Evolution and History of Family Medicine: A Comprehensive Overview
 undefined
undefined


F
F
a
a
m
m
i
i
l
l
y
y
P
P
r
r
a
a
c
c
t
t
i
i
c
c
e
e
:
:
P
P
r
r
i
i
n
n
c
c
i
i
p
p
a
a
l
l
s
s
&
&
P
P
r
r
a
a
c
c
t
t
i
i
c
c
e
e
D
r
.
S
y
e
d
I
r
f
a
n
K
a
r
i
m
,
A
s
s
i
s
t
a
n
t
P
r
o
f
e
s
s
o
r
F
a
m
i
l
y
&
C
o
m
m
u
n
i
t
y
M
e
d
i
c
i
n
e
K
i
n
g
S
a
u
d
U
n
i
v
e
r
s
i
t
y





Most of us go through training and practicing medicine without receiving any formal education about the
history of Family Medicine:
We will look at
the birth and growth of Family Medicine, the triumphs,
the dreams, some of the obstacles and challenges found
along the path
as well as the hopes and strategies for the future.
O
b
j
e
c
t
i
v
e
s
To become aware of the history of Family Medicine
To become familiar with the desirable qualities of a
Family Physician
To understand the concepts of Family Medicine,
including its definition
H
i
s
t
o
r
y
o
f
F
a
m
i
l
y
M
e
d
i
c
i
n
e
History does not just
explain the
past
…
also provides the framework for
understanding the present
…..
helps us to
move forward
E
v
o
l
u
t
i
o
n
The age of the General Practitioner
The age of Specialization
Family Medicine as a Clinical and Academic Discipline
At the start of the modern medical profession- every
one was a General Practitioner (GP)
In the 60s and 70s, the age of Specialization, a lot of
court cases and patients dissatisfaction
Realizing the need for a specialist for the whole
person.
In the 1950s the public began to express their dissatisfaction
mainly:
The shortage of physicians
The high cost of medical care
The fragmentation of care
The family practitioner evolved as a specialist to replace the
rapidly disappearing general practitioner in 1950s.
The development of family practice as a specialty occurred at
the end of a long period of decline in general practice.
F
a
m
i
l
y
M
e
d
i
c
i
n
e
a
s
a
C
l
i
n
i
c
a
l
a
n
d
A
c
a
d
e
m
i
c
D
i
s
c
i
p
l
i
n
e
At the start of the 70s, 3-4 years training in Family
Medicine after graduation
In 1982, three years training in family medicine
became a requirement
D
e
f
i
n
i
t
i
o
n
o
f
F
a
m
i
l
y
M
e
d
A
m
e
d
i
c
a
l
s
p
e
c
i
a
l
t
y
o
f
f
i
r
s
t
c
o
n
t
a
c
t
w
i
t
h
t
h
e
p
a
t
i
e
n
t
a
n
d
i
s
d
e
v
o
t
e
d
t
o
p
r
o
v
i
d
i
n
g
p
r
e
v
e
n
t
i
v
e
,
p
r
o
m
o
t
i
v
e
,
r
e
h
a
b
i
l
i
t
a
t
i
v
e
a
n
d
c
u
r
a
t
i
v
e
c
a
r
e
w
i
t
h
e
m
p
h
a
s
i
s
o
n
t
h
e
p
h
y
s
i
c
a
l
,
p
s
y
c
h
o
l
o
g
i
c
a
l
a
n
d
s
o
c
i
a
l
a
s
p
e
c
t
s
f
o
r
t
h
e
p
a
t
i
e
n
t
,
h
i
s
f
a
m
i
l
y
a
n
d
t
h
e
c
o
m
m
u
n
i
t
y
.
The scope is not limited by system, organ, disease entity,
age or sex.
W
H
O
r
e
p
o
r
t
M
a
j
o
r
b
a
r
r
i
e
r
s
t
o
e
q
u
i
t
a
b
l
e
h
e
a
l
t
h
c
a
r
e
-
Unequal access to disease prevention & care
Rising cost of health care
Inefficient health care system
Lack of emphasis on Generalists
’
(Family Medicine)
training
R
e
v
e
r
s
i
n
g
t
h
e
t
r
e
n
d
In 1962 WHO discussed the world wide shortage of family
practitioners in Geneva conference.
