Understanding and Treating Sleep Problems in Children with Autism



Gregory P. Hanley. Ph.D., BCBA-D



. Understanding and Treating
Sleep Problems
of Children with Autism

DataFinch
November, 2014

Important assumption of
Behavior Analysis
:
Sleep problems are viewed
as skill deficits
which can be addressed
by teaching relevant skills
Important assumption of
Behavior Analysis
:
Autism is not a life sentence
of poor sleep
and tired days
Good Sleep
falling asleep quickly
staying asleep through the night
rising without much trouble each morning
not feeling drowsy during the day
Why is Good Sleep Important?
Good sleep is restorative; without it, children are:
more irritable
more easily fatigued
more likely to suffer from unintentional injury
less likely to follow instructions
less likely to learn academic concepts
more likely to engage in problem behavior
(meltdowns, self-injury, aggression, stereotypy)
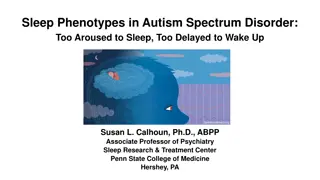
Without good sleep, people with autism may be more
likely to engage in
stereotypy
Why is Good Sleep Important?
Persistent sleep problems in childhood are also
associated with:
childhood and adult obesity
adolescent behavioral and emotional problems
anxiety in adulthood
sleep problems through adulthood
Why is Good Sleep Important?
Children’s sleep problems can lead to:
Maternal malaise and depression
Parental sleep problems
Erosion of the parent’s relationship with each other and
with their children
Sleep problems are prevalent:
35 - 50% of young children
63 - 73% of children diagnosed with autism
Sleep problems are persistent
—
they do not typically remit with time
How Prevalent are Sleep Problems?
Clash between our ancestral history
(encoded in our genes)
and existing cultural practices
we are built to sleep in a particular context
but
we are expected to sleep in a very different context
Why So Prevalent?
Parents are likely to consult with pediatricians
despite only 5 hr of training on average
Treatment Options?
81% of children’s visits to pediatricians, psychiatrists, or
family physicians for sleep problems result in a prescription
for a medication
despite no FDA approval,
no medication labeled for pediatric insomnia,
no (or inconsistent) efficacy signal in literature
Treatment Options?
Behavioral solutions are recommended 22% of
time
(Stojanovski et al., 2007)
but the solutions are relatively weak antecedent-
oriented approaches
(e.g.,
positive
routines
prior to bed)
or not “behavioral” at all (candles and lotion)
Treatment Options?
Common Sleep Problems
Nighttime routine noncompliance
Sleep-interfering behavior
Delayed sleep onset
Night awakenings
Early awakenings
Assumptions Regarding Sleep
•
Behavioral quietude /Falling asleep
are the
behaviors of interest
•
Can be influenced by past and present events
in one’s sleeping environment
–
can be motivated (or demotivated)
–
can become reliant on environmental cues
–
can be affected by other reinforcers for
other behaviors available at night
Looking at falling asleep….
through the lens of a contingency
•
Conduct a contingency analysis:
EO + SD
R
Sr
•
That which is known:
–
Reinforcer (Sr) for falling asleep is
sleeping
•
That which is unknown:
–
Everything else!
Looking at sleep….
through the lens of a contingency
EO
+ SD
Falling Asleep
Sleep
–
What alters the value of sleep as a reinforcer?
Looking at sleep….
through the lens of a contingency
EO +
SD
Falling Asleep
Sleep
–
What signals that the reinforcer is available (and prepares
the body to “consume” the reinforcer), and are those
signals available when the child wakes up multiple times
each night?
Looking at sleep….
through the lens of a contingency
EO + SD
Interfering behaviors
Sr
–
What other behaviors are occurring before and after the
bid good night that are incompatible with falling asleep
(i.e., that do not allow for behavioral quietude)?
Looking at sleep….
through the lens of a contingency
EO + SD
Interfering behaviors
Sr
–
What reinforcers are available for behaviors that are
incompatible with falling asleep?
