preferred method of ventilatory support in many patients with an acute exacerbation of COPD. Avoidance of hypoxemia is critical, even if oxygen therapy worsens hypercarbia Invasive mechanical ventilation is required in patients with respiratory failure who fail NIPPV, do not tolerate NIPPV, or who have contraindications to NIPPV. Careful attention to ventilation parameters is needed in patients with severe obstruction
COPD Several measures have been shown to reduce chronic obstructive pulmonary disease (COPD) exacerbations smoking cessation pulmonary rehabilitation proper use of medications (including metered dose inhaler technique) vaccination against seasonal influenza and pneumococcus Medications, such as tiotroprium and combination inhaled glucocorticoid and long-acting beta agonists(LABA) can help to reduce the frequency of COPD exacerbations roflumilast and N-acetylcysteine (NAC) may also be of benefit
COPD PROGNOSIS Exacerbations of COPD are associated with increased mortality with in-hospital mortality ranges from three to nine percent Mortality following hospital discharge after an exacerbation of COPD is influenced by a number of factors, including age, the severity of the underlying COPD, presence of hypercapnia, and the presence of Pseudomonas aeruginosa in the patient s sputum as described in the following studies: It is estimated that 14 percent of patients admitted for an exacerbation of COPD will die within three months of admission In those with an exacerbation of COPD and a PaCO2of 50 mmHg or more, the 6 and 12 month mortality rates have been reported at 33 and 43 percent, respectively. In a study of 260 patients admitted with a COPD exacerbation, the one year mortality was 28 percent. Independent risk factors for mortality were age, male gender, prior hospitalization for COPD, PaCO2 45 mmHg (6 kPa), and urea >8 mmol/L. Patients hospitalized for a COPD exacerbation who have Pseudomonas aeruginosa in their sputum have a higher risk of mortality at three years than those without (59 versus 35 percent, HR 2.33, 95% CI 1.29-3.86), independent of age, comorbidity, or COPD severity Even if the COPD exacerbation resolves, many patients never return to their baseline level of health