The report expressed a need to train GPs to serve as
physicians of first contact with the patient
.
H
o
w
t
o
o
v
e
r
c
o
m
e
t
h
e
s
e
b
a
r
r
i
e
r
s
?
The WHO states, that the best option to overcome these
barriers is to utilize the services of trained Family
Physicians
B
a
r
b
r
a
S
t
a
r
f
i
e
l
d
s
t
u
d
y
:
In a large multicenter study, she found that the central role of FM in
the health care system of a country results in enhanced quality &
cost-effective care
She proved that the health outcome indicators are significantly better
in those countries in which Family Medicine plays a central role in
the HC system
C
o
n
t
r
i
b
u
t
i
o
n
o
f
P
r
i
m
a
r
y
C
a
r
e
t
o
H
e
a
l
t
h
S
y
s
t
e
m
s
a
n
d
H
e
a
l
t
h
Barbara Starfield
There are countless diseases and if all diseases were prevalent
in equal proportion it would be impossible
for a family physician
to
deal
with it.
Fortunately 90% of the symptoms are due to a handful of
diseases, Example; chronic cough
95% of cases of cough over 2 months are due to post nasal drip,
asthma, gerd,chronic bronchitis due to cigarette smoking or ace
induce cough.
Only 6.3% of all cases needs referral.
FAMILY PRACTICE IN UNITED STATES: A STATUS REPORT, JAMA 2002
Studies have shown that family physicians see more
patients than internist
In the office with shorter time, low cost with more patient
satisfaction and equal clinical outcome.
Family medicine ; its core principles and impact on patient care and medical education in united
states. keio medical journal of medicine, 2004
A
m
b
u
l
a
t
o
r
y
m
e
d
i
c
a
l
c
a
r
e
:
a
c
o
m
p
a
r
i
s
o
n
o
f
i
n
t
e
r
n
i
s
t
s
a
n
d
f
a
m
i
l
y
-
g
e
n
e
r
a
l
p
r
a
c
t
i
t
i
o
n
e
r
s
N
E
n
g
l
J
M
e
d
.
1
9
8
0
J
a
n
3
;
3
0
2
(
1
)
:
1
1
-
6
.
Internist:
Spent 18.4 minutes with
the average patient
used laboratory tests in
73 per cent of visits and x-
ray tests in 53 per cent,
family-general
practitioners:
Spent 13.0 minutes with
the average patient
used these studies in 34
and 19 per cent of visits
Health Problems in the community
75% SELF CARE
25% 2
25% GP
2.5
%
T
T
h
h
e
e
N
N
e
e
e
e
d
d
F
F
o
o
r
r
T
T
r
r
a
a
i
i
n
n
e
e
d
d
F
F
a
a
m
m
i
i
l
l
y
y
P
P
h
h
y
y
s
s
i
i
c
c
i
i
a
a
n
n
s
s
The central role of a well trained Family Physician in health care is
well recognized in:
•
Developed countries -- UK, USA and Canada
•
Oil rich countries – Gulf countries ??
•
Developing countries -- ? ? ? ? ?
The need is even greater in all less developed countries.
T
h
e
C
o
r
e
C
o
m
p
e
t
e
n
c
i
e
s
o
f
t
h
e
G
e
n
e
r
a
l
P
r
a
c
t
i
t
i
o
n
e
r
/
F
a
m
i
l
y
D
o
c
t
o
r
Primary care management
Person-centered care.