Looking at sleep….
through the lens of a contingency
EO
+ SD
Incompatible behaviors
Sr
–
What alters the value of these other reinforcers for
behaviors that are incompatible with falling asleep?
Looking at sleep….
through the lens of a contingency
EO +
SD
Incompatible behaviors
Sr
–
What signals that these other reinforcers are available?
How do we assess and treat
children’s sleep problem?
•
Through a general understanding of the
common factors that influence good sleep and
sleep problems
•
Using an
open-ended indirect assessment
to
identify the personal factors influencing the
sleep problem
–
SATT (Sleep Assessment and Treatment Tool)
•
By encouraging parents to develop the
intervention with us
–
we support parents in their implementation of the assessment-
based treatment via phone calls and weekly visits.
A typical case example
Ray
4-year-old-boy with Autism
Hyperactive
Parents tried multiple medications for sleep problems
Social Acceptability Survey (Parents)
Step 1: Develop Ideal Sleep Schedule
Step 2: Routinize Nighttime Routine
Step 3: Optimize Bedroom Conditions
Step 4: Regularize Sleep Dependencies
Step 5: Address Sleep Interfering Behavior
Step 1:
Develop Optimal Sleep Schedule
•
Recognize of age-appropriate sleep amounts
•
Recognize importance of current sleep phase
and
“forbidden zones”
•
Recognize universal tendency to go to bed later
and wake up later
Adapted
from:
Solve Your Child's Sleep Problems,
Richard Ferber, Simon & Schuster, 2006
Age-Based Sleep Averages:
Sleep Scheduling
Cautions:
Difficulty falling asleep, staying asleep, or complying with
nighttime routines may occur if child is expected to be in
bed too long
Difficulty waking up or day time tiredness may be related
to child being in bed for too short of a time
Implication: Select the right sleep total for child
When should the bedtime be scheduled?
Night
Night
Day
Alert
Sleepy
Adapted
from:
Solve Your Child's Sleep Problems,
Richard Ferber, Simon & Schuster, 2006
Night
Night
Day
Alert
Sleepy
Forbidden Zone
Midday Dip in
Alertness
Adapted
from:
Solve Your Child's Sleep Problems,
Richard Ferber, Simon & Schuster, 2006
When should the bedtime be scheduled?
Caution
Putting children to bed during the
Forbidden Zone
will increase the likelihood of
nighttime routine noncompliance,
sleep onset delays
and
sleep interfering behavior
When should the bedtime be scheduled?
We have a tendency to go to bed later and wake up
later because of our 24
.2
hr clock
Artificial light and nighttime activity availability
leads to a 25-hour clock
When should the bedtime be scheduled?
Copied
from:
National Institute of Health (NIH) Sleep and Sleep Disorder’s Teacher’s Guide
At the beginning of sleep treatment:
set the start of the sleep routine slightly
later
than when the child
fell asleep the previous night
Then gradually transition sleep phase earlier
if child falls asleep within 15 min move bedtime 15 min earlier
next night until desired bedtime is achieved
(Piazza et al., 1991)
When should the bedtime be scheduled?
Extreme Sleep Phase Shift?
Consideration
Try
chronotherapy
if sleep phase is more than 4
hours past desirable sleep time:
Move sleep and awake times
forward
by 1 to 2
hours each night (larger leaps can be made with
older children)
Step 2:
Routinize Nighttime Routine
Develop a nighttime routine that occasions
“behavioral quietude”
Try to implement it consistently across nights
Step 2:
Routinize Nighttime Routine
Some emphases prior to bid goodnight
Activities progress from active to passive
Arrange choices on picture schedule
Make gradual changes in fun factor
avoid rich to barren context transition
Exercise/baths earlier in routine
Ambient light gets progressively dimmer
Light snacks without caffeine
Step 3: Optimize Bedroom Conditions
Cooler temperature
Indirect lighting only
Non-undulating noise
Best toys/preferred activities not visible
Nighttime Noncompliance Considerations
Tendency to not follow instructions or resist guidance to,
for example, put on PJs, brush teeth, or get in bed
Solutions:
•
Start routine just prior to natural sleep phase
•
Promote instruction following during the day
–
See steps on handout (e.g., name game, follow through, etc.)