Specific problem solving skills
Comprehensive approach
Community orientation
Holistic modelling
D
o
m
a
i
n
s
o
f
C
o
m
p
e
t
e
n
c
e
i
n
F
a
m
i
l
y
M
e
d
i
c
i
n
e
(
W
O
N
C
A
)
Primary care management:
- Dealing with unselected problems
- Cover the full range of health problems
- Coordinate care with other health care professionals
- Make health care system available to the patient
- Act as patient
’
s advocate
P
e
r
s
o
n
-
c
e
n
t
e
r
e
d
c
a
r
e
To adopt a person-centered approach in dealing with patients
To use the consultation to bring about an effective doctor-patient
relationship
- Respect patient
’
s autonomy
- To set priorities in partnership with the patient
- Provide long-term continuity and coordinated care
S
p
e
c
i
f
i
c
p
r
o
b
l
e
m
s
o
l
v
i
n
g
s
k
i
l
l
s
Relate decision making processes to the prevalence of illness in the
community
- To apply the clinical information to an appropriate management plan in
collaboration with the patient
- To tolerate uncertainty in dealing with early & undifferentiated
problems
- To intervene urgently when necessary
- To make effective and efficient use of diagnostic and therapeutic
interventions
C
o
m
p
r
e
h
e
n
s
i
v
e
a
p
p
r
o
a
c
h
To manage simultaneously multiple complaints and
pathologies, both acute and chronic
To promote health and well-being
To manage & coordinate health promotion, prevention,
curative care, rehabilitation and palliative care
C
o
m
m
u
n
i
t
y
o
r
i
e
n
t
a
t
i
o
n
To reconcile the health needs of the individual
patients and the health needs of the community
in which they live, balancing with available
resources
H
o
l
i
s
t
i
c
a
p
p
r
o
a
c
h
To use bio-psycho-social models, taking into
account the cultural dimensions
Growing need for Excellent Qualities
Patient care should be the first concern.
Listen to the patient and respond to their concerns and preferences.
Respect patient rights to reach decisions with you about their treatment & care.
Support patients in caring for themselves to improve and maintain their health
.
G
r
o
w
i
n
g
n
e
e
d
f
o
r
E
x
c
e
l
l
e
n
t
Q
u
a
l
i
t
i
e
s
Be honest and open and act with integrity.
Never discriminate un fairly against patient or colleagues.
Never abuse your patient trust in you or public trust in the profession.
Act without delay if you have good reason to believe that either u or your colleague may put
patient s at risk.
1
1
0
0
C
C
s
s
O
O
F
F
F
F
A
A
M
M
I
I
L
L
Y
Y
P
P
R
R
A
A
C
C
T
T
I
I
C
C
E
E
1
1
=
=
C
C
a
a
r
r
i
i
n
n
g
g
/
/
C
C
o
o
m
m
p
p
a
a
s
s
s
s
i
i
o
o
n
n
a
a
t
t
e
e
2
2
= Clinically Competent
= Clinically Competent
3
3
= Cost-effective Care
= Cost-effective Care
4
4
= Continuity of Care
= Continuity of Care
5
5
= Comprehensive Care
= Comprehensive Care
6
6
=
=
C
C
o
o
m
m
m
m
o
o
n
n
P
P
r
r
o
o
b
b
l
l
e
e
m
m
s
s
M
M
a
a
n
n
a
a
g
g
e
e
m
m
e
e
n
n
t
t
7
7
=
=
C
C
o
o
-
-
o
o
r
r
d
d
i
i
n
n
a
a
t
t
i
i
o
o
n
n
o
o
f
f
C
C
a
a
r
r
e
e
8
8
=
=
C
C
o
o
m
m
m
m
u
u
n
n
i
i
t
t
y
y
-
-
b
b
a
a
s
s
e
e
d
d
C
C
a
a
r
r
e
e
&
&
R
R
e
e
s
s
e
e
a
a
r
r
c
c
h
h
9
9
=
=
C
C
o
o
n
n
t
t
i
i
n
n
u
u
i
i
n
n
g
g
P
P
r
r
o
o
f
f
e
e
s
s
s
s
i
i
o
o
n
n
a
a
l
l
D
D
e
e
v
v
e
e
l
l
o
o
p
p
m
m
e
e
n
n
t
t
1
1
0
0
=
=
C
C
o
o
m
m
m
m
u
u
n
n
i
i
c
c
a
a
t
t
i
i
o
o
n
n
&
&
C
C
o
o
u
u
n
n
s
s
e
e
l
l
i
i
n
n
g
g
S
S
k
k
i
i
l
l
l
l
s
s
`
`
w
w
i
i
t
t
h
h
c
c
o
o
n
n
f
f
i
i
d
d
e
e
n
n
t
t
i
i
a
a
l
l
i
i
t
t
y
y
C
C
a
a
r
r
i
i
n
n
g
g
/
/
C
C
o
o
m
m
p
p
a
a
s
s
s
s
i
i
o
o
n
n
a
a
t
t
e
e
c
c
a
a
r
r
e
e
An essential quality in a Family Physician
•
Personal patient centered Care
C
C
l
l
i
i
n
n
i
i
c
c
a
a
l
l
l
l
y
y
C
C
o
o
m
m
p
p
e
e
t
t
e
e
n
n
t
t
•
Only caring is not enough
•
Need for four years training after graduation and
internship
C
C
o
o
s
s
t
t
-
-
e
e
f
f
f
f
e
e
c
c
t
t
i
i
v
v
e
e
C
C
a
a
r
r
e
e
•
In time and money
•
Gate keeper- Use of appropriate resources
•
Use of time as a diagnostic tool
C
C
o
o
n
n
t
t
i
i
n
n
u
u
i
i
t
t
y
y
o
o
f
f
C
C
a
a
r
r
e
e
•
For acute, chronic, from childhood to old age, and
terminal care patients and those requiring rehabilitation
•
Preventive care/ Promotion of health
•
Care from cradle to grave
C
C
O
O
M
M
P
P
R
R
E
E
H
H
E
E
N
N
S
S
I
I
V
V
E
E
C
C
A
A
R
R
E
E
•
Responsibility for every problem a patient presents
with
•
Physical, Psychological & Social
•
Holistic approach with triple diagnosis
C
C
O
O
M
M
M
M
O
O
N
N
P
P
R
R
O
O
B
B
L
L
E
E
M
M
S
S
M
M
A
A
N
N
A
A
G
G
E
E
M
M
E
E
N
N
T
T
•
e.g. Hypertension, Diabetes, Asthma, Depression,
Anemia, Allergic Rhinitis, Urinary Tract Infection
•
Common problems in children and women
C
C
O
O
N
N
T
T
I
I
N
N
U
U
I
I
N
N
G
G
P
P
R
R
O
O
F
F
E
E
S
S
S
S
I
I
O
O
N
N
A
A
L
L
D
D
E
E
V
V
E
E
L
L
O
O
P
P
M
M
E
E
N
N
T
T
•
To keep up-to-date
•
Need for breath of knowledge
C
C
O
O
-
-
O
O
R
R
D
D
I
I
N
N
A
A
T
T
I
I
O
O
N
N
O
O
F
F
C
C
A
A
R
R
E
E
•
Patient’s advocate
•
Organizing multiple sources of help
C
C
O
O
M
M
M
M
U
U
N
N
I
I
T
T
Y
Y
B
B
A
A
S
S
E
E
D
D
C
C
A
A
R
R
E
E
A
A
N
N
D
D
R
R
E
E
S
S
E
E
A
A
R
R
C
C
H
H
•
Care nearer patients’ home
•
Preventive, promotive, rehabilitative and curative care
in patient’s own environment
•
Relevant research within the patient’s own
surroundings
C
C
O
O
M
M
M
M
U
U
N
N
I
I
C
C
A
A
T
T
I
I
O
O
N
N
&
&
C
C
O
O
U
U
N
N
S
S
E
E
L
L
I
I
N
N
G
G
S
S
K
K
I
I
L
L
L
L
S
S
•
Essential for compliance of advice and treatment/sharing
understanding
•
Confidentiality and safety netting
•
Needed for patient satisfaction
•
Involving patient in the management
T
a
k
e
h
o
m
e
m
e
s
s
a
g
e
The principles and competencies required for the practice of
Family Medicine are universal, applicable to all cultures and all
social groups, from richest to the poorest
Promote Family Medicine for the best of our society
T
h
a
n
k
y
o
u
C
o
n
t
i
n
u
i
t
y
o
f
C
a
r
e
–
W
h
y
This build Trust .