Precursor
=
Responding
effectively to one’s name
=
stopping activity, looking at
teacher, saying, “Yes,” and
waiting until teacher says
something.
Beaulieu et al.,
(2013,
JABA
)
Precursor
=
Responding
effectively to one’s name
=
stopping activity, looking at
teacher, saying, “Yes,” and
waiting until teacher says
something.
Compliance
=
completing
an instruction within 6 s
Nighttime Noncompliance Considerations
Tendency to not follow instructions or resist guidance to,
for example, put on PJs, brush teeth, or get in bed
Solutions:
•
Start routine just prior to natural sleep phase
•
Promote instruction following during the day
–
See steps on handout
•
Arrange big discrepancy in consequences for compliance
vs. noncompliance to routine
–
Avoid DRA with extinction
Step 4:
Optimize Sleep Dependencies
Transitioning from
behavioral quietude to sleep
depends on stimuli associated with falling asleep
Stimuli that set the occasion for sleep must be there through the
night because children wake up often during the night
Optimizing
Sleep Dependencies
Transitioning from behavioral quietude to sleep depends
on stimuli associated with falling asleep
Problems:
Things that occasion sleep are not present when the child
wakes up during the night =
Night Awakenings
Things that occasion sleep are suddenly removed or
inconsistently available =
Sleep Onset Delay
and possibly
sleep
interfering Behavior
Examples
:
TV, radio, books, bottles, “full belly,” presence of
another person, being rocked or patted, lights, fallen stuffed
animal or blanket
Optimizing
Sleep Dependencies
Occasion sleep with things that
don’t require your presence,
can be there in the middle of the night, and
are transportable
(e.g., for vacations or nights at Grandparent’s home)
Optimizing
Sleep Dependencies
Good dependencies
:
pillow,
blanket,
stuffed animal (with bed rails),
pacifier,
sound machine on continuous
Eliminate or fade “bad” ones and replace with “good”
dependencies
Step 5: Address
Sleep Interfering Behavior
SLIB
= Behaviors that interfere with behavioral
quietude necessary for falling asleep
The big four are
:
leaving bed (curtain calls)
crying / calling out
playing in bed or in bedroom
(this includes motor or vocal stereotypy)
talking to oneself
Step 5: Address (SLIB)
Be sure to first properly consider what the likely
reinforcers are for the interfering behavior
Attention / Interaction
Food/drink
Access to TV or toys
Escape/avoidance of dark or of bedroom
Automatic reinforcers
(those directly produced by the behavior)
Part 1
Provide the presumed reinforcer prior to bidding
the child good night
Addressing
SLIB
Part 2
After bid goodnight, eliminate access to presumed
reinforcer following IB
With socially mediated IB, options include:
Extinction, Progressive Waiting,
Time-Based Visiting
,
Quiet-Based Visiting, Quality Fading, or
Bedtime Pass
With automatically-reinforced SLIB, we use:
Relocation of relevant materials
Blocking
Addressing
SLIB
Addressing SLIB
Time-Based Visiting
Visit your child at increasingly larger intervals after the bid
good night and across nights (hopefully before IB occurs);
during visit re-tuck them, bid good night, and leave.
Bed Time Pass
Give your child a
bed time pass
to be used as needed after the bid good night
to have one request granted.
If # of IBs was high before you try this treatment, provide
more than one bed time pass initially and then fade out the
number each night.
Addressing SLIB
Most Preferred
Bedtime pass
Blue
Card
Green
Card
Red
Card
Extinction
Time-based
Visiting
Reinforcement only
if handed a pass
No reinforcement
(period)
Reinforcement
available according
to time
Contingencies
Just prior to bed, the children were allowed
to choose the treatment for each night
Treatments
Treatment-
Correlated
Stimuli
Eliminating Interfering
Behavior
My new favorite:
The Combo+
Time-Based Visiting
and the
Bed Time Pass
with dueling outcomes
+Hand in pass for something now or hold onto pass
and hand in at breakfast for something better
Addressing Night Awakenings
Should be resolved with appropriate sleep schedule
and healthy sleep dependencies
If not, address issues related to temperature, food, light,
noise, incontinence, nighttime reinforcers
If not, we actively teach child to know when it is okay to get
up for the day
usually with moon/sun clocks
Key Considerations for Good Sleeping
sleep schedule
nighttime routines
sleep contexts
sleep dependencies
reinforcers for sleep interfering behavior
Implications
Chronic medication use
is not the solution
for sleep problems
exhibited by children with autism
(or for your sleep problems)
For you to consider…
Start on Friday
Exercise
Avoid caffeine
Reflect on the day and tomorrow
before
you are in bed
and
For you to consider…
Address sleep onset delay by:
1.
Making your bedtime 1 hr. later than usual,
2.
Getting out of bed if not asleep within 10-15 min, and sitting
in chair & read a literary classic for 15 min or until drowsy,
3.
Gradually adjusting sleep and wake times to desired times.
Address difficulties getting out of bed in morning with:
4. Sleep Cycle App
Step 1:
Develop Ideal Sleep Schedule
Step 2:
Routinize Nighttime Routine
Step 3:
Optimize Bedroom Conditions
Step 4:
Regularize Sleep Dependencies
Step 5:
Address Sleep Interfering Behavior
Freedom from sleep problems is
possible and probable with:
Individualized assessment
Individualized and comprehensive treatment:
Thank you.
Good luck with all that you do for all
who you teach and provide care
Contact info.:
Gregory P. Hanley, Ph.D., BCBA-D
Psychology Department
Western New England University
1215 Wilbraham Road
Springfield, Massachusetts 01119
ghanley@wne.edu
It is a treat to be able to speak with you tonight about some of the work that my students and I have been doing over the last few years to develop comprehensive and socially valid interventions for some of the more common problem behaviors associated with autism.
Sleep problems in children with autism are viewed as skill deficits that can be addressed through relevant skills teaching. Good sleep is crucial for children's overall well-being, as it affects mood, behavior, learning, and physical health. Lack of good sleep can lead to irritability, fatigue, unintentional injuries, difficulty following instructions, and engaging in problem behaviors. Addressing sleep issues is essential to prevent long-term consequences such as obesity, behavioral problems, and emotional issues. The prevalence of sleep problems in children with autism is high and persistent, requiring timely intervention.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
. Understanding and Treating Sleep Problems of Children with Autism Gregory P. Hanley. Ph.D., BCBA-D DataFinch November, 2014
Important assumption of Behavior Analysis: Sleep problems are viewed as skill deficits which can be addressed by teaching relevant skills
Important assumption of Behavior Analysis: Autism is not a life sentence of poor sleep and tired days
Good Sleep falling asleep quickly staying asleep through the night rising without much trouble each morning not feeling drowsy during the day
Why is Good Sleep Important? Good sleep is restorative; without it, children are: more irritable more easily fatigued more likely to suffer from unintentional injury less likely to follow instructions less likely to learn academic concepts more likely to engage in problem behavior (meltdowns, self-injury, aggression, stereotypy)
Without good sleep, people with autism may be more likely to engage in stereotypy 16 Number of Hours Slept each Night Mean Baseline Session Rate of Stereotypy 14 r = -.484, p < .05 12 10 8 6 4 2 Jack 0 5 10 15 20 Days