Creates a context of healing .
Increases the family physicians and patients
knowledge of each other
Increases the Patient and Doctor satisfaction.
Increase the compliance .
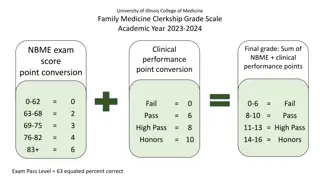
Explore the evolution and history of Family Medicine, from the age of General Practitioners to the emergence of Family Physicians as specialists. Learn about the challenges, triumphs, and future prospects of Family Medicine as a clinical and academic discipline.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Family Practice :Principals & Practice Dr. Syed Irfan Karim, ASSISTANT PROFESSOR FAMILY & COMMUNITY MEDICINE KING SAUD UNIVERSITY
Most of us go through training and practicing medicine without receiving any formal education about the history of Family Medicine: We will look at the birth and growth of Family Medicine, the triumphs, the dreams, some of the obstacles and challenges found along the path as well as the hopes and strategies for the future.
Objectives To become aware of the history of Family Medicine To become familiar with the desirable qualities of a Family Physician To understand the concepts of Family Medicine, including its definition
History of Family Medicine History does not just explain the past also provides the framework for understanding the present .. helps us to move forward
Evolution The age of the General Practitioner The age of Specialization Family Medicine as a Clinical and Academic Discipline
At the start of the modern medical profession- every one was a General Practitioner (GP) In the 60s and 70s, the age of Specialization, a lot of court cases and patients dissatisfaction Realizing the need for a specialist for the whole person.
In the 1950s the public began to express their dissatisfaction mainly: The shortage of physicians The high cost of medical care The fragmentation of care The family practitioner evolved as a specialist to replace the rapidly disappearing general practitioner in 1950s. The development of family practice as a specialty occurred at the end of a long period of decline in general practice.
Family Medicine as a Clinical and Academic Discipline At the start of the 70s, 3-4 years training in Family Medicine after graduation In 1982, three years training in family medicine became a requirement
Definition of Family Med A medical specialty of first contact with the patient and is devoted to providing preventive, promotive, rehabilitative and curative care with emphasis on the physical, psychological and social aspects for the patient, his family and the community. The scope is not limited by system, organ, disease entity, age or sex.
WHO report Major barriers to equitable health care - Unequal access to disease prevention & care Rising cost of health care Inefficient health care system Lack of emphasis on Generalists (Family Medicine) training
Reversing the trend In 1962 WHO discussed the world wide shortage of family practitioners in Geneva conference. The report expressed a need to train GPs to serve as physicians of first contact with the patient.
How to overcome these barriers ? The WHO states, that the best option to overcome these barriers is to utilize the services of trained Family Physicians
Barbra Starfield study: In a large multicenter study, she found that the central role of FM in the health care system of a country results in enhanced quality & cost-effective care She proved that the health outcome indicators are significantly better in those countries in which Family Medicine plays a central role in the HC system Contribution of Primary Care to Health Systems and Health Barbara Starfield
There are countless diseases and if all diseases were prevalent in equal proportion it would be impossible for a family physician to deal with it. Fortunately 90% of the symptoms are due to a handful of diseases, Example; chronic cough 95% of cases of cough over 2 months are due to post nasal drip, asthma, gerd,chronic bronchitis due to cigarette smoking or ace induce cough. Only 6.3% of all cases needs referral. FAMILY PRACTICE IN UNITED STATES: A STATUS REPORT, JAMA 2002
Studies have shown that family physicians see more patients than internist In the office with shorter time, low cost with more patient satisfaction and equal clinical outcome. Family medicine ; its core principles and impact on patient care and medical education in united states. keio medical journal of medicine, 2004
Ambulatory medical care: a comparison of internists and family-general practitioners N Engl J Med. 1980 Jan 3;302(1):11-6. Internist: family-general practitioners: Spent 13.0 minutes with the average patient Spent 18.4 minutes with the average patient used these studies in 34 and 19 per cent of visits used laboratory tests in 73 per cent of visits and x- ray tests in 53 per cent,
Health Problems in the community 75% SELF CARE 25% 225% GP 2.5 %
The Need For Trained Family Physicians The central role of a well trained Family Physician in health care is well recognized in: Developed countries -- UK, USA and Canada Oil rich countries Gulf countries ?? Developing countries -- ? ? ? ? ? The need is even greater in all less developed countries.