Why is Good Sleep Important? Persistent sleep problems in childhood are also associated with: childhood and adult obesity adolescent behavioral and emotional problems anxiety in adulthood sleep problems through adulthood
Why is Good Sleep Important? Children s sleep problems can lead to: Maternal malaise and depression Parental sleep problems Erosion of the parent s relationship with each other and with their children
How Prevalent are Sleep Problems? Sleep problems are prevalent: 35 - 50% of young children 63 - 73% of children diagnosed with autism Sleep problems are persistent they do not typically remit with time
Why So Prevalent? Clash between our ancestral history (encoded in our genes) and existing cultural practices we are built to sleep in a particular context but we are expected to sleep in a very different context
Treatment Options? Parents are likely to consult with pediatricians despite only 5 hr of training on average
Treatment Options? 81% of children s visits to pediatricians, psychiatrists, or family physicians for sleep problems result in a prescription for a medication despite no FDA approval, no medication labeled for pediatric insomnia, no (or inconsistent) efficacy signal in literature
Baseline Behavioral Intervention 0 mg 0 mg 0 ml Melatonin: 3 mg Clonidine: 0.1 mg Hydroxyzine: 4 ml 07:00 pm Ideal sleep zone Asleep Nap Goal bid goodnight time (09:00 pm) 09:00 pm 11:00 pm 01:00 am 03:00 am Time 05:00 am 07:00 am Goal wake time (08:00 am) 09:00 am Alice 11:00 am 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 Nights
Treatment Options? Behavioral solutions are recommended 22% of time (Stojanovski et al., 2007) but the solutions are relatively weak antecedent- oriented approaches (e.g., positiveroutines prior to bed) or not behavioral at all (candles and lotion)
Common Sleep Problems Nighttime routine noncompliance Sleep-interfering behavior Delayed sleep onset Night awakenings Early awakenings
Assumptions Regarding Sleep Behavioral quietude /Falling asleep are the behaviors of interest Can be influenced by past and present events in one s sleeping environment can be motivated (or demotivated) can become reliant on environmental cues can be affected by other reinforcers for other behaviors available at night
Looking at falling asleep. through the lens of a contingency Conduct a contingency analysis: EO + SD R Sr That which is known: Reinforcer (Sr) for falling asleep is sleeping That which is unknown: Everything else!
Looking at sleep. through the lens of a contingency EO + SD Falling Asleep Sleep What alters the value of sleep as a reinforcer?
Looking at sleep. through the lens of a contingency EO + SD Falling Asleep Sleep What signals that the reinforcer is available (and prepares the body to consume the reinforcer), and are those signals available when the child wakes up multiple times each night?
Looking at sleep. through the lens of a contingency EO + SD Interfering behaviors Sr What other behaviors are occurring before and after the bid good night that are incompatible with falling asleep (i.e., that do not allow for behavioral quietude)?
Looking at sleep. through the lens of a contingency EO + SD Interfering behaviors Sr What reinforcers are available for behaviors that are incompatible with falling asleep?
Looking at sleep. through the lens of a contingency EO + SD Incompatible behaviors Sr What alters the value of these other reinforcers for behaviors that are incompatible with falling asleep?
Looking at sleep. through the lens of a contingency EO + SD Incompatible behaviors Sr What signals that these other reinforcers are available?
How do we assess and treat children s sleep problem? Through a general understanding of the common factors that influence good sleep and sleep problems Using an open-ended indirect assessment to identify the personal factors influencing the sleep problem SATT (Sleep Assessment and Treatment Tool) By encouraging parents to develop the intervention with us we support parents in their implementation of the assessment- based treatment via phone calls and weekly visits.
A typical case example Ray 4-year-old-boy with Autism Hyperactive Parents tried multiple medications for sleep problems
Baseline Treatment 180 Clonidine 0.10 mg Sleep Onset Delay (min) 160 Melatonin 1-3 mg 140 120 Diary 100 Video 80 60 Appropriate Range of Sleep Onset Delay 40 Illness 20 0 120 Clonidine 0.10 mg Interfering Behavior (min) 100 80 Melatonin 1-3 mg 60 40 20 Illness 0 400 Night/Early Waking (min) Clonidine 0.10 mg 350 300 Melatonin 1-3 mg 250 200 150 Illness 100 50 0 14 Clonidine 0.10 mg 12 Total Sleep (hr) 10 8 Illness 6 Goal Range of Sleep 4 Melatonin 1-3 mg Naps 2 Ray 0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100 Nights
Baseline Treatment 180 Clonidine 0.10 mg Sleep Onset Delay (min) 160 Melatonin 1-3 mg 140 120 Diary 100 Video 80 60 Appropriate Range of Sleep Onset Delay 40 Illness 20 0 120 Clonidine 0.10 mg Interfering Behavior (min) 100 80 Melatonin 1-3 mg 60 40 20 Illness 0 400 Night/Early Waking (min) Clonidine 0.10 mg 350 300 Melatonin 1-3 mg 250 200 150 Illness 100 50 0 14 Clonidine 0.10 mg 12 Total Sleep (hr) 10 8 Illness 6 Goal Range of Sleep 4 Melatonin 1-3 mg Naps 2 Ray 0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100 Nights
Baseline Treatment 180 Clonidine 0.10 mg Sleep Onset Delay (min) 160 Melatonin 1-3 mg 140 120 Diary 100 Video 80 60 Appropriate Range of Sleep Onset Delay 40 Illness 20 0 120 Clonidine 0.10 mg Interfering Behavior (min) 100 80 Melatonin 1-3 mg 60 40 20 Illness 0 400 Night/Early Waking (min) Clonidine 0.10 mg 350 300 Melatonin 1-3 mg 250 200 150 Illness 100 50 0 14 Clonidine 0.10 mg 12 Total Sleep (hr) 10 8 Illness 6 Goal Range of Sleep 4 Melatonin 1-3 mg Naps 2 Ray 0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100 Nights
Baseline Treatment 180 Clonidine 0.10 mg Sleep Onset Delay (min) 160 Melatonin 1-3 mg 140 120 Diary 100 Video 80 60 Appropriate Range of Sleep Onset Delay 40 Illness 20 0 120 Clonidine 0.10 mg Interfering Behavior (min) 100 80 Melatonin 1-3 mg 60 40 20 Illness 0 400 Night/Early Waking (min) Clonidine 0.10 mg 350 300 Melatonin 1-3 mg 250 200 150 Illness 100 50 0 14 Clonidine 0.10 mg 12 Total Sleep (hr) 10 8 Illness 6 Goal Range of Sleep 4 Melatonin 1-3 mg Naps 2 Ray 0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100 Nights
Baseline Treatment 180 Clonidine 0.10 mg Sleep Onset Delay (min) 160 Melatonin 1-3 mg 140 120 Diary 100 Video 80 60 Appropriate Range of Sleep Onset Delay 40 Illness 20 0 120 Clonidine 0.10 mg Interfering Behavior (min) 100 80 Melatonin 1-3 mg 60 40 20 Illness 0 400 Night/Early Waking (min) Clonidine 0.10 mg 350 300 Melatonin 1-3 mg 250 200 150 Illness 100 50 0 14 Clonidine 0.10 mg 12 Total Sleep (hr) 10 8 Illness 6 Goal Range of Sleep 4 Melatonin 1-3 mg Naps 2 Ray 0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100 Nights
Social Acceptability Survey (Parents) Table 1 Average (Range) Questions Walter Andy Lou 1.Acceptability of assessment procedures 7 6 7 6.7 (6-7) 2. Acceptability of treatment 7 6 7 6.7 (6-7) 3. Improvement in sleep 7 7 7 7 4. Consultation was helpful 7 6 7 6.7 (6-7) Note: Likert scale: 1 to 7. 1 (not acceptable, not satisfied, not helpful), 7 (highly acceptable, highly satisfied, highly helpful)
Step 1: Develop Ideal Sleep Schedule Step 2: Routinize Nighttime Routine Step 3: Optimize Bedroom Conditions Step 4: Regularize Sleep Dependencies Step 5: Address Sleep Interfering Behavior
Step 1: Develop Optimal Sleep Schedule Recognize of age-appropriate sleep amounts Recognize importance of current sleep phase and forbidden zones Recognize universal tendency to go to bed later and wake up later