The Core Competencies of the General Practitioner / Family Doctor Primary care management Person-centered care. Specific problem solving skills Comprehensive approach Community orientation Holistic modelling
Domains of Competence in Family Medicine (WONCA) Primary care management: - Dealing with unselected problems - Cover the full range of health problems - Coordinate care with other health care professionals - Make health care system available to the patient - Act as patient s advocate
Person-centered care To adopt a person-centered approach in dealing with patients To use the consultation to bring about an effective doctor-patient relationship - Respect patient s autonomy - To set priorities in partnership with the patient - Provide long-term continuity and coordinated care
Specific problem solving skills Relate decision making processes to the prevalence of illness in the community - To apply the clinical information to an appropriate management plan in collaboration with the patient - To tolerate uncertainty in dealing with early & undifferentiated problems - To intervene urgently when necessary - To make effective and efficient use of diagnostic and therapeutic interventions
Comprehensive approach To manage simultaneously multiple complaints and pathologies, both acute and chronic To promote health and well-being To manage & coordinate health promotion, prevention, curative care, rehabilitation and palliative care
Community orientation To reconcile the health needs of the individual patients and the health needs of the community in which they live, balancing with available resources
Holistic approach To use bio-psycho-social models, taking into account the cultural dimensions
Growing need for Excellent Qualities Patient care should be the first concern. Listen to the patient and respond to their concerns and preferences. Respect patient rights to reach decisions with you about their treatment & care. Support patients in caring for themselves to improve and maintain their health.
Growing need for Excellent Qualities Growing need for Excellent Qualities Be honest and open and act with integrity. Never discriminate un fairly against patient or colleagues. Never abuse your patient trust in you or public trust in the profession. Act without delay if you have good reason to believe that either u or your colleague may put patient s at risk.
10 Cs OF FAMILY PRACTICE 1= Caring/Compassionate 2= Clinically Competent 7= Co-ordination of Care 8= Community-based Care & Research 3= Cost-effective Care 4= Continuity of Care 9= Continuing Professional Development 5= Comprehensive Care 6= Common Problems Management 10= Communication & Counseling Skills` with confidentiality
Caring/Compassionate care An essential quality in a Family Physician Personal patient centered Care
Clinically Competent Only caring is not enough Need for four years training after graduation and internship
Cost-effective Care In time and money Gate keeper- Use of appropriate resources Use of time as a diagnostic tool
Continuity of Care For acute, chronic, from childhood to old age, and terminal care patients and those requiring rehabilitation Preventive care/ Promotion of health Care from cradle to grave
COMPREHENSIVE CARE Responsibility for every problem a patient presents with Physical, Psychological & Social Holistic approach with triple diagnosis
COMMON PROBLEMS MANAGEMENT e.g. Hypertension, Diabetes, Asthma, Depression, Anemia, Allergic Rhinitis, Urinary Tract Infection Common problems in children and women
CONTINUING PROFESSIONAL DEVELOPMENT To keep up-to-date Need for breath of knowledge
CO-ORDINATION OF CARE Patient s advocate Organizing multiple sources of help
COMMUNITY BASED CARE AND RESEARCH Care nearer patients home Preventive, promotive, rehabilitative and curative care in patient s own environment Relevant research within the patient s own surroundings
COMMUNICATION & COUNSELING SKILLS Essential for compliance of advice and treatment/sharing understanding Confidentiality and safety netting Needed for patient satisfaction Involving patient in the management
Take home message The principles and competencies required for the practice of Family Medicine are universal, applicable to all cultures and all social groups, from richest to the poorest Promote Family Medicine for the best of our society
Continuity of Care Why This build Trust . Creates a context of healing . Increases the family physicians and patients knowledge of each other Increases the Patient and Doctor satisfaction. Increase the compliance .