Age-Based Sleep Averages: Age 2 3 4 5 6 9 12 15 18 Total Sleep 11 hrs 30 min 9.5 hours 11 hrs 15 min 10 hours 11 hrs 10 hrs 45 min 10 hrs 30 min 10 hrs 9 hrs 45 min 9 hrs 15 min 9 hrs Night Sleep # Naps 1 (2 hrs) 1 (1hr15min) 0-1 10 -11 hours Adapted from: Solve Your Child's Sleep Problems, Richard Ferber, Simon & Schuster, 2006
Sleep Scheduling Cautions: Difficulty falling asleep, staying asleep, or complying with nighttime routines may occur if child is expected to be in bed too long Difficulty waking up or day time tiredness may be related to child being in bed for too short of a time Implication: Select the right sleep total for child
When should the bedtime be scheduled? Alert Sleepy Night Day Night Adapted from: Solve Your Child's Sleep Problems, Richard Ferber, Simon & Schuster, 2006
When should the bedtime be scheduled? Midday Dip in Alertness Forbidden Zone Alert Sleepy Night Day Night Adapted from: Solve Your Child's Sleep Problems, Richard Ferber, Simon & Schuster, 2006
When should the bedtime be scheduled? Caution Putting children to bed during the Forbidden Zone will increase the likelihood of nighttime routine noncompliance, sleep onset delays and sleep interfering behavior
When should the bedtime be scheduled? We have a tendency to go to bed later and wake up later because of our 24.2 hr clock Artificial light and nighttime activity availability leads to a 25-hour clock
Copied from: National Institute of Health (NIH) Sleep and Sleep Disorders Teachers Guide
When should the bedtime be scheduled? At the beginning of sleep treatment: set the start of the sleep routine slightly later than when the child fell asleep the previous night Then gradually transition sleep phase earlier if child falls asleep within 15 min move bedtime 15 min earlier next night until desired bedtime is achieved (Piazza et al., 1991)
Extreme Sleep Phase Shift? Consideration Try chronotherapy if sleep phase is more than 4 hours past desirable sleep time: Move sleep and awake times forward by 1 to 2 hours each night (larger leaps can be made with older children)
Step 2: Routinize Nighttime Routine Develop a nighttime routine that occasions behavioral quietude Try to implement it consistently across nights
Step 2: Routinize Nighttime Routine Some emphases prior to bid goodnight Activities progress from active to passive Arrange choices on picture schedule Make gradual changes in fun factor avoid rich to barren context transition Exercise/baths earlier in routine Ambient light gets progressively dimmer Light snacks without caffeine
Step 3: Optimize Bedroom Conditions Cooler temperature Indirect lighting only Non-undulating noise Best toys/preferred activities not visible
Nighttime Noncompliance Considerations Tendency to not follow instructions or resist guidance to, for example, put on PJs, brush teeth, or get in bed Solutions: Start routine just prior to natural sleep phase Promote instruction following during the day See steps on handout (e.g., name game, follow through, etc.)
BL1 BL2 100 U = 0, p < .05 Precursor = Responding effectively to one s name = stopping activity, looking at teacher, saying, Yes, and waiting until teacher says something. U = 11, p > .05 M % Precursors 80 Individual Children Beaulieu et al., (2013, JABA) 60 40 20 0 100 U = 12, p > .05 U = 4.5, p < .05 M % Compliance 80 60 40 20 0 Control Experimental Control Experimental Group
BL1 BL2 100 U = 0, p < .05 Precursor = Responding effectively to one s name = stopping activity, looking at teacher, saying, Yes, and waiting until teacher says something. U = 11, p > .05 M % Precursors 80 Individual Children 60 40 20 0 100 U = 12, p > .05 U = 4.5, p < .05 M % Compliance 80 60 Compliance = completing an instruction within 6 s 40 20 0 Control Experimental Control Experimental Group































")









 Sleep and")